

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uterine carcinosarcomas (UCSs), also called malignant mixed Müllerian tumors (MMMTs) of the uterus, are a rare but aggressive form of endometrial cancer, comprising both malignant epithelial and mesenchymal components. The mesenchymal component is either homologous or heterologous. Homologous sarcoma comprises tissue that is native to the Müllerian duct, such as endometrial stromal sarcoma, fibrosarcoma or leiomyosarcoma. Cartilaginous, osteosarcomatous, liposarcomatous, and rhabdomyosarcomatous differentiations are commonly observed in heterologous elements. Although UCS accounts for less than 5% of all uterine malignancies, the 5-year overall survival (OS) rate for this subtype is extremely low, ranging from 10% to 47% [123].
UCS was traditionally classified in the sarcoma category because of the sarcomatous component. However, molecular and genetic research has demonstrated that UCS is distinct from sarcoma, and the carcinomatous component induces the observed tumor aggressiveness and metastasis. Recent data have suggested that the origin of UCS is monoclonal, and UCS should be best categorized as a de-differentiated uterine carcinoma rather than as a sarcoma [45]. Furthermore, evidence showed that UCS metastasizes via the lymphatic system instead of the blood system, which is the primary pattern of spread in sarcoma subtypes. As a result, the International Federation of Gynecology and Obstetrics (FIGO) 2009 staging guidelines suggest that UCS should be staged according to carcinomas of the endometrium [6].
MATERIALS AND METHODS
In the present study, we performed a retrospective analysis including 60 UCS and 115 grade 3 endometrioid endometrial carcinoma (G3EC) consecutive patients who underwent primary surgery between February 2006 and August 2013 at Fudan University Shanghai Cancer Center. Patients who underwent secondary cytoreductive surgery were excluded. Informed consent was obtained from all individual participants included in the present study. Gynecologic pathologists reviewed all pathological slides to confirm the diagnosis.
We retrospectively collected demographic and clinicopathological data from the medical records, which included age at diagnosis, parity, menopause state, body mass index (BMI), presence of ascites fluid, tumor stage, family history of malignancy, pretreatment cancer antigen 125 serum level, tumor size, myometrial invasion, lymph-vascular space involvement (LVSI) and nerve invasion, and lymph node metastasis.
The data on surgical procedures and adjuvant treatment were also analyzed. Twenty-three UCS and 38 G3EC patients with stage IIIc-IVb diseases received cytoreductive surgery. Optimal cytoreduction was defined as tumors with the maximal diameter of the largest residual tumor nodule measuring less than 1 cm at the completion of the primary operation. OS was evaluated and defined as the time between the dates of diagnosis and death by the tumor or the last follow-up visit.
Survival curves were calculated using the Kaplan-Meier method. Kaplan-Meier survival curves were generated, and the survival differences were quantified using the log-rank test (univariate analysis). The Cox regression model (multivariate analysis) was used to analyze independent prognostic factors. Forest plots were introduced as subgroup analyzes for comparing the prognostic differences between these two malignant endometrial carcinomas (EC). Statistical tests were considered significant at p<0.05. All analyzes were performed using SPSS ver. 20.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Demographic and clinical features
The median ages of UCS and G3EC patients at diagnosis were 59.5 years (interquartile range [IQR], 53 to 61 years) and 56 years (IQR, 55 to 66 years), respectively, and the values showed statistical significance (p=0.019). Among all patients participating in the present study, 49 UCS patients (81.7%) and 85 G3EC patients (73.9%) experienced menopause, without significant difference (p=0.250). Of the UCS and G3EC patients, the median BMI values were 20.7 kg/m2 (range, 16.2 to 31.5 kg/m2) and 22.5 kg/m2 (range, 15.4 to 33.4 kg/m2), respectively (p>0.05).
Both UCS and G3EC patients had chief complaints of abnormal vaginal bleeding and/or vaginal discharge. Three UCS (5.0%) and five G3EC patients (4.3%) complained of hypogastric pain; fatigue and anorexia were observed in one UCS patient (1.7%) and three G3EC patients (2.6%). Ascites fluid was observed in 33 UCS and 18 G3EC patients (p<0.001) (Table 1).
