

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
It is well recognized that the persistent infection of the uterine cervix with a high-risk human papillomavirus (HR-HPV) is a major cause of invasive cervical cancer and its precursor [1]. Infections with HPV-16 and HPV-18 are associated with the highest risk for cervical intraepithelial neoplasia (CIN) 2 or worse (≥CIN 2). HPV-16 and HPV-18 are responsible for 70% of all invasive cervical carcinomas, followed by HPV-45/31/33 [234].
The cytology test, which is used as a cervical cancer screening tool, has been successfully contributing to a decrease in cervical cancer incidence and its associated mortality. However, recent guidelines favor performing HPV DNA testing in addition to the cytology test (co-testing) [4]. Because the cytology test has low sensitivity and reproducibility, adding a HPV DNA test to cytology increases the sensitivity for detecting high grade squamous intraepithelial lesions (HSILs) or invasive cancers. Moreover, the screening interval is extended to every 5 years compared to every 3 years when the cytology test is used alone. In 2015, new interim guidance on HPV primary screening for cervical cancer was established [4]. It recommends primary HPV testing for women who are age 25 or older. For women with HR-HPV (–), follow-up after 3 years is recommended. For women with HPV-16/18 (+), direct colposcopy is advised, and for women with other non-16/18 HR-HPV (+), the cytology test is advised. If the cytology test shows a negative intraepithelial lesion or malignancy (NILM) result, follow-up with both cytology and HR-HPV testing at 12 months is indicated. If the cytology result is atypical squamous cells of undetermined significance (ASCUS) or worse (≥ASCUS), the appropriate treatment guideline is followed [4].
Among the HR-HPV genotypes, some genotypes that are closely related evolutionarily (e.g., HPV-16 and HPV-31) exhibit different degrees of cancer risk, which are thought to be related to different protein functions and patterns of gene expression [5]. Numerous studies have revealed information about the biology and life-cycle of HPV, but these processes are not fully understood. Although the prevalence of HPV and its detected genotypes is variable across the world, HPV-16, -18, -31, -52, and -58 are consistently found worldwide [67].
The U.S. Food and Drug Administration (FDA) has recently approved a recombinant 9-valent HPV vaccine (Gardasil 9, Merck, Kenilworth, NJ, USA) for the prevention of anogenital cancer caused by HPV-16, -18, -31, -33, -45, -52, and -58 and for the prevention of genital warts caused by HPV-6 and -11. Four genotypes are from the licensed Gardasil vaccine (HPV-6, -11, -16, -18), and five are new additions (HPV-31, -33, -45, -52, -58) [89]. The five additional HPV types covered by Gardasil 9 account for approximately 20% of cervical cancers.
Current screening algorithms of both co-testing or HPV primary screening guidelines do not reflect the difference in risk for ≥CIN 2 among women with various non-16/18 HR-HPV genotypes. However, a number of studies revealed that, in Asia (unlike America, Australia, Europe, and Africa), a higher percentage of HPV-52 and HPV-58 is associated with cervical cancer and HPV-52 and HPV-58 are comparable to HPV-16 and HPV-18 in prevalence for invasive cervical cancer [67]. This is consistent with several investigations that studied Korean women [101112]. Previous studies showed that HPV-16, -18, -52, -45, -58, -35, -33, and -31 were strongly associated with cervical cancer and precancer lesions in Asian women, especially Korean women [13]. In this study, we examined the HPV genotype distribution and odds ratios for histologically confirmed ≥CIN 2 for each HR-HPV genotype using a commercially available HPV DNA chip test (HPV 9G DNA chip, Biometrix Technology Inc., Chuncheon, Korea) to test the hypothesis that HPV genotyping can classify non-16/18 HR-HPV infection by risk stratification.
MATERIALS AND METHODS
1. Study subjects
This study was approved by Institutional Review Boards of Catholic Medical Center Office of Human Research Protection Program (KC15RISE0866). The pathology archive database records of Seoul St. Mary's Hospital were reviewed, and 32,873 patients visited the Gynecologic Department of the hospital for cervical examination from October 2012 to April 2015. All referred patients with abnormal cervical cytology from local clinic underwent Papanicolaou testing (Pap test) and colposcopy, followed by biopsy if necessary. The HPV DNA test was routinely recommended and performed for patients who consented. Colposcopic biopsy was done in patient with abnormal cervical cytology from local clinic or abnormal findings of colposcopy (such as acetowhite epithelium, leukoplakia, punctuation, mosaicism, or abnormal vascular pattern).
