

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Although the majority of cases of endometrial cancer with endometrioid histology are diagnosed at an early-stage and have an excellent prognosis, women with advanced-stage tumors have a significantly poorer survival [1]. The presence of lymph node metastases is one of the most important prognostic factors for endometrioid endometrial cancer (EEC) [2]. The possible role of lymph node dissection has been investigated by numerous studies in the last years [3456], but controversy still remains regarding the indications, anatomic extent, and therapeutic value of this procedure [78].
The National Comprehensive Cancer Network (NCCN) Panel as well as the European Society for Medical Oncology (ESMO)-European Society of Gynaecological Oncology (ESGO)-European SocieTy for Radiotherapy & Oncology (ESTRO) Consensus Conference on Endometrial Cancer have recently recommended a selective and risk-adapted performance of lymphadenectomy, in order to avoid systematic over-treatment [89]. On the other hand, omission of nodal dissection in patients at risk of lymph node metastasis may result in an inability to specifically tailor post-operative treatment. Sentinel node identification has been recently proposed as an alternative technique to reduce the morbidity of nodal dissection, maintaining the information regarding the presence of nodal spread of disease [1011]. This new and less invasive approach is gaining increasing popularity and is progressively replacing complete nodal staging at many institutions worldwide, mainly for low- or intermediate-risk disease.
It is important to note that patients with stage IIIC EEC (according to International Federation of Gynecology and Obstetrics; FIGO) have been reported to have a variable 5-year disease-specific survival (DSS), ranging from 44% to 77%, [12131415]. These wide ranges suggest that there is considerable heterogeneity among lymph node positive patients, and that the staging system does not reflect the survival impact of all the possible prognostic variables. To date, owing to the difficulty of collecting large series of women with lymph node positive EEC, data regarding the prognostic factors in these patients are very limited [1516].
The improvement of risk assessment in lymph node positive EEC patients, beyond the current FIGO staging definition, however, should be an argument for urgent action, given the growing implementation of sentinel lymph node (SLN) mapping. The absolute number of metastatic lymph nodes, indeed, has recently emerged as an important prognostic factor in several types of malignancies [12171819]. It is therefore possible that the use of SLN biopsy alone, without a systematic pelvic and para-aortic lymphadenectomy, may not be completely adequate to capture the information regarding the real number of involved nodes.
The aim of this study was to assess whether patients with only 1 positive node have a different prognosis compared to those with >1 positive node.
MATERIALS AND METHODS
We performed a retrospective evaluation of all consecutive patients who underwent primary surgical staging for EEC at 7 Italian gynecologic oncology referral centers between January 2004 and December 2014.
The primary aim of our study was to compare patients with 1 positive pelvic node vs. those with >1 positive pelvic node in terms of survival outcomes. The relationship between other important clinical-pathologic factors and disease-free survival (DFS) and DSS was also assessed.
The Institutional Review Boards (IRB) of participating centers approved this study; all patients included in the present analysis gave written consent to data collection and to the use of personal records for health research. A standardized database was used to collect data systematically abstracted from the oncological datasets of each Institution; these are research-quality forms, which are regularly updated by trained residents in a prospective fashion.
In particular, we collected data on: patient- (age, American Society of Anesthesiologists [ASA] score), disease- (histologic grade, myometrial invasion,; lymph vascular space invasion [LVSI], tumor size, cervical involvement, presence or absence of pre-operative or intra-operative evidence of extra-uterine disease, number of metastatic lymph nodes, pattern of lymph node involvement), and treatment-related characteristics (surgical approach, type of lymphadenectomy performed, adjuvant therapy). Follow-up data were gathered until the end of 2017.
All patients underwent total hysterectomy, bilateral salpingo-oophorectomy, and pelvic±para-aortic lymphadenectomy. Lymphadenectomy was performed based on standard international guidelines. The surgical procedures were performed by open surgery, laparoscopy or robotic approach, according to surgeon's discretion, institutional facilities and clinical characteristics. The anatomic extent of lymphadenectomy, however, varied based on institutional policy and patient's characteristics [20].
