

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The patterns of healthcare utilization change in infectious disease outbreaks. Identifying the patterns of change is important for future preparedness and response. The effects on healthcare utilization of infectious disease epidemic depend on the characteristics of an infection. In the 2003 severe acute respiratory syndrome (SARS) epidemic in Taiwan, medical service utilization decreased due to fear of nosocomial transmission.12 However, in the 2009 pandemic of H1N1 influenza, which is highly infectious but has a low case-fatality rate, emergency care utilization increased.34
In 2015, South Korea (hereafter “Korea”) experienced an epidemic of Middle East respiratory syndrome (MERS). In a vulnerable healthcare delivery system in which the gatekeeper function of primary clinics was weak, the first patient wandered through several different hospitals before being diagnosed, thereby spreading the infection.5 The 14th patient, a super-spreader, stayed in an overcrowded emergency room (ER) in a tertiary-care hospital for 3 days and spread the infection to 78 patients.6 An healthcare-associated MERS epidemic then started and the fear of MERS spread nationwide.678 A 14-day self-isolation quarantine program was applied to contacts of infected patients, while there was no restriction on the public's access to medical care.89 However, Korean citizens were afraid to visit healthcare facilities due to fears regarding the potential nosocomial transmission of this unfamiliar contagious disease. Such fears affected the entire society, and all healthcare utilization reportedly decreased.
In order to effectively respond to emerging infectious disease outbreaks, it is important to predict changes in healthcare utilization and understand the different patterns of changes in diverse population groups. Previous studies have analyzed the impacts of SARS and influenza epidemics.2341011 However, although few small studies have investigated changes in healthcare utilization during the MERS epidemic in Korea,1213 no study has systematically evaluated the impact of the MERS epidemic on nationwide healthcare utilization. Furthermore, the impact of the reduction in emergency care utilization on health outcomes has not been explored.
The hypothesis of this study was that the use of emergency care during the MERS epidemic decreased regardless of age, sex, and socioeconomic position (SEP), but with a less prominent impact for severe diseases, meaning that the final health outcomes of emergency care showed minimal changes. We aimed to investigate the changes in emergency care utilization during the 2015 MERS epidemic according to patient characteristics, disease severity, and region, and evaluate its impact on mortality.
MATERIALS AND METHODS
Study setting and databases
The population of Korea is approximately 50 million people, spread over an area of 99000 km2. The administrative units of Korea include eight metropolitan cities and nine provinces that are divided into cities and counties. Korea implemented National Health Insurance (NHI) in 1989, covering the entire population. The Korean government runs NHI as a single insurer, compulsorily covering inpatient, outpatient, and emergency services.1415 While NHI service ensures high accessibility to medical care, the gatekeeper function of primary clinics is weak, meaning that people can visit tertiary-care hospitals freely, with low out-of-pocket costs. Korea has a total of 420 registered ERs, which are open to all beneficiaries without restriction, and overcrowding of ER is a serious problem in tertiarycare hospitals.1617
The National Health Information Database (NHID) from NHI Service was analyzed.1518 The eligibility database (DB), healthcare utilization DB, and death information DB contained within NHID were used for this study. The eligibility DB (patients' demographic information) included age, sex, and insurance premium as an indicator of SEP.19 The healthcare utilization DB contained insurance service fee codes and diagnostic codes. The total number of diagnostic codes was five, including one principal code, one secondary code, and three additional diagnostic codes, based on the International Classification of Diseases, 10th edition. All healthcare use covered by NHI was included in the NHID, but cases involving traffic accidents covered by auto insurance (accounting for approximately 2.6% of total healthcare use) and cases involving foreigners not covered by the Korean NHI were excluded.141820 We individually linked the eligibility DB and healthcare utilization DB with the death information DB, including date of death, to investigate the mortality after ER visits.