Among them, total of 1,838 patients (5.6%) underwent excisional biopsies in addition to the Pap test, and 1,142 patients (62.1%) underwent HPV test using HPV 9G DNA chip, simultaneously. p16 immunohistochemistry was performed in uncertain cases for a differential diagnosis between a low grade squamous intraepithelial lesion (LSIL) and HSIL. After a retrospective review, we excluded 39 patients with insufficient for diagnosis and one patient of an unrelated malignancy (malignant lymphoma).
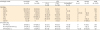
The average age of all 1,102 patients was 40.1 years, and the age distribution was as follows: age ≤29, 195 patients (17.7%); 30 to 39 years, 327 patients (29.7%); 40 to 49 years, 340 patients (30.9%); 50 to 59 years, 169 patients (15.3%); and age ≥60, 71 patients (6.4%) (Table 1).
Table 1
Age distribution according to HPV genotyping results*

Values are presented as number (%).
HPV, human papillomavirus; HR, high-risk.
*HR-HPV (+) includes HPV-16 (+) and/or HPV-18 (+) and/or 12 other non-16/18 HR-HPV (+); HPV-16/18 (+) includes HPV-16 (+) and/or HPV-18 (+), with or without any other HPV genotypes (+); non-16/18 HR-HPV (+) includes HPV-16 (–) and HPV-18 (–), 12 other HR-HPV (+) with or without low-risk HPV (+) or 'HPV-other types' (+); among all 1,102 cases, 113 cases were infected with multiple HPV genotypes, and they were classified as the group with the higher risk for its constituents. †Evaluable subjects with valid HPV results and valid biopsy results.
2. HPV genotyping
HPV 9G DNA genotyping was performed according to the manufacturer's protocol [1415] under the supervision of Dr. A. Lee (a pathologist with a specialty in gynecopathology and molecular pathology). Briefly, all specimens of swabs were placed in a SurePath preservative vial (BD Diagnostics-Tripath BD Biosciences, Oxford, UK) and transferred to the pathology laboratory. From this specimen, viral nucleic acids were extracted by using a commercial QIAsymphony DSP Virus/Pathogen Mini Kits (QIAGEN, Venlo, the Netherlands) and were amplified by duplex polymerase chain reaction (PCR) to generate amplicons. The HPV DNA was amplified with primers Right Primer (RP)-Cy5 (3'-GAAAHATAAACTGTAAATCATAYTC-Cy5-5') and Forward primer (FP) (3'-GCMCAGGGWCATAAYAATGG-5'). Five microliters of the Cy5-labeled PCR product were subjected to agarose gel electrophoresis using 2% agarose in 1X Tris-borate ethylenediaminetetraacetic acid (EDTA) according to the standard protocol. The Cy5-labeled PCR product was used for further hybridization experiments on the HPV 9G DNA chip for HPV detection and genotyping. HPV amplicons were hybridized with type-specific oligonucleotide probes and visualized on HPV 9G DNA chips as double-positive spots when HPV DNA was present in the amplified PCR product. The HPV 9G DNA chip identified single or multiple infections of 14 HR-HPV genotypes (HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, -66, and -68) and five low-risk (LR)-HPV genotypes (HPV-6, -11, -34, -40, and -42). A specimen was classified as “HPV-other types” when a positive band was detected by gel electrophoresis for PCR products with no specific spot identified for either the 14 HR-HPV or five LR-HPV genotype on the HPV DNA chip.
