

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
At the Rare Ovarian Tumors Conference held in Tokyo 2015 prior to the 5th Ovarian Cancer Consensus Conference of the Gynecologic Cancer InterGroup (GCIG), young investigators addressed an update on recent advances in the knowledge and treatment of rare ovarian cancers, including low-grade serous, mucinous, and clear cell carcinomas of the ovary.
LOW-GRADE SEROUS CARCINOMA (LGSC)
1. Background
Recent studies have identified low-grade and high-grade serous carcinomas (HGSC) as 2 distinct entities and the new edition of the World Health Organization (WHO) classification, published in 2014, has adopted this binary classification. Traditional 3-tiered grading of serous carcinoma had limited significance in terms of prognosis, management strategies, and biology, whereas the 2-tier system well reflects the molecular pathogenesis, clinicopathologic features, and epidemiology. These criteria for grading, established by Malpica et al. [1], have now been widely accepted. LGSC defined as serous carcinoma composed of uniform cells showing mild to moderate nuclear atypia and fewer mitotic figures (12 or less, and in general, mostly 2 to 3 per 10 high power fields [HPFs]), is a rare neoplasm accounting for 5%–10% of all ovarian serous carcinomas. Very rarely, LGSC may give rise to HGSC or undifferentiated carcinoma [2].
2. Understanding the difference between LGSC and HGSC
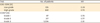
LGSC and HGSC differ distinctly in presentation, histogenesis, treatment strategies, and outcome (Table 1). The former is characterised by younger age, and paradoxically, poor response to conventional chemotherapy [34567]. It is mitotically less active, and immunohistochemically shows a low Ki-67 labelling index. Since TP53 is typically intact, TP53 immunostaining shows wild-type pattern, aiding distinction of LGSC from HGSC. KRAS, BRAF, or ERBB2 mutations are common in contrast to HGSC, which is characterised nearly uniform loss of TP53 function due to mutation or deletion, associated with significant chromosomal instability and decreased overall survival (OS) [8].
Table 1
Differentiating low- and high-grade serous carcinoma

| Feature | LGSC | HGSC | Source |
|---|---|---|---|
| Nuclear atypia | Uniform | Pleomorphic | [1] |
| Form | Oval/round | Variable | [1] |
| Size and shape | Uniform | Variable (>3:1) in size | [1] |
| Nucleoli | May exist | Present | [1] |
| Mitotic index/10 HPFs | ≤12 | >12 | [1] |
| Precursor | SBT | STIC | [7] |
| Incidence | 4%–10% | >85% | [6] |
| Median age | Younger, <50 yr | Older, >50 yr | [6] |
| Stage at presentation | Early in about 40% | Advanced in 70%–80% | [6] |
| Clinical course | Indolent | Aggressive | [6] |
| Response to chemotherapy | Usually poor | Good but with high recurrence rate | [3–5] |
| Chromosomal instability | Low | High | [13] |
| Gene mutation | KRAS, BRAF, and ERBB2 | TP53 | [8] |
| 5-yr survival | 50%–60% | 30%–40% | [4,6,7,15] |
HGSC is considered to rise de novo in association with serous tubal intraepithelial carcinoma (STIC). On the other hand, LGSC appears to have a close phenotypic relationship to serous borderline tumors (SBT), particularly of the micropapillary type, because of similar cytomorphology, occasional co-existence of both borderline and low-grade components, and overexpression of CDKN1A and other TP53 modulated genes [9] indicating the existence of adenoma-carcinoma sequence [10]. Therefore, the revised WHO classification (2014) specifically defines micropapillary SBT as non-invasive LGSC.
SBT shares a common high KRAS mutation rate with LGSC (20%–40% of cases), and much more frequently shows BRAF mutations compared with LGSC (30%–50% vs. 0%–30%) especially in advanced stages [891011]. Deletion of tumor-suppressor function of miR-34a and CDKN2A/B has been suggested to be implicated in the progression of SBT to LGSC, although this finding remains to be confirmed by further evaluation [12]. The distinction between SBT and LGSC is critical for deciding on conservative or radical surgical management, since fertility is often a major concern in younger patients especially with bilateral disease [13]. A recent study has demonstrated that women below the age of 35 years with persistent disease at completion of initial therapy have a poorer outcome [14]. There has been a suggested association between an increased risk for developing LGSC in women who have a history of endometriosis [15].