Table 1
Comparison in clinicopathological characteristics between UCS and G3EC

2. Treatment
Radical/subradical abdominal hysterectomy was the first choice of therapy in all patients with uterine malignancies. Fifty-one UCS patients (85.0%) accepted additional pelvic lymphadenectomy, and 34 patients (56.7%) accepted para-aortic lymphadenectomy when suspected intraoperatively. Among the G3EC patients, 107 patients (93.0%) received pelvic lymphadenectomy and/or omentectomy, and para-aortic lymphadenectomy was conducted in 102 patients (88.7%). Among all of the patients, 23 UCS (45.1%) and 38 G3EC patients (33.0%) had stage IIIc-IVb diseases and received additional cytoreduction surgery, whereas 31 patients (50.8%) received additional extensive surgical procedures, including omentectomy (n=27), appendectomy (n=18), rectum resection (n=1), and peritoneal stripping (n=1). Complete gross resection (R0) was achieved in 36 patients (59.0%), whereas 16 (26.2%) were left with residual diseases, showing tumor nodule diameters of no more than 1 cm, and nine patients (14.8%) were left with residual diseases, showing tumor nodule diameters of more than 1 cm. Patients who accepted complete gross resection had a 3-year OS of 70.1% (SD, 7.9%), and those with gross residual diseases with tumor nodules of ≤1 and >1 cm had a 3-year OS of 45.0% (SD, 13.2%) and 13.3% (SD, 12.3%; p<0.001), respectively. For UCS patients, the 3-year OS rate of the R0 and residual disease groups was 53.7% (SD, 18.7%) and 18.8% (SD, 15.8%), respectively (p=0.030), and the 3-year OS rate of the R0 group and residual G3EC disease group was 69.6% (SD, 9.6%) and 40.0% (SD, 12.6%), respectively (p=0.088).
Adjuvant therapy, including chemotherapy (CT) and radiotherapy (RT), was performed in uterine malignancies. The major CT regimens comprised paclitaxel-carboplatin (n=30), ifosfamide-cisplatin (n=9), doxorubicin (n=11), and others (n=4). Patients receiving carboplatin-paclitaxel and sarcoma-sensitive regimens, including ifosfamide-cisplatin and doxorubicin, had a 5-year OS of 53.2% (SD, 12.9%) and 30.8% (SD, 13.1%), respectively (p=0.020). Among the 57 UCS patients receiving adjuvant therapy, three patients (5.3%) received adjuvant RT, 28 patients (49.1%) received adjuvant CT, and 26 patients (45.6%) received adjuvant CT with RT. The 3- and 5-year OS in patients receiving multimodal therapy were 78.8% and 71.0%, respectively, compared with 59.7% and 35.8% in patients receiving adjuvant RT or CT alone, respectively (p=0.028). Among the G3EC patients, 54 patients (47.0%) received adjuvant RT and 59 patients (51.3%) received adjuvant CT. Thirty-seven G3EC patients received RT with CT, but there was no correlation with significantly improved OS.
3. Pathological characteristics
Among all 60 UCS patients, 37 patients (61.7%) were at stage I/II, and 23 patients (38.3%) were at stage III/IV, whereas 73 G3EC patients (63.5%) were at stage I/II, and 42 G3EC patients (36.5%) were at stage III/IV. There was no significant statistical difference between UCS and G3EC patients in stage distribution.
The average diameter of the largest tumors observed in UCS and G3EC patients were 4.6 cm (range, 0.3 to 14.0 cm) and 4.0 cm (range, 0.3 to 11.0 cm), respectively, and these values showed significant statistical differences (p=0.046). Twenty-six UCS (43.3%) and 70 G3EC patients (60.9%) had myometrial invasion ≥1/2, and a significant statistical difference was observed (p=0.027). Adnexal metastasis was observed in 12 UCS (20.0%) and 10 G3EC patients (8.7%; p=0.048).
A heterologous mesenchymal component was observed in 12 patients (20.0%), and a homologous component was observed in 44 patients (73.3%). The 3- and 5-year OS rates for patients with the homologous component were 85.2% and 68.1%, respectively, whereas these rates were 38.9% and 19.4%, respectively for patients with heterologous tumors (log-rank test, p<0.001 for 5-year OS).
