

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Paclitaxel is a natural product obtained from the bark of the Pacific yew tree, Taxus brevifolia. Paclitaxel has demonstrated significant activity in clinical trials against a wide variety of tumors, including ovarian, breast, lung, and head and neck cancers [1]. To enhance the solubility of the hydrophobic paclitaxel compound, it has been prepared with a micelle-forming vehicle, Cremophor EL (CrEL) [2]. However, the addition of CrEL causes dose-limiting toxicities (DLTs). Patients treated with this drug exhibit hypersensitivity reactions, which might be due to CrEL-induced formation of complement-activating particles [3]. Moreover, neurotoxicity associated with paclitaxel might be due to CrEL-induced axonal demyelination and swelling [4]. In addition, CrEL-paclitaxel formulations exhibit nonlinear pharmacokinetics, because the CrEL micelles impede drug metabolism and tissue distribution. In contrast, CrEL-free paclitaxel exhibits linear pharmacokinetics [56]. Clinically, CrEL-paclitaxel formulations are associated with relatively low biological responses, due to the altered pharmacokinetics of paclitaxel; on the other hand, higher doses can cause hypersensitive reactions and neurotoxicity. Therefore, novel paclitaxel formulations, either without CrEL or with smaller amounts of CrEL, have been designed to reduce or eliminate DLTs, and thereby improve the therapeutic effect [78910].
Genexol-PM (Samyang Co., Seoul, Korea) is a novel, polymeric micellar (PM) paclitaxel formulation. The polymeric micelles comprise a low-molecular-weight, nontoxic, biodegradable, amphiphilic, diblock copolymer, monomethoxy poly(ethylene glycol)-block-poly(D,L-lactide) (mPEG-PDLLA) [11]. In vivo, Genexol-PM was shown to have a maximum tolerated dose (MTD) 3-times higher than paclitaxel. Moreover, the PM component increased the drug's tissue distribution by 2–3-fold in various organs, most importantly, in tumors. Thus, Genexol-PM provided great advantages over conventional paclitaxel in antitumor activity [11].
The pharmaceutical preparation development of Genexol-PM had commenced at 1998 and preclinical studies were conducted for evaluating pharmacokinetics, pharmacological, and toxicological profiles of Genexol-PM. The first investigational new drug application (IND) was submitted to Korea Food and Drug Administration in July 2001 and Genexol-PM was approved in Korea in July 2006 with the indications of a first-line therapy for recurrent and metastatic breast cancer and non-small-cell lung cancer (NSCLC) in combination with cisplatin.
As regulation of pharmaceuticals approval, notification and review, ovarian indication is added based on the same pharmacological mechanism of the drug, or active pharmaceutical ingredient and indication are same with ones of previously approved anticancer. The active control of paclitaxel + carboplatin is a first-line ovarian cancer therapy. Two phase I monotherapy studies were previously conducted, with Genexol-PM administered once every 3 weeks in patients with advanced cancers. One trial was performed in the USA, and it reported a MTD of 435 mg/m2. The other trial was performed in Korea, and it showed an MTD of 390 mg/m2 [12]. Subsequently, a phase II study was conducted, with Genexol-PM, administered at 300 mg/m2, once every 3 weeks in patients with metastatic breast cancer. That trial showed good efficacy and tolerable toxicities [13]. The pharmacokinetics of Genexol-PM displayed dose-proportionality in phase I monotherapy trials, with once every 3 weeks and once-weekly schedules [1214]. Based on those previous results, we performed a phase I study to determine the MTD and DLTs in patients with advanced ovarian cancer that received Genexol-PM as a first-line treatment combined with carboplatin.
