

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of diabetes and obesity are consistently increasing among Koreans.1 As socioeconomic conditions and health-related dietary habits change, the prevalence of chronic degenerative diseases is increasing.2 Among chronic diseases, metabolic syndrome (MS), which is largely caused by poor dietary and lifestyle habits, is an important national and international concern that threatens public health, increases the prevalence of diabetes and cardiovascular disease, and affects quality of life.3 Although the exact pathogenic mechanism of MS remains unclear, abdominal obesity and insulin resistance are known to play major roles.4 According to data from the Korean Health Insurance Review & Assessment Service in 2014, the proportion of patients with MS in Korea was higher in individuals in their fourth (4–5%), fifth (15.6%), and sixth (36.6%) decades of life.5
MS has been reported to have a significant effect on oral health.6 Individuals with MS have poorer periodontal status than those without MS,7 and those with diabetes exhibit a higher incidence of periodontal disease.8 Moreover, hypertension plays a role in alveolar bone destruction, and smoking and alcohol use are also associated with periodontal disease.9 Progression of atherosclerotic vascular degeneration in the presence of cardiovascular risk factors may lead to decreased blood supply to the periodontal tissue, decreased resistance to anaerobic bacteria, and increased risk for periodontal disease.10 Periodontal tissue may serve as a reservoir for bacteria and their products, inflammation and immune mediators, which in turn may become a risk factor for diabetes and/or cardiovascular disease.11
Periodontal disease is one of the most frequent chronic conditions of the oral cavity and is one representative oral disease that causes tooth loss.12 According to the Korea National Health and Nutrition Examination Survey (KNHANES), in 2015, the number of residual teeth in Korean adults was 28.4 in individuals in their fourth, 27.5 in the fifth, 25.3 in the sixth, and 22.5 in the seventh decades of life, with the number of remaining teeth decreasing with older age.13
In general, the prevalence of MS and tooth loss increases with age. As the older adult population is increasing globally and since their concerns with health are increasing, the importance of oral health, as well as general health, should not be ignored. Although there have been studies investigating the relationship between MS and the number of residual teeth in Korea, the most recent used data from the 2012 Korean National Health and Nutrition Survey. Few have investigated the relationship between MS and the number of remaining teeth since 2012, including the Korean National Health and Nutrition Survey data.141516 Therefore, this study was conducted as part of a Cardiovascular and Metabolic Disease Etiology Research Center (CMERC)17 cohort study to investigate the relationship between MS, individual elements of MS, and tooth loss in middleaged Korean adults.
MATERIALS AND METHODS
This study received approval from the Institutional Review Board (4-2013-0661) of Severance Hospital of Yonsei University College of Medicine (Seoul, Korea) and from the Institutional Review Board of the Kyungpook National University Hospital (Daegu, Korea) (KNUH 2014-07-040).
Study participants
This study was conducted in collaboration with the CMERC,17 a cohort study funded by the Ministry of Health and Welfare of the Korean Government in 2013 to examine the relationship between cardiovascular and metabolic diseases and oral health. This study included individuals aged 30–64 years who resided in Seoul, Korea. From January to June 2014, individuals who were interested in participating in the oral health survey among those who visited the research clinic and provided written consent were selected. Individuals who were diagnosed with malignant tumor(s) within 2 years or were still undergoing cancer treatment; were diagnosed with myocardial infarction, stroke, or cardiac failure; were currently involved in drug trials; or who were pregnant or planning to become pregnant were excluded from consideration. Among the 748 subjects who responded to the oral health questionnaires, 30 were excluded due to unclear responses, leaving 718 in the final analysis.
Variables
MS was classified into three or more abnormalities according to the results of measurement of waist circumference, low high-density lipoprotein cholesterol, fasting blood sugar, triglyceride, and blood pressure according to the most widely used standard in the United States (National Cholesterol Education Program-Adult Treatment Panel); abdominal obesity (waist circumference, male ≥90 cm, female ≥85 cm), low high-density lipoprotein cholesterol (male ≤40 mg/dL, female ≤50 mg/dL); triglyceride [≥150 mg/dL (1.7 mmol/L)]; fasting glucose [≥100 mg/dL (6.1 mmol/L)]; and diastolic/systolic blood pressure (≥130/85 mm Hg).18 The waist circumference of the subjects was measured using a tape measure (SECA 201, Seca, Hamburg, Germany) while breathing out, after confirming the mid-point between the lower end of the last rib and the upper end of the iliac crest from the middle of the axilla. Blood samples were collected from subjects in a fasted state and submitted to a single laboratory (Seoul Clinical Laboratories, Yongin, Korea). Low high-density lipoprotein cholesterol and triglyceride levels were measured using an auto-analyzer (ADIVA1800, Siemens Medical, Deerfield, IL, USA). Glucose was measured using a colorimetric method, and low high-density lipoprotein cholesterol and triglyceride levels were measured using an enzymatic method. Blood pressure was measured three times at 2 min intervals on the right arm (HEM-7080, Omron Health, Kyoto, Japan) so as to maintain a stable state in a sitting position for 5 min before measurement. Also, we investigated for the presence of chronic diseases, such as kidney disease, chronic obstructive pulmonary disease (COPD), or rheumatic disease. Measures and methods for variables, except for the oral variables, are explained in the preceding article.17
Oral questionnaires were based on data with proven validity and reliability by Jin, et al.19 In an oral health survey, the number of teeth lost was determined by the response to the questionnaire item, “How many missing teeth do you have except the wisdom teeth?”20 The subjects were divided into two groups: those with tooth loss and those without tooth loss.
