

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vaginal intraepithelial neoplasia (VAIN) is a rare entity of lower genital tract premalignant lesion, which incidence has been reported to be 100 times lower than that of cervical intraepithelial neoplasia (CIN) [1]. The prevalence of VAIN, however, has increased steadily over the several decades due to the improved screening methods, such as cervicovaginal cytology and colposcopy, as well as increased awareness of the condition [2]. Moreover, there have been several studies on the malignant potential of high-grade VAIN, which risk of progression to cancer has been shown to range between 2% and 12% [234]. Besides the risk of progression, frequent emergence of recurrence after initial treatment of VAIN has been reported, which could adversely affect the quality-of-life (QoL) of women with VAIN from heightened anxiety.
Despite the growing interest on the clinical importance of VAIN, its natural history, efficacy of treatment, and risk of recurrence or progression are not well understood due to its rarity. Most of the studies have included small numbers of patients (range, 40–160) with short-term follow-up and did not define the outcome measures clearly [456]. In addition, due to the absence of current consensus regarding the optimal management of VAIN, various treatment modalities, including excision, topical agent (e.g., intravaginal 5-fluorouracil [5-FU] cream), laser ablation, or radiotherapy, have been used with varying success rates. In most of those studies, comparison of treatment outcomes between various treatment methods could not be performed owing to the small sample size.
Therefore, in this study, we aimed to evaluate the clinical outcomes of VAIN in a relatively large number of patients and to assess the risk of recurrence and progression to invasive vaginal carcinoma.
MATERIALS AND METHODS
After obtaining institutional review board (IRB) approval of a waiver of informed consent (CGH-IRB-2017-36), an institutional pathology database was searched to identify cases diagnosed as VAIN at Cheil General Hospital and Women's Healthcare Center, Seoul, Korea, from January 1, 2000 to July 31, 2016. Patients with histologically confirmed VAIN of any grade were included in the study analysis. Exclusion criteria were the history of invasive vaginal cancer and the presence of concurrent cervical cancer extending to vagina with VAIN or carcinoma in situ (CIS).
Clinicopathological variables were retrieved from medical records retrospectively, which included age at diagnosis, menopausal state, referral Pap test, high-risk human papillomavirus (HPV) positivity, history of CIN or cervical cancer, treatment modalities, and outcomes. If the patients underwent hysterectomy before the diagnosis of VAIN, the date of hysterectomy and their surgical indications were also obtained. Histologic variables, such as grade, location of VAIN, multifocality of the lesions, and the presence of concurrent CIN, were reviewed.
Treatments for VAIN were categorized as observation, laser ablation with/without topical agent, topical management, surgical excision, and radiotherapy. Intravaginal 5-FU cream was used as topical agent for the initial treatment of VAIN or for the adjuvant treatment after laser ablation.
Primary outcome measures were regression, recurrence, persistence, and progression after treatment for VAIN. Regression or normalization was defined as negative cytology, colposcopic examination, or vaginal biopsy after the initial treatment. Recurrence was defined as regression of VAIN with subsequent redevelopment of histologically confirmed VAIN. Persistence and progression were diagnosed when repeat vaginal biopsy showed the same or higher grade of VAIN, respectively. The time to normalization was computed as the time interval between the start date of treatment (or the date of VAIN diagnosis in observation group) and the date of confirmation of regression.
A χ2 test was used to assess the categorical differences in clinical and histopathological factors. To evaluate the independent risk factors for recurrence or progression, multiple regression analysis was performed. The times to normalization were assessed and compared according to the treatment modality using Kaplan-Meier method and log-rank test. All differences were considered statistically significant at p<0.05. Statistical analysis was performed using SPSS for Windows (version 20.0; SPSS Inc., Chicago, IL, USA).
RESULTS
From January 2000 to July 2016, 576 patients with histologically confirmed VAIN1–3 or vaginal CIS were identified. The median age was 50.3 years (range, 20–81), and 58.3% of the patients were menopaused (Table 1).
Table 1
Clinicopathologic characteristics (n=576)

Two-hundred forty-four patients (42.4%) underwent hysterectomy before the diagnosis of VAIN, and median interval between hysterectomy and VAIN diagnosis was 58.4 months (range, 3.7–469.2). The surgical indications included benign diseases such as leiomyoma or adenomyosis (48.4%), cervical dysplasia (20.1%), cervical cancer (20.5%), and uterine cancer (7.8%). Among 332 patients who did not perform hysterectomy, 131 patients (39.5%) had concurrent CIN lesions. When adding previous and concurrent cervical neoplasia cases, a total of 303 patients (52.6%) had either prior or concurrent cervical neoplasia and 256 patients (44.4%) had no relevant history.