MATERIALS AND METHODS
1. Eligibility
This study was performed at the Seoul National University Hospital (Seoul, Korea), Asan Medical Center (Seoul, Korea), and Severance Hospital (Seoul, Korea). Patients were eligible for the trial when they satisfied the following inclusion criteria: (1) 18 years or older; (2) written informed consent provided before study participation; (3) histologically diagnosed with an advanced epithelial ovarian cancer, classified as IIIB-IV according to International Federation of Gynecology and Obstetrics (FIGO) classifications; (4) disease measurable with the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.0 [15], and no experience with chemotherapy; (5) appropriate for paclitaxel and carboplatin combination therapy; (6) Eastern Cooperative Oncology Group (ECOG) performance grade 0–2; (7) life expectancy more than 6 months; and (8) proper blood, kidney, and liver function upon screening, within 14 days before administration of the test drugs; indicators of proper function were defined as follows: hemoglobin (Hb) level ≥10 g/dL, absolute neutrophil count (ANC) ≥1.5×109/L, platelet count ≥100×109/L, serum total bilirubin ≤1.5 times the upper limit of normal (×ULN), serum aspartate transaminase (AST) and alanine transaminase (ALT) ≤2.5×ULN, serum alkaline phosphatase (ALP) ≤2.5×ULN, and serum creatinine ≤1.5×ULN.
The study exclusion criteria were: (1) received chemotherapy other than debulking surgery; (2) received radiotherapy in the abdominal cavity or pelvis; (3) received immunotherapy or hormone therapy for ovarian cancer; (4) history of carcinoma in the past 5 years; (5) received a major surgery other than debulking surgery within 2 weeks before the screening; (6) past or present medical history of metastasis in the central nervous system (CNS); (7) grade 1 or higher level of sensory or motor neuropathy, based on the National Cancer Institute Common Toxicity Criteria for Adverse Events (NCI CTCAE) V3.0; (8) severe comorbidities, including a medical or mental condition that prevented understanding the clinical trial and providing written informed consent, severe cardiovascular disease, uncontrolled active infectious disease, or hypersensitivity to the test drugs or the vehicle; and (9) participated in another study within 4 weeks before the screening.
All participants provided written informed consent. The study protocol was approved by the appropriate institutional review boards and by independent ethics committees. The study was in compliance with Good Clinical Practices, Guidelines of the International Conference on Harmonization, and the Declaration of Helsinki.
2. Study design
This was an open-label, multicenter, phase I, dose-escalation study. Samyang Corporation supplied the Genexol-PM. A premedication was applied before starting Genexol-PM to minimize hypersensitivity. The dose escalation was designed according to the modified Fibonacci sequence [16]. Genexol-PM doses were administered in 3 study stages: stage 1 (220 mg/m2), stage 2 (260 mg/m2), and stage 3 (300 mg/m2); in all study stages, carboplatin was administered at 5 area under the curve (AUC). The drugs were administered on the first day of every cycle (one cycle consisted of 3 weeks) for a maximum of 6 cycles. The duration was extended in responsive subjects, at the investigator's discretion. Doses were reduced to the next lower dose, when subjects exhibited DLT; the medication was withdrawn, when a subject continued to experience toxicity.
In stage 1, we enrolled 6 subjects and evaluated DLTs during the first treatment cycle. When DLTs occurred in no more than 1 subject, the next 6 subjects were enrolled for stage 2. Again, in stage 2, when DLT occurred in no more than 1 subject, the next 6 subjects were enrolled for stage 3 (300 mg/m2). The study plan was to stop dose escalations when DLT occurred in more than 2 subjects in any stage, and the concerned dose would be defined as the MTD. This MTD would be recommended for the phase II study, based on general toxicity. If DLTs did not occur in more than 2 subjects in the stage 3 group, the recommended dose was determined as 300 mg/m2 or less, based on the patterns of adverse events.
3. Safety and efficacy analysis
A safety analysis was performed for every subject that received the test drugs. Several safety variables were used for descriptive statistics estimations, including ECOG performance status, electrocardiograms, physical examinations, vital signs, laboratory tests, and adverse events. The severities of adverse events were evaluated according to NCI CTCAE V3.0. Serious adverse events and adverse drug reactions were analyzed separately. DLTs were evaluated during the first treatment cycle, and they were defined as one of the following events: (1) grade 3 or more hypersensitivity, despite the premedication recommended by the NCI CTCAE V3.0; (2) grade 3 or 4 non-hematologic toxicity, other than nausea and vomiting; (3) grade 4 neutropenia for more than 7 days, or febrile neutropenia, despite granulocyte-colony stimulating factor (G-CSF) administration; and (4) grade 4 thrombocytopenia for more than 7 days or grade 3 thrombocytopenia with bleeding.