Only patients with histologically proven FIGO stage IIIC1 EEC at final pathology and at least 12 lymph nodes harvested were included in the present analysis.
The following patients were considered non-eligible for study inclusion: 1) non-endometrioid histologies; 2) less than 12 lymph nodes harvested; 3) FIGO stage IIIC2; 4) pre- or intra-operative evidence of extra-uterine disease (including adnexal or vaginal involvement, bulky or suspicious nodes, FIGO stage IV); and 5) patients not treated with upfront surgery.
Tumor size was evaluated by the pathologist and measured on the largest tumor diameter. For the pattern of lymph node involvement we used the same definitions as in breast cancer: a micrometastasis was defined as a single focus of metastatic disease per lymph node measuring ≤2 mm; a macrometastasis was defined as metastatic disease measuring more than 2 mm; extranodal tumor extension was defined as cancer perforating the lymph node capsule and extending into the perinodal tissue [21]. All pathologic evaluations were performed by dedicated gynecologic pathologists. When the size of the lymph-node metastasis was not delineated in the pathology report and the terms ‘micrometastasis’ and ‘macrometastasis’ were not used, pathology slides were reviewed at each participating center and a determination was made based on the histopatologic re-evaluation.
1. Statistical analysis
Statistical analysis was performed with SPSS statistical software version 21.0 for Windows (IBM Corp., Armonk, NY, USA) and with STATA/IC 13.0 for Windows (StataCorp LP, College Station, TX, USA). Categorical variables were reported as absolute number and percentage. Continuous variables were reported as median and range or as mean and standard deviation (SD). DFS was calculated from the date of surgery to either the last follow-up or the date of recurrence. DSS was calculated from the date of surgery to either the last follow-up or the date of death from EEC. The relative importance of variables as independent predictors of DFS and DSS was analysed with the multivariate Cox proportional hazard regression: to correct for possible confounders, all parameters found to have a p<0.2 at univariate analysis were included into the multivariable Cox regression model. Adjusted hazard ratios (HRs) and 95% confidence interval (CI) for prognostic factors were estimated.
Survival analysis for patients with 1 vs. >1 metastatic lymph node was performed. Furthermore, additional survival analyses were planned for variables, if any, which resulted independent predictors of DFS and/or DSS at multivariate Cox regression analysis. Survival rates were estimated by the Kaplan-Meier method. The log-rank test was used to compare survival curves. Patients known to be still alive or lost to follow-up at the time of analysis were censored at their last follow-up. All p-values were two-sided, and statistical significance was set at p<0.05.
To correct for the possible imbalance between the group of patients with 1 vs. >1 positive node, we also repeated our evaluation with the technique of propensity score (PS) matching. The PS method allows comparisons between patient groups that are similar on all already-known confounders. The PS for an individual is defined as the probability of having been exposed to a condition based on variables measured at or before the time of treatment. To generate PS, a non-parsimonious logistic regression model that incorporated variables that predict the risk of recurrence was developed, with the presence of 1 or >1 metastatic node as the dependent variable. The choice of covariates potentially relating to the exposure arm included in the PS model was based on univariate analysis and clinical knowledge. Patient age, surgical approach, grading, LVSI, tumor diameter, myometrial invasion, and cervical involvement were included in the PS model. Women in the 1 metastatic node group were matched with women in the >1 metastatic node group in a 1:1 ratio, thereby creating pairs of cases. The success of matching was assessed for each variable using standardized differences. A successful balance was inferred if the residual imbalance for all confounders was <10%.
RESULTS
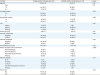
A total of 140 patients met the inclusion criteria and were enrolled in the present analysis. Patient, tumor- and treatment-related characteristics are presented in detail in Table 1. Median patients' age was 62 years. More than one third of patients (37.9%) underwent minimally invasive surgical staging. Forty-eight patients (34.3%) underwent combined pelvic and para-aortic lymphadenectomy. The median number of lymph nodes removed was 22 (range, 12–105), and no significant difference (p=0.06) was detected between open (mean±SD, 26.6±13.7) vs. endoscopic approach (22.8±7.6) in terms of lymph nodes harvested, although a tendency towards a higher nodal yield was observed among women who underwent open surgery. Sixty-five patients (46.4%) presented with only one positive node and 75 patients (53.6%) had more than one metastatic lymph node; these two subgroups were homogeneous for the main patient and disease characteristics (Table 2).