3. Treatment targets
Traditional platinum-taxane combination chemotherapy has shown to have lower activity in LGSC compared to HGSC [5]. Commonly, primary cytoreductive surgery followed by adjuvant platinum based chemotherapy for advanced disease has been the standard practice in many countries despite limited evidence of benefit from chemotherapy [16171819]. Targeted therapies have, however, shown considerable promise, mainly in small non-randomized trials. Bevacizumab; Grisham et al. [20] performed a retrospective review of 17 patients who were treated with bevacizumab, 15 of whom were treated with combinations and 2 with bevacizumab alone. A partial response was obtained in 40% of the patient group (95% confidence interval [CI]=16.3%–67.7%). Similar results were obtained in a retrospective review performed by Schmeler et al. [21], with a response rate of 41% in a group of 21 patients. The value of bevacizumab in first-line treatment of serous ovarian cancers has been demonstrated in 2 phase III randomised studies; the GCIG International Collaboration on Ovarian Neoplasms 7 (ICON7) trial and the complementary Gynecologic Oncology Group study 0218 (GOG-0218) with promising results, however there were limited data in lower grade cancers (Table 2) [2223]. For recurrent disease, surgery remains the most effective intervention, and should be performed whenever possible. Hormonal therapy; LGSC express higher levels of estrogen receptor (ER), progesterone receptor (PR), and E-cadherin than HGSC, suggesting the possibility of these receptors as potential targets of therapy [24] and treatment with tamoxifen and letrozole has been shown to provide clinical benefit in epithelial ovarian cancers overall [2526]. A retrospective review of hormonal intervention suggested moderate anti-tumor activity in cases of recurrent LGSC with the median time to progression (TTP) being 7.4 months (95% CI=6.0–8.9 months), and that patients with both ER and PR double positive tumors had longer TTP than those who were PR negative. The study concluded that the stability of ER and PR in LGSC in the long term however was questionable and hence further studies are required [27]. Vemurafenib; the presence of V600E BRAF mutations, although low in incidence, is associated with an improved prognosis and is more frequently seen in early stage disease [28]. Treatment with vemurafenib, a BRAF inhibitor specific for V600E mutations has shown long term partial responses with improvement in both CA125 levels and in symptom control [29]. Mitogen-activated protein kinase kinase (MEK) inhibitors; Selumetinib (AZD6244, ARRY-142886) an orally available small molecule inhibitor of the MEK pathway was tested in a phase II clinical trial of 52 patients with LGSC. The median progression-free survival (PFS) was 11 months with a response rate of 15% (90% CI=7.9%–26.1%). The response to selumetinib did not appear to be related to RAS/RAF mutation status owing to significant tumor heterogeneity, and other factors that may contribute to pathway activation [30]. A randomized phase II/III trial is currently underway for trametinib, a MEK inhibitor, in recurrent or progressive low-grade serous ovarian cancer (GOG281), comparing the effectiveness of trametinib to chemotherapy chosen by the physician [31]. The MEK inhibitor in low-grade serous ovarian cancer (MILO) trial, an international, randomized phase III study of binimetinib or a chemotherapy chosen by a physician in patients with recurrent or persistent LGSC, was closed earlier after a planned interim analysis which showed that the hazard ratio for PFS crossed the predefined futility boundary [32]. Insulin-like growth factor 1 (IGF-1) pathway; IGF-1 is overexpressed in LGSC compared to SBT and HGSC and IGF-1 and Akt activation may be a potential drug target in the future [33]. Phase II trials are currently underway with the anti-IGF-1R monoclonal antibodies figitumumab (CP-751871) and ganitumab (AMG479) in epithelial ovarian cancer.
4. Take home message
As LGSC demonstrates distinct clinicopathologic and molecular features, it should be distinguished from HGSC in future clinical trials with translational components incorporated into their design. International cooperation will be required to establish strategies employing targeted agents as well as defining effective prognostic and predictive biomarkers. Finally, gynaecologic oncologists should be aware of the rare coexistence or progression to HGSC in cases of LGSC or SBT which can be a pitfall in management.