MERS outbreak in Korea and study population
On May 20, 2015, the first MERS case in Korea was identified in a traveler from the Middle East. From May 20, when the first patient was diagnosed, to July 5, when the last patient was diagnosed, a total of 186 patients were confirmed, with a 20% mortality rate.2122 Although some hospitals were closed temporarily for quarantine purposes, there was no restriction on the use of medical services. However, activities in all sectors of society, including health service utilization, decreased. Social cost of the MERS epidemic was estimated to be 8.3 billion USD.23
All patient visits to ER between January 2014 and December 2016 were examined. Cases for which data regarding the age and sex of the insured and insurance premium were not confirmed were minimal (0.097% of total visits), and such cases were excluded from the analysis. The official end date of the MERS epidemic, according to the criteria of World Health Organization, was December 23, which came 80 days after the last death. However, the period of the 2015 MERS epidemic was defined as June to July 2015, corresponding to the period when new patients were diagnosed and the fear of MERS was prevalent. The peak was June 2015, when most number of new patients were diagnosed.
Measurement of variables
Patients were divided into three age groups: children (0–19 years), adults (20–59 years), and the elderly (over 60). SEP was classified into quintile groups using an insurance premium.19
Based on the first two diagnostic codes (principal and secondary codes), we selected several major diseases in ER and classified them to high-acuity and low-acuity diseases, based on whether their treatment could be initiated at the primary care settings rather than ER.24 High-acuity diseases included cardiac arrest (I46), myocardial infarction (MI; I21–22), hemorrhagic stroke (I60–62), and ischemic stroke (I63–64).25 Low-acuity diseases included acute gastroenteritis (AGE; A08–09), acute pharyngotonsillitis (APT; J00), acute otitis media (AOM; H65–67), and upper respiratory infection (URI; J00–06).124
The regions where the MERS outbreak mainly occurred (i.e., Seoul metropolitan city and Gyeonggi Province) were defined as risk areas and were compared with other regions. In Gyeonggi Province, Suwon, where the infection control hospital is located, and Pyeongtaek, where the first patient was diagnosed, were defined as high-risk areas, while Anyang and Seongnam, which are similar to Suwon and Pyongtaek in terms of population size and number of ER visits, were defined as comparison areas.
The first outcome was the monthly number of ER visits. To assess the degree of reduction in ER visits, the ratio of ER visits in 2015 to the averaged visits from the same month in 2014 and 2016 was calculated as follows and presented as a percentage (%):

The second outcome was the monthly number of deaths within 7 days of an ER visit, which was calculated as follows and presented as a percentage (%): ratio of deaths in 2015 to averaged deaths of the corresponding months in 2014 and 2016.
Statistical analyses
The MERS epidemic can be considered as a natural experiment. The periods of the MERS epidemic were considered as the intervention group, and other months were considered as the comparison group. In addition to the investigation of monthly trends from 2014 to 2016, the monthly numbers of ER visits in 2015 were compared with the average visits of the corresponding months in 2014 and 2016 (ratio of ER visits in 2015, %). The monthly number of deaths within 7 days of an ER visit was analyzed in the same manner. This analytical choice was based on the assumption that the monthly statistical figures in 2015 would have been similar to the averages from 2014 and 2016 in the absence of important events or policies affecting monthly visits and associated mortality.
In addition, age-standardized prevalence and their 95% confidence intervals (CIs) per 100000 population were calculated for the ER visits and deaths within 7 days of an ER visit in 2015. The number of health insurance subscribers was used as the denominator,26 and mid-year population in 2016 was used as the standard population.27 Prevalence ratios and their 95% CIs were also calculated using the averaged value from the same month in 2014 and 2016 as reference.
Changes in emergency care utilization patterns were compared by age, sex, and SEP [quintile of insurance premium: Q1 (lowest) to Q5 (highest)]. The reductions in ER visits for high-acuity and low-acuity diseases were presented as percentages (%) comparing risk areas with comparison areas. The ratios of monthly ER visits in 2015 to the averaged visits from the same month in 2014 and 2016 were compared according to disease severity, and we performed chi-square test to assess whether the differences of monthly ER visits between 2015 and 2014/2016 were statistically significant. All other results were graphically displayed to identify monthly trends throughout the year, and we considered the values during the MERS epidemic to be meaningful if they were outside the range of values for the other months.