Statistical analysis
The chi-squared test was performed to examine differences in general characteristics and between subjects with and without tooth loss. Logistic regression analysis was performed to investigate the relationship between MS components and tooth loss. Subjects were divided into two groups (30–49 and 50–64 years of age) to investigate the relationship between individual components of MS and tooth loss using logistic regression analysis.2122 Multiple regression analysis was performed by subdividing individuals into two groups (30–49 and 50–64 years of age) in the groups of individuals with MS components and those without MS components. Data were analyzed using SPSS version 23.0 (IBM Corporation, Armonk, NY, USA); p<0.05 was considered to be statistically significant.
RESULTS
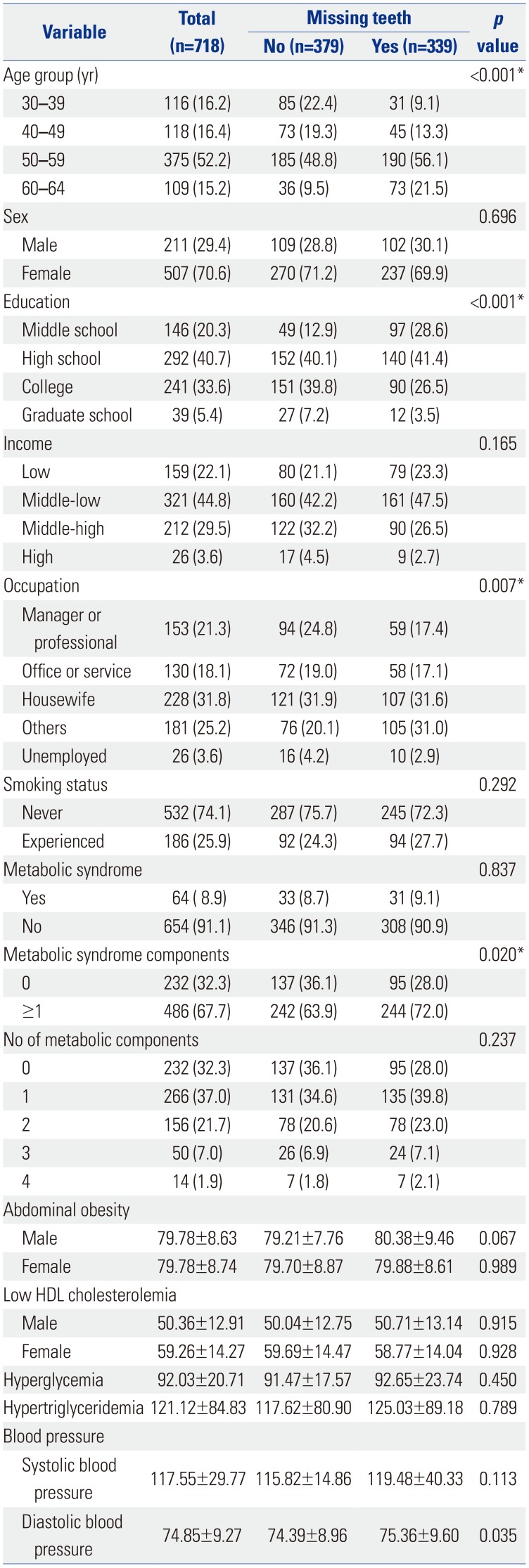
Among 718 subjects, 158 (41.7%) were 30–49 years of age and 221 (58.3%) were 50–64 years of age in the group without tooth loss. In the group with tooth loss, 76 (22.4%) participants were 30–49 and 263 (77.6%) were 50–64 years of age. In the group without missing teeth, 137 (36.1%) exhibited no MS components and 242 (63.9%) had ≥one component of MS. In the group with tooth loss, 95 (28.0%) had MS components and 244 (72.0%) had MS components, a difference that was a statistically significant (p<0.05) (Table 1).