The antitumor effect of Genexol-PM and carboplatin combination therapy was evaluated, based on the objective response rate (ORR). The ORR was defined as the proportion of subjects that achieved a complete tumor response (CR) or partial tumor response (PR). The overall response included tumor response evaluations of target and non-target lesions, performed after every 2 treatment cycles. Both the tumor response and the overall response were evaluated according to RECIST version 1.0 [15].
RESULTS
1. Patient characteristics
This study included 18 patients that agreed to participate, met the inclusion/exclusion criteria at screening, and received the test drugs. These 18 patients constituted the Intention-To-Treat (ITT) population. Of these 18 patients, 3 patients dropped out, due to DLT (n=1), hypersensitivity (n=1), and follow-up loss (n=1); the remaining 15 patients completed the study according to the protocol; these patients constituted the Per-Protocol (PP) population. Patient characteristics are listed in Table 1. The median patient age was 59.0 years (range: 40–75 years). At screening/baseline, the ECOG performance was grade 0 or grade 1. All subjects had tumors with histopathological grades of G3 (poorly differentiated) or G2 (moderately differentiated). The FIGO stages at diagnosis were IIIB, IIIC, and IV (Table 1).
Table 1
Characteristics of patients with ovarian cancer enrolled in this study
2. Determination of MTD and DLTs
The dose-escalation scheme of Genexol-PM is shown in Table 2. No DLT was reported in stage 1 (220 mg/m2) or stage 2 (260 mg/m2), but in stage 3 (300 mg/m2), one out of 6 subjects experienced DLT. This patient experienced general pain, which was classified in the NCI CTCAE V3.0 as a grade 3 or a non-hematological toxicity, other than nausea and vomiting. Thus, based on DLT, which was the primary safety variable, we did not detect a MTD for Genexol-PM for the 3 doses tested in 18 subjects of the ITT population. Therefore, we recommended a dose of 300 mg/m2 or less for the phase II study.
Table 2
Dosage escalation scheme and administration of treatments for patients with ovarian cancer

3. Adverse events
Overall, 18 (100.0%) subjects experienced 383 cases of adverse events, including events unrelated to the test drugs. The incidence of adverse drug reactions was 330 cases in 18 (100.0%) subjects. Considering the incidence per adverse event type, 16 (88.9%) patients experienced 158 cases of blood and lymphatic system disorders; 16 (88.9%) patients reported 47 cases of gastrointestinal disorders; 14 (77.8%) patients reported 25 cases of nervous system disorders; and 14 (77.8%) patients reported 24 cases of skin and subcutaneous tissue disorders. Table 3 summarizes the representative adverse drug reactions observed during the study at each dose level. The severities of adverse events were evaluated as mild in 121 (31.6%) cases, moderate in 153 (40.0%) cases, severe in 79 (20.6%) cases, life-threatening in 30 (7.8%) cases, and death did not occur. Thirty cases of serious adverse events occurred in 10 (55.6%) patients during the study period (Table 4). The Genexol-PM combined with carboplatin administration remained unchanged in 368 (96.1%) cases. Treatment was temporarily discontinued in 10 (2.6%) cases, permanently discontinued in 4 (1.0%) cases, and dose-reduced in 1 (0.3%) case, due to adverse events. Patients recovered from a total 283 (73.9%) cases of adverse events without sequelae, and no death related to the disease or treatment was reported. One of 3 patients who dropped out of the study experienced a grade 2 hypersensitivity at 220 mg/m2 dose during the cycle 2, after completing the cycle 1. This toxicity was not considered as a DLT based on the protocol, but she was dropped in this clinical trial by the intention of the patient.