3. Statistical analysis
The clinical usefulness of the HPV DNA chip and cytology tests (sensitivity, specificity, positive predictive value [PPV], and negative predictive value [NPV]) for the identification of ≥CIN 2 was determined using standard statistical tests. Statistical analyses were performed to assess the association of factors with ≥CIN 2. The age-adjusted odds ratios of HSIL with the respective 95% CIs were determined for different categories of HPV DNA chip results by binary logistic regression using IBM SPSS ver. 22.0 (IBM Co., Armonk, NY, USA). In all cases, a p≤0.05 was considered statistically significant. The HR-HPV (+) result includes single or multiple positives for 14 HR genotypes. The HPV-16/18 (+) result includes HPV-16 (+) and/or HPV-18 (+), with or without any other HPV genotypes present. The non-16/18 HR-HPV (+) result includes HPV-16 (–) and HPV-18 (–), 12 other HR-HPV (+) with or without LR-HPV (+) or 'HPV-other types' (+). The HR-HPV (–) result includes LR-HPV (+) or 'HPV-other types' (+) or HPV (–).
RESULTS
1. HPV DNA chip, cytology, and histology results
Among all 1,102 patients, those with HR-HPV (+), HPV-16/18 (+), and non-16/18 HR-HPV (+) were distributed as 577 patients (52.4%), 231 (21.0%), and 346 (31.4%), respectively. A total of 113 patients (9.75%) were infected with multiple HPV genotypes. The numbers and percentages of HR-HPV (+), HPV-16/18 (+), and non-16/18 HR-HPV (+) for each age group of patients is summarized in Table 1. In cases of multiple infections, patients were classified into to the group with the higher risk for its constituents. For example, a case with both HPV-16 (+) and HPV-35 (+) was classified into the HPV-16/18 (+) group.
Among patients whose cytology tests were NILM, ASCUS, atypical glandular cells, atypical squamous cells that could not exclude HSIL, LSIL, HSIL, and invasive cancer, histology confirmed ≥CIN 2 were 4.3% (15/349), 7.5% (15/199), 33.3% (7/21), 59.3% (51/86), 12.2% (31/255), 88.8% (135/152), and 97.5% (39/40), respectively. Among seven patients whose cytology tests were HSIL or invasive cancer with a histology-based diagnosis of cervicitis, three patients were diagnosed as squamous cell carcinoma by follow-up biopsy after 5 months, 11 months, and 2 years and one patient was diagnosed as CIN 3 by follow-up biopsy after 6 months. The remaining three patients had insufficient gynecologic follow-up.
Among patients with HPV (–), non-16/18 HR-HPV (+), and HPV-16/18 (+), the histology-confirmed ≥CIN 2 was 7.6% (40/525), 33.5% (116/346), and 59.3% (137/231), respectively. HPV-16 and/or -18 were detected in 15.7% (56/356) of patients with histology LSIL, 43.0% (104/242) of patients with histology HSIL, 100% (4/4) of patients with histology adenocarcinoma in situ, and 61.7% (29/47) of patients with histology invasive cancer. The correlation of each cytology and HPV DNA chip result with its corresponding histology result is summarized in Table 2.
Table 2
Histology results according to cytology and HPV genotyping results*
Values are presented as number (%).
AIS, adenocarcinoma in situ; AGC, atypical glandular cells; ASCUS, atypical squamous cells of undetermined significance; ASC-H, atypical squamous cells cannot exclude HSIL; CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; HR, high-risk; HSIL, high grade squamous intraepithelial lesion; LSIL, low grade squamous intraepithelial lesion; NILM, negative intraepithelial lesion or malignancy.
*HR-HPV (+) includes HPV-16 (+) and/or HPV-18 (+) and/or 12 other non-16/18 HR-HPV (+); HPV-16/18 (+) includes HPV-16 (+) and/or HPV-18 (+), with or without other HPV genotypes (+); non-16/18 HR-HPV (+) includes HPV-16 (–) and HPV-18 (–), 12 other HR-HPV (+) with or without low-risk HPV (+) or 'HPV-other types' (+); HR-HPV (–) includes low-risk HPV (+) or 'HPV-other types' (+) or HPV (–); among all 1,102 cases, 113 cases were infected with multiple HPV genotypes, and they were classified as the group with a higher risk for its constituents; LSIL is a synonym for CIN 1, mild squamous dysplasia, flat condyloma, koilocytotic atypia or koilocytosis; HSIL includes CIN 2 or 3 or unclassified HSIL. †Out of these six cases, four cases were diagnosed as tic 3 after follow-up and re-biopsy; three were diagnosed as squamous cell carcinoma in re-biopsy after 5 months, 11 months, and 2 years; and one was diagnosed as CIN 3 in re-biopsy after 6 months. ‡After a review of this case, re-biopsy was recommended, but the patient was lost during follow-up.