Table 1
Patient, tumor- and treatment-related characteristics

Values are presented as number (%) or median (range).
ASA, American Society of Anesthesiologists; AWD, alive with disease; CT, chemotherapy; DID, dead of intercurrent disease; DOD, dead of disease; LVSI, lymph vascular space invasion; NED, no evidence of disease; PALX, para-aortic lymphadenectomy; PLX, pelvic lymphadenectomy; RT, radiation therapy.
*Includes metastasis to inguinal lymph nodes, intra-peritoneal disease, or lung, liver, or bone.
Table 2
Patient, tumor- and treatment-related characteristics by number of positive nodes
A total of 110 patients (78.5%) were treated with adjuvant chemotherapy, and all of them have been documented as having received a platinum-based regimen. In particular, 66 patients (47.1%) received combined/sequential adjuvant radiotherapy and platinum-based chemotherapy. During a median follow-up time of 31 months (range, 1–177), 49 patients (35%) experienced a relapse and 30 (21.4%) died of disease (Table 1). Mean DFS and DSS were 38.8 months (95% CI=32.1–45.4 months) and 41 months (95% CI=34.7–47.4 months), respectively.
At uni- and multi-variate analysis, only the presence of more than one metastatic lymph node was independently associated with both recurrence and mortality (Tables 3 and 4).
Table 3
Cox regression analysis of factors predicting recurrence

Table 4
Cox regression analysis of factors predicting mortality

Multinomial logistic regression (post hoc analysis) of histopatologic characteristics predicting multiple metastatic lymph nodes is presented in Table 5. After multivariable adjustment for possible confounders, lymph node metastasis >2 mm in size resulted as the only independent factor associated with multiple positive nodes (p=0.02).
Table 5
Multinomial logistic regression analysis of histopatologic characteristics predicting multiple metastatic lymph nodes

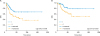
Kaplan-Meyer curves showing the association of the number of metastatic lymph nodes with the risk of relapse and death from disease are presented in Fig. 1. In particular, DFS was significantly longer (p=0.008) in patients with only 1 metastatic lymph node (mean 46.2 months; 95% CI=35.3–57.2 months) compared to those with more than one metastatic lymph node (mean 33.2 months; 95% CI=23.9–42.4 months). Similarly, patients with only one metastatic lymph node had a significantly longer DSS (p=0.009) compared to patients with more than one metastatic lymph node: specifically, mean DSS was 49.6 months (95% CI=39–60.2 months) for the former and 38.2 months (95% CI=29.2–47.1 months) for the latter.
Fig. 1
Survival curves according to the number of metastatic lymph nodes.
DFS, disease-free survival; DSS, disease-specific survival.
The results of the PS-matched analysis are provided in the Supplementary Table 1. The presence of >1 metastatic node remained associated with the risk of recurrence also after propensity-matched analysis (odds ratio=2.40; 95% CI=1.09–5.30; p=0.03).
DISCUSSION
The present study shows that, when the disease is macroscopically confined to the uterus, EEC patients with multiple positive pelvic lymph nodes have a significantly worse prognosis, compared to subjects with only a single positive node. The present findings provide a deeper insight in the knowledge of EEC with pelvic lymphatic spread and demonstrate that the extension of nodal dissemination is associated with disease recurrence.