Table 3
ADR in patients treated for ovarian cancer, stratified by dose level
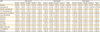
Table 4
SAE among patients treated for ovarian cancer
4. Antitumor response
All patients had measurable sites that were evaluable for an antitumor response. Seventeen patients in the ITT population received tumor evaluations, and of those, 94.1% (16/17) were ORRs (95% confidence interval [CI]=82.9–100.0). The ORRs per dose were 100.0% (n=6; 95% CI=100.0–100.0) for the 220 mg/m2 dose group, 83.3% (n=5; 95% CI=53.5–100.0) for the 260 mg/m2 dose group, and 100.0% (n=5; 95% CI=100.0–100.0) for the 300 mg/m2 dose group. The groups showed no statistically significant differences (p=1.00). Based on the best overall response of the 15 patients in the PP population, the ORR (including CRs and PRs) was estimated as 93.3% (n=14; 95% CI=80.7–100.0). Tumor re-evaluations were performed in 17 out of 18 subjects in the ITT population. The results were the same as those found in the previous tumor evaluations, except in 4 subjects, which showed CRs in the previous evaluations, but PRs in the re-evaluations (Table 5).
Table 5
Rate of response to ovarian cancer treatment, stratified by dose level
DISCUSSION
Paclitaxel is the most important drug for the treatment of epithelial ovarian cancer. However, the paclitaxel solubilizer, CrEL, has been shown to influence paclitaxel toxicity (including hypersensitivity reactions and peripheral neuropathies), pharmacokinetics, and antitumor activity [5617181920]. In contrast, Genexol-PM is a CrEL-free, paclitaxel loaded into polymeric micelles, which was approved in Korea in 2006 as a first-line therapy for recurrent and metastatic breast cancer and NSCLC. Compared to the conventional paclitaxel, preclinical studies demonstrated that the PM paclitaxel formulation displayed a 3-fold higher MTD and significantly stronger antitumor effects [11]. In a phase I study, where Genexol-PM was tested for treating advanced malignancies [12], the main DLTs were neuropathy, myalgia, and neutropenia, and the recommended phase II dose was 300 mg/m2, once every 3 weeks. In another study, a tri-weekly dose of Genexol-PM (230 mg/m2) was combined with cisplatin (60 mg/m2) as a first-line therapy for advanced NSCLC [21]. In a second treatment cycle, 46% of patients received dose escalations to 300 mg/m2. The major hematological toxicity was grade 3/4 neutropenia (46.4%). The major non-hematologic toxic effects included grade 3 peripheral sensory neuropathy (13.0%) and grade 3/4 arthralgia (7.3%). Four patients (5.8%) experienced grade 3/4 hypersensitivity reactions. A premedication to prevent hypersensitivity was not initially recommended. However, during the study, a prophylaxis for hypersensitivity was routinely recommended, typically hydrocortisone, antihistamine, or an H2 blocker. In addition, several phase II clinical trials conducted in Korea and the US indicated that Genexol-PM was generally well tolerated, and it showed sufficient antitumor activity in patients with metastatic breast cancer, urothelial carcinoma, and progressive pancreatic cancer [132223].
This phase I clinical trial investigated a previously untested combination of Genexol-PM, once per 3 weeks, with carboplatin, as a first-line chemotherapy in ovarian cancer, A previous phase I trial tested Genexol-PM as a single therapy in advanced malignancies, but only one patient had ovarian cancer. Moreover, that study evaluated the therapy in a palliative setting [12]. Based on that study, and another which combined Genexol-PM with cisplatin [1221], in the present study, we selected initial doses of 5 AUC carboplatin and 220 mg/m2 Genexol-PM. A Genexol-PM MTD was not determined in this study, because only 1 DLT occurred with the highest dose tested (300 mg/m2). Among our patients, Genexol-PM toxicity mainly manifested as neutropenia and neuromuscular toxicity, similar to those reported with paclitaxel treatment [117]. However, despite the higher paclitaxel dose administered with Genexol-PM, the combination therapy-associated adverse events we observed were comparable to those observed with conventional paclitaxel and carboplatin regimens. We observed a 22.2% incidence of grade 3/4 neutropenia, which was comparable to that reported in other phase III trials that used standard doses of paclitaxel combined with carboplatin [2425]. The most common non-hematologic toxicity in the current study was peripheral neuropathy (17.6%). Although grade 3/4 peripheral neuropathy was not reported in this study, Genexol-PM induced neuromuscular toxicity similar to that induced by CrEL-formulated paclitaxel. This suggested that the neuropathy was most likely caused by the paclitaxel, rather than a component of the carrier [20]. A previous phase I and pharmacokinetic study [12] found severe neurotoxicities at doses of 230 and 390 mg/m2; within those treatment groups, the development of significant neurotoxicity tended to be associated with a higher area under the paclitaxel curve and a higher maximum paclitaxel concentration. A randomized trial of nab-paclitaxel plus gemcitabine for treating pancreatic cancer also showed a relatively high incidence of peripheral neuropathy (17%) [26], comparable to our results.