The distribution of histologic grade was as follows: VAIN1 31.1%, VAIN2 45.3%, VAIN3 14.9%, and vaginal CIS 8.7%. Most of the VAIN lesions were detected in the upper third of vagina (96.9%), and multiple lesions were observed in 52.1%. There was a significant correlation between VAIN grade and referral Pap test results (p<0.001; Table 2). While low-grade squamous intraepithelial lesion (LSIL) was the most common Pap finding among VAIN1 cases, high-grade squamous intraepithelial lesion (HSIL) was the most common among women with VAIN3/CIS. HPV test was performed in 523 patients (90.8%), and 444 cases were positive for high-risk HPV types (84.9%). Among high-risk HPV+ patients with available data on HPV genotypes (n=410), other types were more common than HPV16 and HPV18 (72.9% vs. 19.0% and 8.0%). However, as VAIN grade increased, the proportion of HPV16+ cases increased accordingly (p<0.001; Table 2).
Table 2
Referring Pap test results and high-risk HPV positivity in correlation with VAIN grade

ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; CIS, carcinoma in situ; HPV, human papillomavirus; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; SCC, squamous cell carcinoma; VAIN, vaginal intraepithelial neoplasia.
The most common treatment modality was laser ablation with or without topical agent (67%), followed by observation (10.9%), excision (10.8%), and topical agent (9.4%). When excluding 60 patients who did not have sufficient follow-up data, a total of 516 patients were included in the study analysis of treatment outcomes. During the median follow-up period of 44.6 months (range, 2.7–187.5), 71 patients (13.8%) experienced recurrence after regression from initial treatment and 95 patients (18.4%) had persistent or progressive disease (Table 1).
Among 148 VAIN1 patients with available follow-up data, observation was performed in 29.1%, of whom 48.8% obtained regression. Regression rate was higher in laser and excision group compared to observation and topical agent group (75.7% and 77.8% vs. 48.8% and 46.2%, Table 3). Although treatment improved regression rate, however, laser or excision treatment did not shorten the time to normalization (median normalization time in laser and excision group, 6.6 months and 6.5 months vs. 3.7 months in observation group; p=0.095). Among 17 patients who progressed to higher grade after initial treatment (VAIN2 or VAIN3), all of the patients achieved regression with second-line treatment. None of these patients progressed to invasive vaginal cancer.
Table 3
Treatment outcomes according to histologic grade and treatment modalities (n=516)

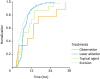
Among VAIN2 patients, 13 patients (5.3%) were followed-up with observation only, and 7 cases (53.8%) regressed spontaneously. Most of the VAIN2 patients were treated with laser therapy (82.4%) and 74.1% of the laser-treated patients achieved regression without recurrence. Patients with VAIN3/CIS were treated in all the cases. Treatment modalities used in VAIN3/CIS included laser ablation (61.3%), excision (32.3%), topical agent (4.8%), and radiotherapy (1.6%) with the following rates of regression: 72.4%, 67.5%, 0%, and 100% (p=0.003). When comparing the regression rate of laser ablation to that of excision, there was no statistically significant difference (p=0.584). When evaluating the time to normalization in VAIN2+ patients, the median times to normalization among patients who underwent laser and excision therapy were 6.4 months and 4.7 months, respectively, which were significantly shorter than 13.0 months in observation group (p=0.006; Fig. 1). Apart from the treatment modality, other factors, including HPV status, previous history of cervical neoplasia, multifocality of VAIN lesions, or hysterectomy state, did not affect the normalization time with statistical significance (p>0.05).
Fig. 1
Kaplan-Meier curve demonstrating the time to normalization in patients with high-grade VAIN according to the treatment modality (p=0.006).
VAIN, vaginal intraepithelial neoplasia.
We also performed subgroup analysis according to the hysterectomy status and its indication (no hysterectomy (group 1) vs. hysterectomy for cervical neoplasia, including CIN and cervical cancer (group 2) vs. hysterectomy for other diseases (group3). Patients who underwent hysterectomy (groups 2 and 3) were significantly older than the patients in no hysterectomy group (55.4 years and 53.4 years vs. 46.6 years, respectively; p<0.001). In addition, there were more VAIN3/CIS cases in group 2 (20.2%) than the other 2 groups (3.4% in group 3 and 7.5% in group 1; p<0.001). However, there was no significant difference in HPV positivity between the groups (p=0.107). Also, the time intervals between hysterectomy and VAIN diagnosis were not significantly different between groups 2 and 3 (72.1 months vs. 87.3 months; p=0.143).