Data management and statistical analyses were conducted using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics statement
The protocol of this study was reviewed and approved by the Institutional Review Board of Seoul National University Hospital (No. C-1804-041-934). Data use of this study was also approved by the National Health Insurance Service of Korea (Study No. NHIS-2018-1-153). No personal identifiers were provided in the data; instead, only anonymized aggregate data were used for the final analysis.
RESULTS
Overall emergency room visits according to the MERS epidemic
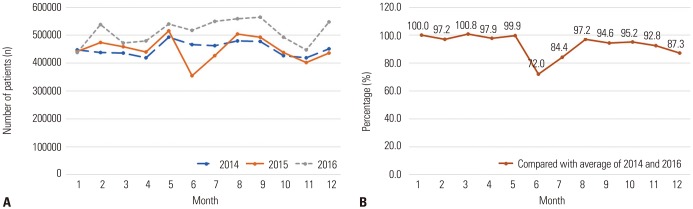
ER visits rose from 2014 to 2016, as shown graphically in Fig. 1. At the peak of the MERS epidemic in June 2015, the number of ER visits sharply declined by 28.0%, reaching 72.0% of the average visits in 2014 and 2016 (Fig. 1, Supplementary Table 1, only online). Except for June and July, the ratio of ER visits in 2015 ranged from 87.3% to 100.8%. The MERS epidemic resulted in a marked reduction in ER visits regardless of age, sex, and SEP, especially in pediatric patients (39.6%, 21.9%, and 24.9% decreased in children, adults, and the elderly, respectively) (Supplementary Table 2, Supplementary Fig. 1, only online).
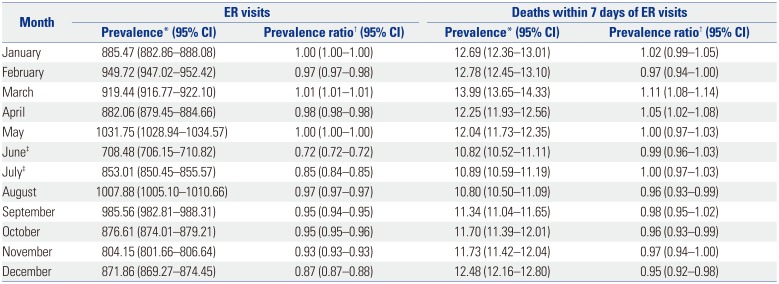
The age-standardized prevalence ratios for ER visits per 100000 population in June 2015 was 0.72, which was lower compared to the rest of the year (0.85 to 1.01) (Table 1).
Emergency care utilization according to disease severity
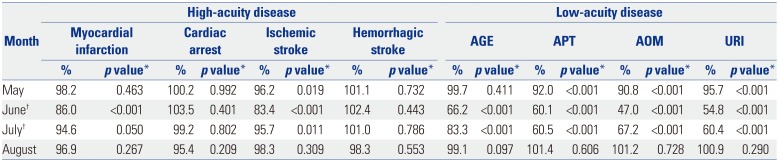
At the peak of the MERS epidemic, the ratio of ER visits due to low-acuity diseases decreased more sharply than that of ER visits due to high-acuity diseases (33.8%, 39.9%, 53.0%, and 45.2% decreased in AGE, APT, AOM, and URI, respectively versus a 14.0% decreased for MI and a 16.6% decreased for ischemic stroke). ER visits due to the highest-acuity diseases, cardiac arrest and hemorrhagic stroke, did not decrease during the MERS outbreak (with ratios of 103.5% for cardiac arrest and 102.4% for hemorrhagic stroke) and showed similar trends throughout the year (Table 2, Supplementary Table 3, Supplementary Figs. 2 and 3, only online).