4. Overall survival
With a median follow-up period of 49.2 months (range, 2.9 to 110.1 months) for surviving patients, nine G3EC patients (7.8%) were lost to follow-up, and 45 patients died from cancer (20 died from carcinosarcoma and 25 died from G3EC). The 3- and 5-year OS rates were 70.5% and 54.2% for UCS patients and 80.0% and 76.8% for G3EC patients (log-rank test, p=0.040 for 5-year OS) (Fig. 1), respectively. After adjusting based on FIGO stage, patients with early stage (FIGO I & II) diseases had 5-year OS rates of 67.7% and 92.4% for UCS and G3EC, respectively (log-rank test, p=0.020 for 5-year OS). Patients with advanced stage (FIGO III & IV) diseases had 5-year OS rates of 29.6% and 49.7% for UCS and G3EC, respectively (p=0.421).
Fig. 1
Overall survival (OS) curve of uterine carcinosarcoma (UCS) and grade 3 endometrioid endometrial carcinoma (G3EC) patients. The 3-year and 5-year OS rate for UCS were 70.5% and 54.2%, 80.0% and 76.8% for G3EC.

The subgroup analysis of the prognostic factors between the two malignancies was performed (Fig. 2). Using a forest graph, we observed that UCS patients presented worse OS than G3EC patients in the following subgroups, showing significant statistical differences: age of <60 years at diagnosis (p=0.032), menopause (p=0.022), absent ascites fluid (p=0.001), tumors with early stages (stage I–II, p=0.035), no vaginal invasion (p=0.014), no lymph node metastases (p=0.006), and adjuvant CT/RT (p=0.044).
Fig. 2
Subgroup analysis of the prognostic factors between the uterine carcinosarcoma (UCS) and grade 3 endometrioid endometrial carcinoma(G3EC).
UCS patients exhibited worse overall survival (OS) than G3EC patients in such specific subgroups: patients who were diagnosed at age less than 60 years (P=0.032), with postmenopausal status (P=0.022), without ascites fluid (P=0.001), tumor with early stage (stage I-II, P=0.035), without vagina invasion (P=0.014), without lymph node metastases (P=0.006), and with adjuvant chemo/radiotherapy (P=0.044).

5. COX regression analysis
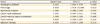
Potential prognostic factors were examined using the multivariate analysis to determine the correlated factors. As shown in Table 2, carcinosarcoma histological type (hazard ratio [HR], 2.4; 95% CI, 1.0 to 5.6; p=0.039) and FIGO stage (HR, 4.9; 95% CI, 1.4 to 16.6; p=0.010) were the two independent factors for OS, after adjusting based on myometrial invasion, lymph node involvement, LVSI, tumor volume, and adjuvant CT/RT. These results further suggested that UCS patients have particularly poor outcomes.
Table 2
Multivariate analysis of prognostic factors for overall survival by Cox proportional hazards models
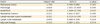
To consolidate the results of the present study, the Cox proportional hazards model was also used to evaluate prognostic factors in both UCS and G3EC. Carcinosarcoma patients with advanced stage diseases (p=0.012), adnexal involvement (p=0.021), LVSI and nerve invasion (p=0.005), lymph node metastases (p=0.039), adjuvant RT (p=0.037), and heterologous subtype (p=0.001) exhibited worse OS (Table 3). However, only the histological subtype (heterologous vs. homologous subtype, HR, 4.6; 95% CI, 1.4 to 15.8; p=0.014) was identified as an independent prognostic factor for OS in the multivariate analysis (Table 4).
Table 3
Univariate analysis of factors associated with overall survival in UCS and G3EC

Table 4
Prognostic factors of uterine carcinosarcoma analyzed by Cox proportional hazards models

G3EC patients with ascites fluid (p=0.003), advanced disease (p<0.001), adnexal involvement (p=0.043), vaginal involvement (p=0.027), LVSI and nerve invasion (p<0.001), and lymph node metastases (p<0.001) were correlated with worse OS (Table 3). The multivariate analysis (Table 5) revealed that tumor stage (HR, 5.9; 95% CI, 1.0 to 33.9; p=0.046) and ascites fluid (HR, 5.1; 95% CI, 1.1 to 22.7; p=0.032) were independent prognostic factors for OS.