Our results appear in agreement with the observation of a wide survival range for women with stage IIIC EEC, thus suggesting a considerable heterogeneity in this subset of patients. In this setting, an adequate risk-based stratification may allow a more accurate assessment of prognosis and should foster specific efforts to identify a more tailored treatment. The therapeutic paradigm for EEC patients with lymph node metastases has shifted in recent years to a multimodal approach including surgery, chemotherapy, and radiation therapy [22]. Due to the paucity of cases, however, there is still debate regarding the best therapeutic options in these patients. In particular, controversies exist around the possible treatment strategies for patients with lymph node metastases detected with SLN mapping and/or not submitted to systematic pelvic and para-aortic lymphadenectomy. Recently, Touhami et al. [23], have reported that the risk of metastasis in non-SLNs is 34.8% when SLN is positive, and that this incidence increases with the size of the SLN metastasis. Moreover, it has to be taken into account that the routine performance of ultrastaging on SLNs increases the detection of metastatic disease, in the form of micrometastases and isolated tumor cells, and that the best therapeutic approach in these specific circumstances is still under investigation [24]. Of note, in the present study we found that the size of lymph node metastasis (<2 mm vs. >2 mm) is not associated with disease recurrence and survival. A more specific analysis, however, revealed that the presence of macrometastases was the only independent predictor of multiple pelvic node involvement.
The main objective of our study was to define the prognostic impact of the number of pelvic metastatic nodes in patients with disease macroscopically confined to the uterus. This clinical context is that compatible with the sentinel node mapping. We also decided to exclude stage IIIC2 patients in order to avoid the possible bias of including women with higher stage disease. Considering the findings of the present analysis, it is logical to ask whether the use of SLN biopsy alone, without a pelvic and para-aortic lymphadenectomy, could allow an adequate risk-based stratification of patients with metastatic nodes and/or with lymph node metastases >2 mm in size. It is also possible to hypothesize that SLN technique and systematic lymphadenectomy could not be considered as mutually-exclusive. While sentinel node mapping has been demonstrated as a reliable tool to assess lymphatic spread both in low-risk and high-risk patients [1125], future studies could identify a subset of cases in whom a combination of the 2 approaches may provide the best benefit to the patient.
Previous studies have indicated that lymph node ratio (defined as the ratio between the number of positive nodes and the total number of lymph nodes removed) is associated with prognosis in stage IIIC EEC [2627]. Although these findings are consistent with the results of the present study and underline the relationship between the extent of nodal involvement and survival outcomes, we highlight that lymph node ratio is determined not only by the burden of nodal disease but also by the total number of nodes harvested. In contrast, the absolute number of positive nodes may represent a more direct and independent measure of lymph node involvement (since it is less affected by the extent of lymphadenectomy).
The retrospective design with the possible selection and reporting biases likely represents the main limitation of the present study. Nevertheless, the oncological databases from which our data have been collected, are prospectively maintained by dedicated physicians in all the Institutions involved. As a possible further limitation, it has to be considered that the anatomical extent of lymphadenectomy (i.e. pelvic±para-aortic) varied over time, depending on institutional policies and international guidelines. It should be underlined, however, that all patients included in the present analysis had at least 12 pelvic nodes harvested, and all the procedures were performed by gynecologic oncologists in oncological referral centers. Another possible limitation of the study is that the sample size was not calculate a priori. Due to the low incidence of nodal metastases in patients with endometrioid histology, no paraaortic involvement and no macroscopic extra-uterine spread, a consecutive series of 140 patients with only pelvic node metastasis is likely to be statistically adequate for the study purposes.
Our study poses some questions that can be summarized as follows: 1) Which are the possible therapeutic implications of the finding that multiple pelvic nodal metastases in stage IIIC1 EEC portend a worse prognosis? Is this cohort of patients suitable for a more aggressive and individualized treatment? And which kind?; 2) Is it justified to perform full lymphadenectomy in patients with a positive SLN? If the positive SLN is identified at definitive histology, would a re-operation for a full lymphadenectomy be justified? These and other questions should be answered in the setting of possible future prospective multicenter trials.
In conclusion, our study provides evidence that the absolute number of metastatic pelvic nodes (1 vs. >1) is a strong independent parameter to predict disease recurrence and mortality. Moreover, our data suggest that stratifying patients with IIIC1 EEC according to the actual number of positive nodes allows a more accurate assessment of prognosis. This could represent the possible basis for better tailoring and individualization of surgical treatment and/or adjuvant therapy.
 XML Download
XML Download