Emergency care utilization by region
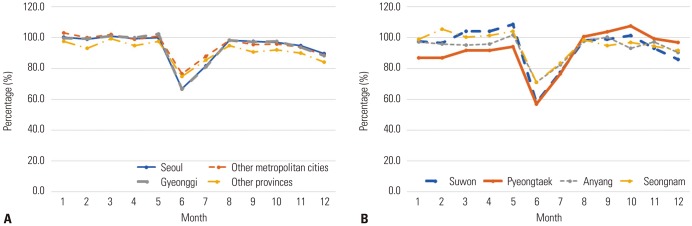
At the peak of the MERS epidemic, the reduction in emergency care use was more prominent in the risk areas than in other metropolitan cities and provinces (66.9% in Seoul and 66.7% in Gyeonggi Province versus 76.7% in other metropolitan cities and 75.0% in other provinces). In Gyeonggi Province, the reduction was more prominent in high-risk areas than in comparison areas (58.1% in Suwon and 56.8% in Pyeongtaek versus 71.0% in Anyang and 71% in Seongnam) (Fig. 2, Supplementary Table 4, only online).
Effect of reduction in emergency care utilization on short-term mortality
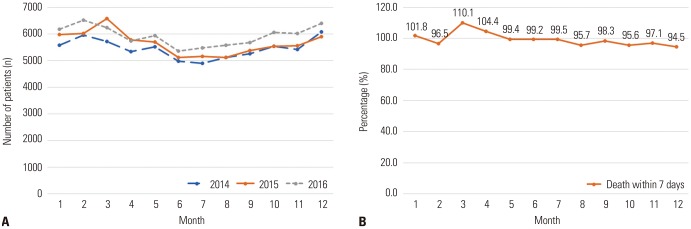
No substantial changes were detected in the number of deaths within 7 days after an ER visit throughout the year (December: 94.5% to March: 110.1%), including the MERS epidemic period (June: 99.2% and July: 99.5%) (Fig. 3, Supplementary Table 5, only online). The death trends within 7 days of an ER visit in 2015 were similar throughout the year, regardless of sex and SEP. Due to the unstable numbers of monthly childhood deaths (ranging from 42 to 85 in 2014–2016), a large variation in children was noted, from 54.4% in February to 133.3% in August, while the corresponding values during the months of the MERS epidemic were 114.6% (June) and 78.0% (July) (Supplementary Table 2, Supplementary Fig. 4, only online).
DISCUSSION
This study evaluated changes in the utilization of emergency care throughout the 2015 MERS epidemic in Korea by using NHID, which covered the entire Korean population. Emergency care utilization decreased regardless of age, sex, and SEP at the peak of the MERS epidemic, especially in pediatric patients. The reduction was more prominent in low-acuity diseases than in high-acuity diseases, and in the MERS epidemic areas than in other areas. Although ER visits decreased markedly during the epidemic period, the number of deaths within 7 days of an ER visit did not change.
Patterns of medical service use in infectious disease outbreak may vary according to the characteristics of an infection, such as infectivity and lethality of the disease. Both SARS and H1N1 influenza were epidemics that caused global panic, but the pattern of healthcare utilization changed in the opposite direction. Healthcare utilization decreased in the 2003 SARS epidemic due to fear of nosocomial infection, whereas it explosively increased in the 2009 H1N1 influenza pandemic due to fear of influenza itself.23410 In the case of MERS, since the main transmission route was nosocomial transmission and the mortality rate was high, healthcare utilization decreased during the epidemic.1213 This effect was dramatic in the ER rather than other departments in hospitals, as most of the nosocomial infections occurred in a crowded ER.6 When we analyzed the monthly number of ER visits by type of ER using the National Emergency Department Information System (NEDIS) data, the number of ER visits decreased in all three types of ER (regional emergency medical center, local emergency medical center, and local emergency medical institution) in MERS epidemic, regardless of the type of ER.16 Since only 186 patients were diagnosed with MERS during the epidemic in Korea, the explanation for the impact of MERS on ER use was fear, not the MERS disease itself. The effects of fear impacted everyone in the society regardless of age, sex, and SEP groups.7 The greater reduction in the epidemic areas than in other comparison areas also corroborates the explanation that the fear of MERS infection caused the reduced utilization of healthcare.