In the previous phase I study, the pharmacokinetics of Genexol-PM tended to be linear, unlike the non-linear pharmacokinetics observed with conventional paclitaxel [12]. The AUC from time 0 to infinity (AUCinf) and the peak or maximum paclitaxel concentration (Cmax) of Genexol-PM injection were lower than the same doses of Taxol injection, and the half-life of Genexol-PM injection was relatively short, compared to 20.1 hours of the half-life of Taxol injection. The systemic total body clearance was higher than that of Taxol injection (12.2–17.7 L/hr/m2) reported in literature. However, the average apparent volume of paclitaxel distribution in the elimination phase after the intravenous administration of Genexol-PM injection was greater than that of Taxol injection. It was inferred that the clearance and apparent volume of distribution increased because as more paclitaxel was moved to peripheral and cancer tissues when administering Genexol-PM injection, a fast extinction of paclitaxel in systemic circulation and a longer movement time was taken. It has been suggested that Genexol-PM preferentially targets tumor tissues, which results in prolonged tumor exposure. Furthermore, compared to conventional paclitaxel, Genexol-PM showed a lower AUC and a shorter plasma half-life, which might be explained by the enhanced distribution of Genexol-PM into tumor tissues. Accordingly, Genexol-PM was expected to have significant advantages over conventional paclitaxel because it permitted the delivery of much higher doses and it enhanced the drug distribution to tumors. In the present study, the best overall response (including CR and PR) in the ITT population was estimated at 94.1%. Although CR was reported in only 2 patients, the ORR of 94.1% was a significant result, considering that the study was designed for patients with measurable disease after debulking surgery for advanced ovarian cancer.
Efficacy evaluations of Genexol-PM with advanced solid cancer were performed over the 135–390 mg/m2 (135, 175, 230, 300, and 390 mg/m2) dose range and the MTD of Genexol-PM was determined to be 390 mg/m2 in the study [12]. PRs were observed in 3 of the 21 patients (14%) and the first PR patients was at dose level 2 (175 mg/m2). The recommended regimen for Genexol-PM in breast cancer is 260 mg/m2. If grade 2 or higher non-hematological toxicities do not occur in the first cycle, increase the dose to 300 mg/m2 in the second cycle. After the completion of this phase I clinical study, we recommended a dose of 300 mg/m2 or less for a phase II study. Actually the phase II pivotal study in ovarian cancer was designed to receive 260 mg/m2 of Genexol-PM allowing for the increase of dose to 300 mg/m2.
In conclusion, in the present phase I study, based on DLT, no MTD was detected at the doses tested for Genexol-PM with carboplatin as a first-line treatment for advanced ovarian cancer. Moreover, the results of this Genexol-PM trial did not significantly change existing safety data. Only 1 patient experienced a grade 3 DLT of general pain at a dose of 300 mg/m2. Consequently, we recommended a dose of 300 mg/m2 or less for a phase II study. The high paclitaxel dose achieved without additional significant toxicity suggested that Genexol-PM could potentially replace the conventional paclitaxel formulation. Further studies of Genexol-PM are warranted to evaluate its efficacy, optimal schedules, and long-term outcomes.
 XML Download
XML Download