Overall, the regression rate was slightly higher in hysterectomy group (groups 2 and 3) than group 1 (72.6% vs. 64.3%; p=0.046). However, there was no statistically significant difference in regression rate between groups 2 and 3 (70.1% vs. 74.2%; p=0.503). In addition, among VAIN2+ patients, the times to normalization were not different between the 3 groups (6.5 months, 6.3 months, and 6.0 months in groups 1, 2, and 3, respectively; p=0.991). Treatment modalities used in VAIN patients who underwent hysterectomy (groups 2 and 3) included laser ablation (69.4%), topical agent (13.7%), observation (10.5%), excision (5.9%), and radiotherapy (0.5%) with the following rates of regression without recurrence: 78.9%, 50.0%, 52.2%, 84.6%, and 100% (p=0.033). Among VAIN patients who underwent hysterectomy for cervical neoplasia (group 2; n=87), treatment modalities included laser ablation (69.0%), observation (11.5%), topical agent (9.2%), excision (9.2%), and radiotherapy (1.1%). The regression rates were 73.3%, 40.0%, 62.5%, 87.5%, and 100%, respectively.
During the follow-up period, 4 patients developed invasive vaginal cancer with a median time to cancer diagnosis of 21.4 months (range, 5.0–44.8 months). The characteristics of the 4 patients were summarized in Table 4. The 4 cases were all in the patients who were treated for VAIN3/CIS (4/124, 3.2%). Except the second patient whose last response was partial remission after radiotherapy and chemotherapy without further follow-up, the remaining 3 patients achieved complete remission after radiotherapy with or without chemotherapy. The 3 patients are all alive without any evidence of recurrent disease with a median progression-free survival time of 24.2 months (range, 14.9–37.8).
Table 4
Characteristics of 4 patients who progressed to invasive vaginal cancer

Finally, we evaluated the risk of recurrence and progression among the high-grade VAIN cases, including VAIN2, VAIN3 and vaginal CIS. On univariate analysis, hysterectomy state, high-risk HPV positivity, and treatment modality were significantly associated with the risk of recurrence/persistence/progression (p=0.002, p<0.001, and p=0.003, respectively). However, other factors, including menopausal state, multifocal VAIN lesions, and history of cervical neoplasia (prior or concurrent), did not affect the recurrence risk (p>0.05). On multivariate analysis, high-risk HPV positivity and treatment method other than laser or excision were found to be independent predictive factors for VAIN recurrence and progression (p=0.003 and p=0.001; Table 5). Among patients with high-grade VAIN who underwent hysterectomy (groups 2 and 3), multivariate analysis for the risk of recurrence and progression showed similar results. High-risk HPV positivity (odds ratio [OR]=4.50; 95% confidence interval [CI]=1.46–13.88; p=0.009) and treatment modality (OR=3.10; 95% CI=1.48–6.51; p=0.003) were identified to be independent predictive factors for recurrence/persistence/progression.
Table 5
Multivariate analysis on the risk factors for recurrence/persistence/progression after treatment of high-grade VAIN

DISCUSSION
The present study evaluated the clinicopathologic characteristics of VAIN and assessed the risk of recurrence and progression to vaginal cancer. To our knowledge, this is the largest study on the clinical outcomes of VAIN to date.
Overall, response to initial treatment of VAIN was as follows: regression 81.6% (421/516), persistence 13.8% (71/516), and progression to higher grade 4.7% (24/516). Among 421 patients who initially achieved regression, 71 patients (16.9%) developed recurrence. There was no significant difference in the regression and recurrence rate among different VAIN grades. In VAIN1 patients, observation was performed in 29.1% of the cases and 48.8% obtained regression without recurrence. In VAIN2+ patients, treatment modalities included observation (3.5%), topical management (6.5%), laser ablation (75.3%), excision (14.1%), and radiotherapy (0.5%) with the following rates of recurrence/progression: 46.2%, 62.5%, 26.4%, 32.7%, and 0%, respectively. There were 4 patients who progressed to invasive vaginal cancer during the follow-up period, and all of the patients were initially diagnosed as VAIN3/CIS.
In our study, observation was performed in a relatively small proportion of VAIN1 patients (29.1%) in comparison with other studies [67]. This was caused by the retrospective nature of the study, in which the treatment was decided at the responsible physician's discretion. Among the VAIN1 patients who were followed with observation only, 25.6% of the patients progressed to the higher grade. However, similar to the previous studies, none of these patients developed vaginal cancer. Although the risk of progression to cancer is minimal in VAIN1, continuous surveillance is still warranted due to the frequent emergence of recurrence and progression even after treatment with laser or excision (24.3% or 22.2%, respectively).