2. Clinical performance of HPV 9G DNA chip test and cytology test
The sensitivity, specificity, PPV, and NPV of the HPV 9G DNA chip test and cytology test—with a cut-off ≥ASCUS for the detection of histology CIN 2 or worse—are shown in Table 3. The cytology test showed a higher sensitivity of 95.9% (95% CI, 91.7 to 97.0) compared to that of the HPV 9G DNA chip test, which was 86.3% (95% CI, 82.2 to 89.8). The HPV 9G DNA chip test showed a higher specificity of 60.0% (95% CI, 58.5 to 61.2) compared to that of the cytology test, which was 41.3% (95% CI, 40.1 to 42.0) (Table 3).
Table 3
Clinical usefulness of cytology and the HPV DNA genotyping test*

Values are presented as percentages (95% CI).
ASCUS, atypical squamous cells of undetermined significance; HPV, human papillomavirus; HR, high-risk.
*HR-HPV (+) includes HPV-16 (+) and/or HPV-18 (+) and/or 12 other non-16/18 HR-HPV (+); ≥ASCUS includes all cytology results that are ASCUS or worse; ≥cervical intraepithelial neoplasia (CIN) 2 includes CIN 2 or worse.
3. Risk estimates by the HPV genotyping result
For evaluating risk for ≥CIN 2 according to individual HPV genotypes, we excluded patients with multiple infections (n=113; including two cases with both HPV-16 [+] and HPV-18 [+]), and the remaining 989 patients were sorted into fourteen groups representing each genotype of HR-HPV (+) or into the HR-HPV (–) group. The age-adjusted odds ratio for ≥CIN 2 of each group is shown in Table 4. Among patients with HPV-16 (+) and those with HPV-18 (+), the odds ratios for ≥CIN 2 were 21.7 (95% CI, 13.5 to 34.8) and 8.0 (95% CI, 3.7 to 17.5), respectively, compared with patients who were HR-HPV (–). Among patients with the remaining 12 HR-HPV (+) genotypes, patients with HPV-31, -33, -35, -45, -51, -52, -56, -58, and -68 (+) showed statistically significantly higher odds ratios compared with patients who were HR-HPV (–).
Table 4
Age-adjusted odds ratio for ≥CIN 2 of each HR-HPV genotype*
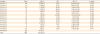
Values are presented as number (%).
CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; HR, high-risk.
*HR-HPV (–), as a control, includes low-risk HPV (+) or 'HPV-other types' (+) or HPV (–). Multiple infection cases (n=113) were excluded for evaluation of each risk of HR-HPV genotype.
†Odds ratio, age-adjusted odds ratio for ≥CIN 2.
For risk estimation for ≥CIN 2, we categorized all 989 patients with single HPV infections into the following three groups: HPV-16/18 (+), non-16/18 HR-HPV (+), and HR-HPV (–). The age-adjusted odds ratio for ≥CIN 2 in the HPV-16/18 (+) group compared with that in the HR-HPV (–) group was 18.2 (95% CI, 11.7 to 28.5; p<0.001), and the odds ratio in the non-16/18 HR-HPV (+) group compared with that in the HR-HPV (–) group was 6.6 (95% CI, 4.4 to 9.9; p<0.001) (Table 5, Supplementary Fig. 1). As a next step, we categorized these 12 groups of non-16/18 HR-HPV genotypes into two groups based on the odds ratios of each HPV genotype. We used the odds ratio of a group of HPV-18 (+) patients, which was 8.0, as a cut-off. Non-16/18 HR-HPV genotypes were divided accordingly as follows: one group as HPV-31/33/35/45/52/58 (+) and the other group as HPV-39/51/56/59/66/68 (+). In the end, all 989 patients were classified into four groups: HPV-16/18 (+), HPV-31/33/35/45/52/58 (+), HPV-39/51/56/59/66/68 (+), and HR-HPV (–). The odds ratios for ≥CIN 2 of each group are shown in Table 6. The age-adjusted odds ratio for ≥CIN 2 in the HPV-16/18 (+) group compared with the HR-HPV (–) group was 18.1 (95% CI, 11.6 to 28.3; p=0.003); the odds ratio in the HPV-31/33/35/45/52/58 (+) group compared with the HR-HPV (–) group was 11.9 (95% CI, 7.6 to 18.8; p<0.001); and the odds ratio in the HPV-39/51/56/59/66/68 (+) group compared with the HR-HPV (–) group was 2.4 (95% CI, 1.4 to 4.3; p<0.001) (Table 6, Supplementary Fig. 2). The 95% CIs of the odds ratio for the HPV-31/33/35/45/52/58 (+) group did not overlap with those of the HPV-39/51/56/59/66/68 (+) group.