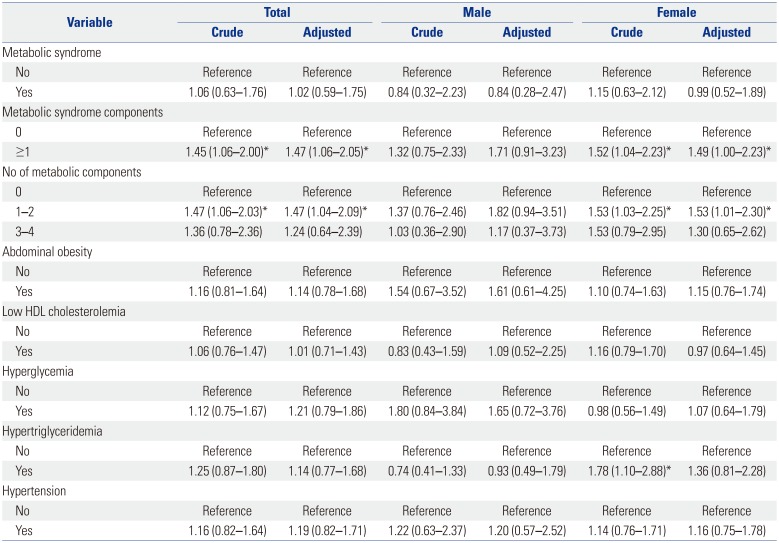
The crude odds ratio (OR) of ≥one MS component affecting tooth loss was 1.45 [95% confidence interval (CI), 1.06–2.00]. After adjusting for sex, age, education, income level, occupation, smoking status, kidney disease [2 (0.3%)], COPD [10 (1.4%)], and rheumatic disease [3 (0.4%)], the adjusted OR was 1.47 (95% CI, 1.06–2.05), which was statistically significant. The OR of the presence of one-two MS components affecting tooth loss was 1.47 (95% CI, 1.06–2.03). After adjusting for sex, age, education, income level, occupation, smoking status, kidney disease, COPD, and rheumatic disease, the adjusted OR was 1.47 (95% CI, 1.04–2.09), which was statistically significant. However, the OR of the presence of three-four MS components affecting tooth loss was not statistically significant (p>0.05). Among females, the OR of MS components (≥1) affecting tooth loss was 1.49 (95% CI, 1.00–2.23), after adjusting for sex, age, education, income level, occupation, smoking status, kidney disease, COPD, and rheumatic disease. There was a slight trend for the relationship between hypertriglyceridemia and tooth loss (Table 2).
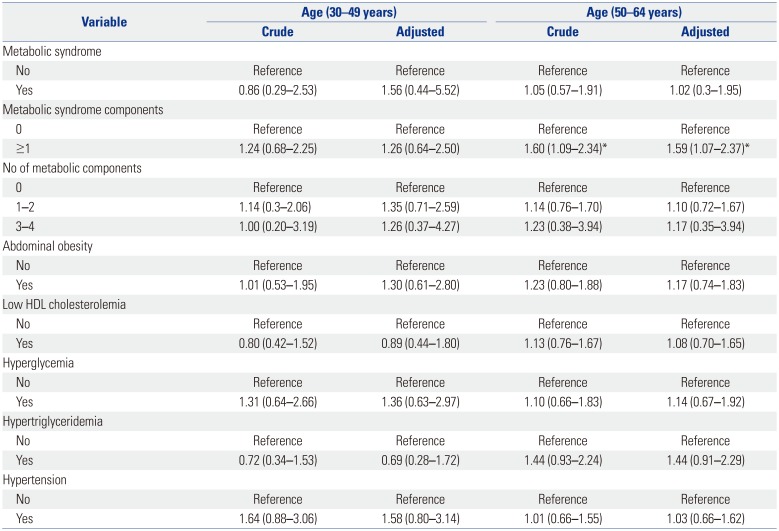
Data reflecting the relationship between MS and number of missing teeth according to age are summarized in Table 3. In the older age group (50–64 years), the OR of MS components (≥1) affecting tooth loss was 1.59 (95% CI, 1.07–2.37) after adjusting for age, sex, education, income level, occupation, smoking status, kidney disease, COPD, and rheumatic disease.