MUCINOUS CARCINOMA
1. Background
Ovarian mucinous carcinoma (OMC) is defined as an epithelial tumor with frank invasion (the largest invasive area equal to or greater than 5 mm) composed of gastrointestinal-type cells containing intracytoplasmic mucin. Recent studies have revealed that primary OMCs are much less common than previously reported (2%–3% of primary ovarian carcinomas), and that those reported as primary OMCs in the past likely included some metastatic tumors as well as mucinous borderline tumors [3435]. There are 2 types of invasion in OMCs, expansile (or confluent glandular) and infiltrative, which may coexist in a single tumor (Table 3). The pathological distinction of pattern of invasion is important, as there is significant difference in prognosis between those with confluent and infiltrative type of invasion. Majority of OMCs are with expansile invasion, almost always stage I, and are usually associated with a favourable prognosis [363738]. In contrast, about 80% of OMCs with infiltrative invasion are stage I, 20% of which recur. Recurrences tend to occur within 3 years of diagnosis and do not respond to chemotherapy or radiotherapy.
Table 3
Classification of mucinous tumors of the ovary

Distinction between primary OMCs and metastatic tumors may be pathologically challenging, although careful gross examination and thorough sampling of the tumor with assistance of immunohistochemistry in certain situation could lead to a correct diagnosis in many of the cases. Those with bilaterality, small size (<10 cm in diameter), high-stage, and an infiltrative invasion should raise suspicion for metastatic tumors [34394041]. The pathological features that favour primary mucinous tumors include: size >10 cm in diameter, multilocular cystic and/or solid tumor without multiple nodules, smooth external surface, expansile pattern of invasion, complex papillary pattern, coexistence of borderline or benign components, an association with a teratoma, endometriosis, adenofibroma, Brenner tumor, or mural nodule. Because OMCs typically form large cystic masses with or without solid component and are frequently admixed with benign and borderline components, sampling is crucial for accurate pathological diagnosis of OMCs. The number of the sections recommended is at least one per centimetre of maximum tumor dimension for tumor smaller than 10 cm, and 2 sections per centimetre for larger tumors [41].
2. Dilemmas in diagnosis and management
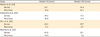
A small portion of advanced-stage mucinous tumors of the ovary are primary in origin (20%) and most are metastatic tumors from the gastrointestinal tract (45%), pancreas (20%), cervix (13%), breast (8%), uterus (5%), or unknown (10%) [35]. Clinicians face great challenge in pathologically distinguishing a primary mucinous tumor of ovarian origin from a metastatic tumor. In this case, molecular and clinical features may aid in distinguishing the two (Table 4) [404142434445]. A retrospective analysis of GOG182/ICON5 on independent review of 44 stage III/IV mucinous carcinomas of the ovary by 3 different pathologists, showed that median survival did not differ greatly between primary or metastatic groups. However, many of those mucinous carcinomas that were initially diagnosed as primary OMC appeared to be metastatic in origin [46].
Table 4
Differentiating mucinous carcinomas of primary vs. metastatic origin

As most OMCs present with localized disease (more than 80% of OMCs are stage I at the time of diagnosis), the standard treatment for patients with early mucinous carcinomas is cytoreductive surgery with pathological evaluation accompanied by surgical staging and special attention to possible gastrointestinal sites of primary disease. Nodal staging is not required in stage IA/IB due to the almost absence of nodal involvement. In younger patients with unilateral early stage disease it is reasonable to consider fertility sparing surgery. Furthermore, there is no clear evidence to suggest that adjuvant chemotherapy is beneficial in the setting of early stage disease. There is limited evidence for the effectiveness of systemic therapy in late stage OMCs. Most notably, only 2%–7% of patients in large randomized controlled trials had mucinous carcinomas. A retrospective review by Winter et al. [47] which investigated the effects of platinum/paclitaxel post debulking surgery in the mucinous cancer group, showed a median OS of 14.8 months comparable to 45.1 months in the serous group. Mimicking Winter's study, results produced by the Groupe d'Investigateurs Nationaux Pour les Etudes des Cancers de l'Ovaire (GINECO), GOG, and GCIG group have yielded similar results (Table 5) [484950].