Table 5
Age adjusted odds ratio for ≥CIN 2 of each HR-HPV group: HPV 16/18 (+) and non-16/18 HR-HPV (+)*

Values are presented as number (%).
CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; HR, high-risk.
*HPV-16/18 (+) includes HPV-16 (+) or HPV-18 (+); non-16/18 HR-HPV (+) or HPV-31/33/35/39/45/51/52/56/58/59/66/68 (+) includes HPV-16 (–) and HPV-18 (–), 12 other HR-HPV (+); HR-HPV (–), as a control, includes low-risk HPV (+) or 'HPV-other types' (+) or HPV (–). Multiple infection cases (n=113) were excluded.
†Odds ratio (OR), age-controlled odds ratio for ≥CIN 2.
Table 6
Age adjusted odds ratio for ≥CIN 2 of each HR-HPV group: HPV 16/18 (+) and the two stratified groups of non-16/18 HR-HPV (+)*

Values are presented as number (%).
CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; HR, high-risk.
*HPV-16/18 (+) includes HPV-16 (+) or HPV-18 (+); non-16/18 HR-HPV (+) includes HPV-16 (–) and HPV-18 (–), 12 other HR-HPV (+); 12 non-16/18 HR-HPV (+) were divided into two groups, one including HPV-39 (+) or HPV-51 (+) or HPV-56 (+) or HPV-59 (+) or HPV-66 (+) or HPV-68 (+), and the other including HPV-31 (+) or HPV-33 (+) or HPV-35 (+) or HPV-45 (+) or HPV-52 (+) or HPV-58 (+); HR-HPV (–), as a control, includes low-risk HPV (+) or 'HPV-other types' (+) or HPV (–). Multiple infection cases (n=113) were excluded.
†Odds ratio, age-controlled odds ratio for ≥CIN 2.
DISCUSSION
Because HR-HPV infection is a necessary cause of cervical cancer, tests for HR-HPV have been proposed as an adjunctive tool to cervical cytology [16]. In our study, we evaluated whether there are differences in risk among 12 non-16/18 HR-HPV genotypes. There are a number of commercial HPV tests, including nucleic acids hybridization assays, such as in situ hybridization; signal amplification assays, such as Hybrid Capture 2 (Qiagen, Gaithersburg, MD); and nucleic acids amplification, such as microarray and PCR (Cervista [Hologic, Bedford, MA, USA], Cobas 4800 HPV test [Roche Molecular Systems Inc., Pleasanton, CA, USA], and APTIMA [Gen-Probe, San Diego, CA, USA]) [17]. Among them, 9G DNA chip technology is based on the phenomenon of molecular recognition to immobilize oligonucleotides for the production of DNA chips. The 9G probes are immobilized by multiple interactions of the nine consecutive guanines on the aminomethylcoumarin acetate (AMCA) monolayer [14]. The HPV 9G DNA chip test, which has been approved by the Korea Food and Drug Administration (KFDA), displays a promising diagnostic characteristic of 100% clinical sensitivity and specificity, making it a promising diagnostic tool for HPV genotyping [1518]. Considering concordance rate between HPV 9G DNA test and Cobas 4800 HPV test which was approved by FDA, both tests were agreed in 97.2% for detecting HPV-16 and -18. HPV 9G DNA test seemed effective in detecting high risk HPV [19].