Table 5
Prognostic factors of grade 3 endometrioid endometrial carcinoma analyzed by Cox proportional hazards models
DISCUSSION
UCS has been previously categorized as a subtype of uterine sarcoma and was listed among the MMMT (carcinosarcomas) in the 2003 World Health Organization classification of tumors of the female genital tract. UCS has been traditionally classified as a sarcoma subtype, reflecting the presence of a sarcomatous component, invasive tumor spread, and poor survival compared with pure epithelial EC. However, subsequent studies have demonstrated that factors associated with excess estrogen exposure, BMI and the propensity for lymphatic spread were common features of both MMMT and high-grade EC [7]. A similar disease pattern, showing sensitivity to CT in immunohistochemical and molecular studies, has also been reported in studies of UCS and high-grade EM [891011]. Indeed, the revised FIGO 2009 staging system distinguished UCS from other uterine sarcomas, and classified this disease together with EC, reflecting similar risk factors shared by both neoplasms. Nevertheless, there remain doubts that challenge the same FIGO system in clinical practice.
Although the increased risk of recurrence and mortality is associated with high-risk EC subtypes, there are few studies comparing the MMMT subtype to high-grade EM in large cohorts. In the present study, we reported that patients with carcinosarcoma had worse survival outcomes compared with G3EC patients. When stratified according to stage, similar findings were observed in patients with early- and advanced-stage diseases. After adjusting for other confounding factors, the multivariate analysis revealed that carcinosarcoma subtype was an independent prognostic factor for poor OS. These findings are consistent with those of previous studies, which also reported survival differences between UCS and high-grade EM cases [312]. A SEER (Surveillance, Epidemiology and End Results) study reported that high-grade EM cases had significantly better OS than UCS cases after adjusting for age, race, lymph node dissection, stage, and postoperative RT [3]. Similarly, Bland et al. [12] conducted a retrospective study, reporting that UCS patients had a significantly shorter progression-free survival (23 months vs. 57 months, p=0.001) and OS (55 months vs. 92 months, p=0.001) compared with patients with high-grade endometrial cancer. Zhang et al. [13] also recently reported that UCS patients had significantly worse outcomes (OS, disease-specific survival, and recurrence-free survival) compared with high-grade EC cases.
Whether the behavior of UCS is the same as high-grade EC remains under debate. However, the results of the present study confirmed that UCS exhibits more aggressive behavior and worse outcome than G3EC. To determine which factors might contribute to this distinct behavior, we compared the demographic and clinicopathological features between UCS and G3EC patients. Compared with G3EC, UCS patients were diagnosed at an older age. In addition, a higher incidence of ascites fluid and adnexal involvement and larger tumor volume were demonstrated in carcinosarcoma, indicating that UCS exhibits more aggressive behaviors. In the present study, the propensity for lymphatic spread between UCS and G3EC did not obviously differ (p>0.05), and was consistent with previous studies [714]. We observed that 16.7% of UCS cases had positive pelvic lymph node involvement and only 6.7% of UCS cases had positive para-aortic lymph nodes, compared with 23.5% and 12.2%, respectively, of G3EC cases. The unifying characteristic in lymphatic spread might reflect the fact that 20% of UCS patients did not have a lymph node examination, compared with 7.8% of G3EC cases, which might have contributed to the low prevalence of positive lymph node involvement in this subgroup.
The present study is unique in that we observed a significant difference in OS between UCS and G3EC patients using subgroup analysis. Although previous studies have reported that UCS patients have poorer survival, only a few studies stratified specific factors in which UCS exhibit worse outcomes compared with high-grade EC. In the following subgroups, including age at diagnosis of less than 60 years, postmenopausal women, negative ascites fluid, stage II tumors, negative vaginal involvement, negative lymph node involvement and adjuvant therapy, UCS patients presented significantly worse outcomes compared with G3EC patients. The specific subgroup analysis could explain why UCS patients had a relatively higher incidence of aggressiveness and modality compared with G3EC patients.