In patients with VAIN2 or VAIN3/CIS, treatment with laser or excision was shown to decrease the recurrence and progression risk significantly and shorten the time to normalization compared to the observation. On multivariate analysis, treatment status was independently associated with recurrence and progression risk. Our finding was inconsistent with previous studies in which recurrence rates were not shown to differ by treatment type [467]. The disagreement might be partly due to the difference in the sample size between the studies. Among various treatment modalities, laser and excision were demonstrated to be superior to topical management. Between the laser ablation and excision, there was no statistically significant difference in the recurrence rates (26.4% vs. 32.7%; p=0.347). When considering the multifocality of VAIN lesions, however, treatment outcomes were shown to differ between laser and excision group. In patients with multifocal lesions, laser ablation was more effective in reducing the recurrence/persistence/progression rate compared to excision (28.2% vs. 54.5%; p=0.012). In contrast, excisional treatment showed a tendency of lower recurrence risk than laser therapy in unifocal cases (16.7% vs. 23.6%; p=0.420). Our finding corresponded with other studies which demonstrated a trend of improved cure rate with excisional therapy, such as upper vaginectomy, for high-grade lesions [23]. Although it failed to show a statistical significance, excisional treatment may be more suitable for high-grade unifocal lesions, especially when there is a possibility of occult stromal invasion in the vaginal cuff [89].
The treatment efficacy of topical agents seemed to be minimal in our study. The treatment outcomes of topical management with intravaginal 5-FU cream were not significantly different from those of observation only. In addition, its adjuvant role following laser ablation was not demonstrated. Among high-grade VAIN patients, there was no significant difference in the treatment outcomes between laser and laser with 5-FU cream group (regression rate, 75.0% vs. 73.1%; p=0.744). Although older studies reported that 5-FU cream showed comparable treatment outcomes with laser ablation in selected cases [1011], more recent studies have reported a trend of inferior treatment efficacy, which results were further supported by our study [23].
In addition to the treatment type, high-risk HPV positivity was identified as an independent risk factor for recurrence and progression. Our finding further supports previous studies on the association of high-risk HPV status with the risk of VAIN development and recurrence [51213]. High-risk HPV was positive in 84.9% among VAIN patients with available HPV test results, which positive rate was comparable to other studies reporting the positivity in the range of 70%–95%. Among various genotypes of high-risk HPV, HPV16 and HPV18 have been reported to be the most prevalent types in VAIN lesions [1415]. However, most of these studies included few cases from Asia. In our study, various types other than HPV16 and HPV18 were more common, although the top 5 most common genotypes were HPV16 (17.3%), HPV53 (7.9%), HPV18 (7.7%), HPV58 (4.9%), HPV52 (4.3%), and HPV56 (4.3%) when the frequency analysis was limited to the VAIN cases with data on the specific HPV genotypes. A recent Chinese study also reported the predominant HPV types as HPV16, HPV33, HPV53, HPV18, and HPV58, suggesting the geographical difference in the distribution of HPV types [16]. However, as VAIN grade increased, the proportion of HPV16+ cases increased accordingly (p<0.001). In vaginal CIS cases, HPV16 was positive in 40.5% which prevalence was significantly higher than 6.9% in VAIN1. Although our study suggested the clinical importance of high-risk HPV status in the management of VAIN, the current study was limited since the post-treatment HPV test results were not available. Further studies on the distribution of specific high-risk HPV genotypes and the role of HPV test in the post-treatment surveillance need to be performed.
Apart from the treatment modality and HPV status, other factors, including previous history of cervical neoplasia, multifocality of VAIN lesions, or hysterectomy state, did not affect the risk of recurrence and progression with statistical significance in our study (p>0.05). Other factors which have been suggested as risk factors for recurrence included multifocality of the lesions, younger age, and higher grade [217]. The conflicting results might be originated from the different study population, various treatment methods, and unstandardized outcome measures.
Our study is limited due to the retrospective nature of the study, which might cause a selection bias since the decision on the treatment modality could not be controlled and it depended on the physician's discretion. Nevertheless, our study added a meaningful insight on the clinical outcomes of VAIN management, providing a comprehensive analysis on a relatively large study population.
In conclusion, VAIN is at high-risk of recurrence and progression, but the progression to vaginal cancer was limited to VAIN3/CIS cases (3.2%). The risk factors for recurrence and progression included treatment type and high-risk HPV positivity. Both laser ablation and excision therapy demonstrated relatively high regression rates compared to observation and topical management. However, laser ablation seemed to be better for multifocal lesions, whereas excision might be more suitable for high-grade unifocal lesions, especially when the occult stromal invasion is suspected. Whatever the treatment method is used, lifetime surveillance is recommended.
 XML Download
XML Download