In our study, the cytology test showed a higher sensitivity of 95.9% (95% CI, 91.7 to 97.0) compared to that of the HPV 9G DNA chip test, which was 86.3% (95% CI, 82.2 to 89.8) and the HPV 9G DNA chip test showed a higher specificity of 60.0% (95% CI, 58.5 to 61.2) compared to that of the cytology test, which was 41.3% (95% CI, 40.1 to 42.0) (Table 3). These results are opposite of previous findings, which show generally higher sensitivity of HPV test than that of cytology test and lower specificity of HPV test than that of cytology test [20]. It is probably due to different study population such as age and regional distribution. Furthermore, we suspect that there is possibility that a clinician had scraped the cervix less extensively, because he might have been aware of abnormal cytology result from referred clinics. Too small specimen might give more negative influence to the result of cytology than HPV DNA test.
Previous studies reported that some genotypes of high risk HPV are strongly associated with high grade cervical lesions (≥CIN 2). According to Cervical Lesions Observed by Papillomavirus types-A Research in Europe II (CLEOPARE II) study, 12 HPV types were associated with high grade cervical lesion, of which especially HPV-16, -18, -31, -33, -35, -45, -51, -52, and -58 were important in Portugal women [21]. Similarly, HPV-16 was the most strongly associated with ≥CIN 3 cervical lesion and 60.6% of high grade cervical lesions were associated with HPV-31, -33, -45, -52, or -58 in French women [22]. A multicenter, prospective study to evaluate the prevalence of HPV types in Asian women with invasive cervical cancer showed that HPV-16, -18, -52, -45, -58, -33, or -31 were strongly associated with cervical cancer. Among them, HPV-33 was prevalent in Korean cervical cancer women than other Southeast Asian women [13]. These results were similar to our study. In our study, we obtained a statistically significant, age-adjusted odds ratio for ≥CIN 2 for each HR-HPV genotype, except the HPV-39, -59, and -66 genotypes (Table 4). Among the groups of HPV-39, -59, and -66, only five patients were ≥CIN 2. The age-adjusted odds ratio of patients with HPV-16 (+) was 21.7 (95% CI, 13.5 to 34.8) and that of patients with HPV-18 (+) was 8.0 (95% CI, 3.7 to 17.5). We used the odds ratio of a group of HPV-18 (+) patients, which was 8.0, as a cut-off, to categorize the 12 non-16/18 HR-HPV genotypes into the HR group and the LR group. Non-16/18 HR-HPV genotypes were divided accordingly as follows: HPV-31/33/35/45/52/58 (+) and HPV-39/51/56/59/66/68 (+). Non-16/18 HR HPV (+), which initially showed an odds ratio for ≥CIN 2 of 6.6 (95% CI, 4.4 to 0.9) as a whole, showed stratified odds ratios when divided into these two groups: 11.9 (95% CI, 7.6 to 18.8) for HPV-31/33/35/45/52/58 (+) and 2.4 (95% CI, 1.4 to 4.3) for HPV-39/51/56/59/66/68 (+). Although the current guidelines do not reflect this difference in risk, the higher risk HPV-31/33/35/45/52/58 genotypes might need more aggressive actions, such as direct colposcopy, rather than follow-up after 12 months. Large scale clinical trials or cohort studies are necessary especially in Asia, where cervical cancer prevalence is high and where HPV genotyping has been widely used in routine screening. This study has some limitations, (1) the study has a retrospective design based on the pathology archive database records. Selection bias may have occurred because we excluded some subjects with missing data. (2) It is single institution study of referral hospital and has small sample size; therefore, this study may not represent general population. Future prospective studies with larger sample size are needed to confirm our study.
In conclusion, the HPV 9G DNA chip test is a useful tool to detect patient with ≥CIN 2, in addition to cytology test. Furthermore, the 12 non-16/18 HR-HPV genotypes obtained from HPV 9G DNA chip test can be further categorized (HPV-31/33/35/45/52/58 vs. HPV-39/51/56/59/66/68) by risk stratification. The HPV-31/33/35/45/52/58 genotypes might need more aggressive action. Large scale clinical trials or cohort studies are necessary to confirm our suggestion.
 XML Download
XML Download