Table 5
Comparison of OS and PFS in OMC compared to serous ovarian carcinoma
| Study | Median OS (mon) | Median PFS (mon) | |
|---|---|---|---|
| Winter et al. [47] | |||
| Serous | 45.1 | 16.9 | |
| Mucinous | 14.8 | 10.5 | |
| Alexandre et al. [48] | |||
| Serous | 47.2 | 17.5 | |
| Mucinous | 21.6 | 11.4 | |
| Tian et al. [49] | |||
| Serous | 40.5 | 16.7 | |
| Mucinous | 11.3 | 9.7 | |
| Mackay et al. [50] | |||
| Serous | 40.8 | 16.1 | |
| Mucinous | 14.6 | 7.6 | |
Disappointing results with first line platinum-based chemotherapy in OMCs have prompted research into specific targeted therapy such as agents that act on the human epidermal growth factor receptor 2 (HER2)/neu, KRAS, or angiogenesis pathways. A phase III study of carboplatin/paclitaxel vs. oxaliplatin/capecitabine with or without bevacizumab showed hope that bevacizumab may delay progression; however, the study was stopped early due to poor accrual of patients [51]. Molecular characterisation of mucinous ovarian tumors has shown overexpression of HER2 in 19% of cases with perfect agreement on immunohistochemistry, fluorescence in situ hybridization (FISH), and chromogenic in situ hybridization (CISH) [52]. A higher incidence of HER2 overexpression in the Asian population has been postulated by Chay et al. [53], and whilst the impact of HER2 status on OS is yet to be clearly established, anti-HER2 therapy in combination with other agents may have a role in management [5455].
3. Take home message
It is unfortunate that large trials for mucinous carcinomas in the international setting have been largely unsuccessful, and the best treatment is still unknown. As mucinous carcinomas have been shown to harbour a variety of molecular changes, the efficacy of single agent targeted therapy may be limited. Moreover, it is difficult to design adequately powered randomized controlled trials in cancers of such rare histological subtype. It will be important to use innovative trial designs to overcome this difficulty.
CLEAR CELL CARCINOMA
1. Background
Ovarian clear cell carcinoma (OCCC) is a subtype of epithelial ovarian carcinoma which is distinct from HGSC, associated with poor prognosis in advanced stages and has been shown to be resistant to conventional platinum-based chemotherapy [56]. It accounts for 5%–25% of epithelial ovarian cancers with a higher incidence seen in Eastern-Asian women. Women with OCCC usually present early with 57%–81% presentations in stage I or II, and are younger (median age 55 years) and the disease is commonly associated with endometriosis. Hypercalcaemia and an increased incidence of venous thrombotic events may occur [57].
Histological features of OCCC include a variety of growth patterns (micropapillary, tubulocystic, solid, and adenofibromatous), cell types (hobnail, clear cell, and oxyphilic), stromal changes (hyalinized, necrotic, hemorrhagic, and psammomatous calcification), and the presence of endometriosis, atypical endometriosis, and atypical proliferative clear cell tumors [585960]. These histological features often co-exist in the one tumor. Serous or endometrioid carcinoma frequently demonstrates cytoplasmic clearing (clear cell change), which leads to difficulty in accurate diagnoses of OCCC. A mitotic count greater than 5 per 10 HPFs is almost never encountered, with most tumors having mitotic counts between 0 and 2 per 10 HPFs [59]. The tumor arises from endometriosis in 50%–70% of cases [58]. An adenofibromatous pattern is present in 20%–25% of cases, and stromal hyalinization is one of the characteristic features [5859].
2. Molecular changes in OCCC and translational possibilities
The molecular pathogenesis of OCCC is less well characterised than HGSC, however many studies show that it harbors unique molecular features including the AT-rich interactive domain 1A (ARID1A) gene mutation, hepatocyte nuclear factor-1β (HNF-1β) overexpression, and the phosphatidylinositol-4,5-bisphosphate 3-kinase (PIK3CA) mutation (Table 6) [6162]. ARID1A encodes a key component of the switch/sucrose nonfermentable (SWI/SNF) chromatin remodelling complex that regulates gene expression targeting multiple pathways that lead to tumorigenesis. It acts as a tumor-suppressor gene in OCCC and is seen in pre-neoplastic lesions leading to the speculation that this gene is implicated in the early transformation of endometriotic cells into cancer. It has been identified in up to 57% of cases of OCCC however no distinct phenotypical property has been identified that may contribute to increased survival [63646566]. HNF-1β is a transcription factor with predominant expression in liver, pancreas, and kidney and is known as a hallmark of OCCC. HNF-1β plays multiple roles in tumorigenesis and chemoresistance by alteration of glycolytic processes in OCCC cells, and by reducing oxidative phosphorylation and thus intracellular reactive oxygen species. Anti-stress properties that allow the survival of endometrial cells induce HNF-1β in the microenvironment and this is maintained throughout its cell life into malignant proliferation. This conferred stress resistance may contribute to the chemoresistance of OCCC [6768]. PIK3CA mutations play an important role in the pathogenesis of OCCC with mutations seen in up to 42% of cases. PIK3CA activation results in abnormal cellular growth, proliferation, survival, and angiogenesis via complex intracellular networks in the regulation of tumor stem cells. PIK3CA mutations have been associated with favourable OS in OCCC in a mutational analysis of 56 primary OCCC cases in Japanese women [69707172]. Vascular endothelial growth factor (VEGF) overexpression is commonly seen in advanced stage epithelial ovarian cancer and is often associated with a poorer prognosis [7374]. With its critical role in angiogenesis, this overexpression may be a therapeutic target and in vitro studies have been promising, showing inhibition of OCCC cell growth especially in cisplatin-refractory cases, highlighting its potential role in recurrent disease [75].