As in previous studies examining changes in healthcare utilization according to disease severity, the results of this study showed that the reduction in emergency care utilization was most prominent for low-acuity diseases.11213 The reduction in visits for high-acuity diseases was relatively small, and the most severe diseases did not show a decrease even in June 2015, when the epidemic was at its peak. Patients decide to use medical care based on their consideration of risks and benefits. During an infectious disease epidemic, patients use medical care when they feel that the benefits of healthcare utilization are greater than the risk of infection.1 When there were concerns about nosocomial infections, those with low-acuity diseases, which are considered to have little benefits from emergency service use, were less likely to visit the ER. In Korea, due to the absence of limitations on healthcare utilization and the weak gatekeeping role of healthcare delivery system, unnecessary hospital utilization of low-acuity patients is prevalent.2829 As a result, overcrowding in a tertiary-care hospital ER caused the MERS epidemic, and low-acuity patients decreased most when the risk of infection overwhelmed the benefit of emergency service use. A study of the SARS epidemic showed that restriction of non-urgent hospital utilization during the epidemic did not increase mortality and complication rates.30 The authors of that study concluded that restriction of non-urgent visits is a safe public health strategy to control nosocomial infections and to maintain hospital surge capacity. Examining the scale of ER visits for low-acuity diseases with little benefit from service use is important, not only for preparing appropriate emergency surge capacity but also for providing evidence to redesign emergency service to decrease healthcarerelated infectious disease outbreak.
Another noteworthy finding of this study was that, although the total number of ER visits decreased, the number of deaths within 7 days of an ER visit did not meaningfully change during the epidemic. This implies that the number of patients with serious conditions visiting the ER did not change, even though overall emergency care utilization decreased. As shown for cardiac arrest and hemorrhagic stroke in this study, the reduction in ER use for high-acuity diseases is expected to be minimal in infectious disease outbreak. When fear of an epidemic spreads and ER visits decrease, preparations for serious conditions need to be focused, and patients with severe diseases should not face barriers to emergency care use.
This study had some limitations. First, our analysis was based on the assumption that no meaningful changes in factors affecting ER visits, except for the MERS epidemic, occurred during the study period, which might not have been completely true. For example, the ratio of ER visits in December 2015 was relatively low compared to the ratio in other comparison months (87.3%; Supplementary Table 1, only online). This may have been due to the influenza epidemic in December 2016, which occurred a month earlier than usual (influenza epidemic alarm was announced by the Korea Centers for Disease Control and Prevention on January 2, 2014; January 22, 2015; January 14, 2016; and December 8, 2016). However, our analysis on the utilization by region (MERS risk area versus comparison area) corroborated our explanation. Second, the scope of this study only included patients who visited the ER. The health outcomes of those who did not use emergency services were not investigated. Although ER visits for the most severe conditions did not decrease, the reduction in emergency care utilization for MI and ischemic stroke, where acute care is important, might have led to complications other than short-term mortality.3132
Supplementary Fig. 5 (only online) employing mortality data among the entire Korean population from Statistics Korea shows no apparent changes in overall mortality according to the MERS epidemic. However, further study is needed to investigate the long-term outcomes of reduced emergency care utilization. Third, ER visits due to traffic accidents, which account for a considerable proportion of injured patients, were not included in this study, as these cases were covered by auto insurance in Korea and not by the NHI. However, based on the estimates from NEDIS database in Korea, 5.1% of ER visits were covered by auto insurance.33 Changes in the ER visits covered by auto insurance would not critically change the findings.
This study also had several strengths. First, to the best of our knowledge, this is the first study to investigate the impact of MERS outbreak at the national level. In the era of emerging infectious diseases, understanding the impact of epidemic is an important first step to being prepared. Second, this study was a natural experiment, in which major confounding factors, such as social and economic factors, might well be independent of the MERS epidemic in the causal association with ER visits and mortality. Third, we employed total NHI data covering the entire Korean population, which enabled us to present stable overall- and subgroup-specific numbers of ER visits and mortality.
In conclusion, during the 2015 MERS epidemic in Korea, the utilization of emergency care decreased regardless of age, sex, and SEP. A greater reduction was observed in epidemic areas than in other comparison areas, and the reduction was greater for low-acuity diseases than for high-acuity diseases. Although the number of ER visits decreased, the number of deaths within 7 days of an ER visit did not change.
 XML Download
XML Download