Previous studies have demonstrated that older age, LVSI, deep myometrial invasion, cervical stromal involvement, and advanced tumor stages represent significant adverse prognostic factors for carcinosarcoma [1516]. In the present study, UCS patients with advanced stage, adnexal involvement, LVSI and nerve invasion, lymph node metastases, adjuvant RT, and heterologous subtype had a worse OS in the univariate analysis. However, notably, the present study showed that only histological subtype was identified as an independent prognostic factor for OS in the multivariate analysis. We compared the outcomes of UCS patients with homologous elements and heterologous subtype diseases and there was a statistically significant difference in the 5-year OS. There was a statistically significant difference in the 5-year OS survival between the two groups (68.1% vs. 19.4%, p<0.001), which was consistent with the results of Hellstrom et al. [17]. A similar result was reported in a study of 42 stage I UCS patients after primary surgery. The presence of heterologous sarcomatous elements is a powerful negative prognostic factor, with a 3-year OS rate of 45% versus 93% in homologous patients (p<0.001) [18].
In the absence of standard guidelines specific for UCS, surgery is the mainstay treatment, and the initial recommended surgical treatment is the same for aggressive endometrial cancer: abdominal hysterectomy with bilateral salpingo-oophorectomy, peritoneal cytology and the removal of pelvic and aortic lymph nodes and omental biopsy. Advanced diseases should receive additional cytoreductive surgery. Lymphadenectomy is an important surgical procedure, not only diagnostic, but also therapeutic, for both early and advanced stage diseases. In the present study, the 5-year OS was 54.6% versus 52.5% for UCS patients receiving (n=48) versus patients without lymphadenectomy (n=12). Although no statistical significance was observed (p>0.05), a tendency towards improved survival was seen in patients with lymphadenectomy. Similar results were reported in a SEER retrospective analysis of stage I-III UCS, and Nemani et al. [19] reported that the 5-year OS was 33.4% versus 35.8% for patients with versus without lymphadenectomy, respectively.
Postoperative treatments for UCS have included RT, CT and the combination of CT and RT. The recommended chemotherapeutic regimen, based on retrospective studies, involves platinum-based CT, including carboplatin-paclitaxel or ifosfamide-cisplatin, with less toxicity and improved survival outcome. These results also demonstrated an advantage favoring the use of paclitaxel-carboplatin compared with the cisplatin-ifosfamide combination. Several studies have shown favorable outcomes in carcinosarcoma patients treated with carboplatin-paclitaxel and recommended this regimen as a first-line treatment [2021]. Radiation therapy is intended to improve local control, particularly in early-stage cancers. Nevertheless, there has been sparse evidence to prove that this treatment extends survival [2223]. In the present study, we observed that adjuvant RT with CT was predictive of better survival in UCS patients compared with individuals receiving CT or RT alone. Gungorduk et al. [24] conducted a retrospective review of three cancer centers involving 66 UCS patients, noting that adjuvant CT with RT is associated with improved OS compared with CT or RT alone (HR, 3.3; 95% CI, 0.7 to 15.0; p=0.01), consistent with the results of the present study. We collected a larger number of cases and prospective trials warranting the evaluation of the effectiveness of multimodal therapy in UCS patients.
The major strengths of the present study included reliable data from a single cancer center, a large sample size of cases, and adjustments for other prognostic factors. Furthermore, we explored specific prognostic factors via subtype analysis to evaluate potential effect modifications. Potential limitations include the retrospective study design and lack of generalizability to nonsurgical cases, reflecting the inclusion of initial surgical cases in the present analysis.
In conclusion, these data suggested that UCS patients exhibited significant differences in clinicopathological characteristics compared with G3EC patients, and UCS patients had worse outcomes than G3EC patients. Tumor stage was identified as an independent adverse prognostic factor. Given the distinct survival differences shown in the present study, it is reasonable to conclude that UCS should be distinct from endometrial endometrioid carcinomas and regarded as a special subtype of high-risk EC. In addition, future studies should explore the molecular biology of carcinosarcoma not only to increase the current understanding of the carcinogenesis of these tumors but also to identify potential molecule-targeted treatments for use in the treatment of these diseases.
 XML Download
XML Download