Table 6
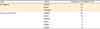
| Type | Gene | Frequency of mutation (%) |
|---|---|---|
| Oncogene | PIK3CA | 54 |
| KRAS | 10 | |
| PPP2R1A | 10 | |
| Tumour suppressor | ARID1A | 62 |
| MLL3 | 15 | |
| ARID1B | 8 | |
| ASXL1 | 8 | |
| CHD8 | 8 | |
| PIK3R1 | 8 |
ARID1A, AT-rich interactive domain 1A; ARID1B, AT-rich interactive domain 1B; ASXL1, additional sex combs-like 1; CHD8, chromodomain helicase DNA binding protein 8; MLL3, mixed-lineage leukemia protein 3; OCCC, ovarian clear cell carcinoma; PIK3CA, phosphatidylinositol-4,5-bisphosphate 3-kinase; PPP2R1A, protein phosphatase 2 regulatory subunit A alpha.
3. Controversies in the clinical management of OCCC
Women with OCCC present in early stages, and at a younger age, raising the question of the role of cytoreductive vs. fertility sparing surgery. Evidence to support complete surgical staging in early stage OCCC is lacking; however, the goal of primary surgical treatment in advanced disease should be complete cytoreduction. In the GOG study by Hoskins in 1994, mucinous and clear cell subtypes demonstrated a poor outcome despite small residual tumor size even after primary cytoreductive surgery [76]. A retrospective analysis of 254 patients showed that only primary cytoreduction which was complete contributed to a better in advanced cases [77]. On a similar note, the role of lymphadenectomy from a therapeutic perspective is unclear. It is acknowledged that the presence of lymph node metastases is an independent prognostic factor however it is not associated with OS on multivariate analysis [7879808182]. Importantly, women undergoing fertility sparing surgery in OCCC did not show poorer survival than their non-OCCC counterparts [8384858687].
OCCC demonstrates a lower response rate to platinum based chemotherapy compared to HGSC, with response rates of 11%–56% compared to 73%–81% in serous subtypes [77]. The Japanese Gynecologic Oncology Group (JGOG) undertook a randomized phase III trial (JGOG3017) of paclitaxel/carboplatin versus irinotecan/cisplatin as first-line chemotherapy in patients with stage IC–IV OCCC which showed no significant difference in 2-year PFS or OS [88], suggesting the need for an alternative approach such as targeted therapy.
4. Take home message
There are still significant gaps in our understanding of OCCC. The effect of hormonal status on malignant transformation is incompletely understood and the risks of subsequent malignancy in women with endometriosis remains unclear. A number of international trials have been designed with the aim of identifying molecular targets; however, it is acknowledged that the presence of such targets may not translate into the effectiveness of agents used to target them. Adequately powered trials with novel designs will be necessary to provide improved clinical outcomes for patients with these rare tumors.
CONCLUSION
Designing adequately powered studies to perform large scale randomized trials is the single largest barrier in improving understanding of rare epithelial ovarian cancers. International collaboration with multidisciplinary and translational components through groups such as the GCIG is required. Multiple smaller trials which screen agents for activity should be considered in the first instance, with expansion into larger randomized trials for agents that show promising activity. Additionally, the poor prognosis associated with many of these rare cancers at advanced stages signify the need for further research in developing novel methods for screening.
 XML Download
XML Download