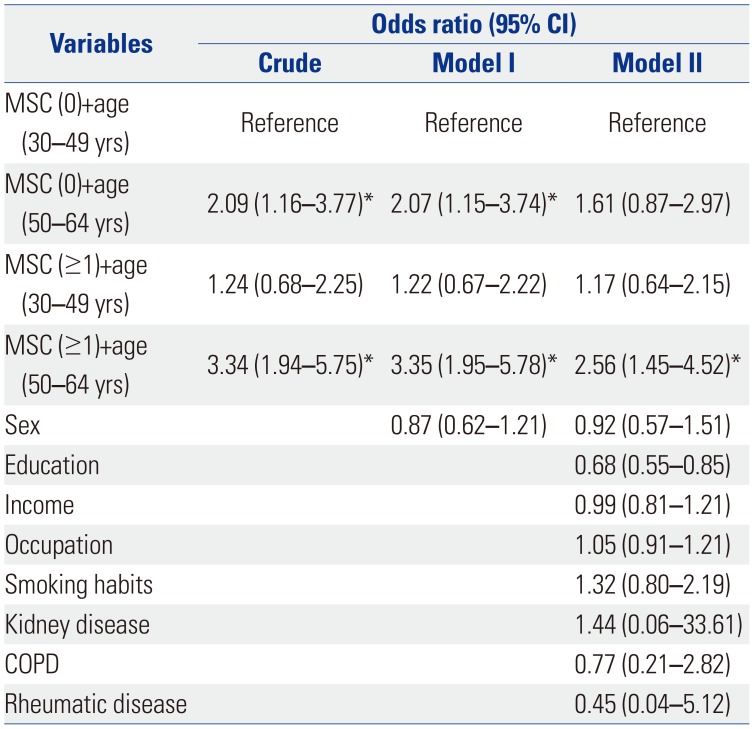
In MS components (≥1) and the older age group (50–64 years), the OR affecting tooth loss was 2.56 (95% CI, 1.45–4.52) after adjusting for sex, education, income level, occupation, smoking status, kidney disease, COPD, and rheumatic disease (Table 4).
DISCUSSION
This study investigated the risk ratio of tooth loss according to the number of MS risk factors in Korean adults. Adult tooth loss is primarily due to periodontal disease caused by alveolar bone destruction in the periosteal tissue of patients with elevated levels of various inflammatory markers.2324 It has been suggested that periodontitis elevates the levels of systemic cytokines, further enhancing lipolysis, which in turn may lead to an increase in circulating triglycerides.25 Inflammation in periodontal tissues increases inflammatory cytokine, bacterial, and lipopolysaccharide levels and shares some common risk factors with MS, including hyperglycemia, obesity, dyslipidemia, and hypertension. Periodontitis has been considered to be a risk factor for MS and can modify the disease pathway.26 Nishimura, et al.27 suggested that periodontal disease should be regarded as a component of MS; however, a causal relationship remains unclear.
Morita, et al.28 reported that the risk for periodontitis increases as the number of risk factors for MS increases. In a preliminary study conducted before this study, the risk ratio for the presence of periodontitis was 2.03 times higher in patients with MS. In addition, adults 30–49 years of age exhibited associations between MS and periodontitis; however, adults ≥60 years of age exhibited a rather weak relationship between MS and periodontitis.20 This may be explained by the fact that the risk for periodontal disease is reduced because the number of remaining teeth is small due to already extracted or missing teeth. By examining periodontal disease history and the number of remaining teeth, Joshipura, et al.29 reported that tooth loss may increase the risk for coronary artery disease.
Song, et al.14 reported a significant difference in the association between MS and the number of natural teeth. Kang and Yul30 reported that the risk ratio of tooth loss was 1.47 times higher in individuals with MS. Kim, et al.15 investigated the relationship between tooth loss and MS using KNHANES data (2012). In female especially, the number of remaining teeth was lower in those with MS, and the risk ratio of MS was 1.87 times higher when the number of remaining teeth was small. Kim, et al.15 and this study both examined the relationship between MS and tooth loss as cross-sectional studies. Kim, et al.15 demonstrated how residual teeth can affect MS in their hypothesis. Kaye, et al.31 reported that the risk ratio of missing teeth was 1.39, the depth of the periodontal pocket was 1.37, the clinical attachment loss was 1.19, the alveolar bone loss ≥40% was 1.25, and tooth mobility was 1.43 times higher in participants with MS. Therefore, this study sought to determine whether the risk of MS itself poses an impact on tooth survival considering a bi-directional biological relationship, and we would like to emphasize the importance of oral health care for MS patients or higher risk MS persons.
Furuta, et al.32 examined middle-aged Japanese adults 35 to 60 years of age and reported the association between MS and periodontal disease. The number of teeth lost was significantly associated with ≥three MS components (p<0.05). In the present study, the risk ratio for tooth loss was 1.47 times higher than that for ≥one MS components, and the difference was statistically significant (p>0.05).
Zhu and Hollis33 found that the risk ratio of MS was higher if the number of remaining teeth remained smaller. The risk ratio of MS was 1.79 times higher in edentulous patients. Ojima, et al.34 reported that the risk of MS was 1.66 times higher when the number of missing teeth was more due to dental caries, with a statistically significant difference (p<0.05). As a result, the presence of MS may increase number of missing teeth due to chronic oral diseases, such as periodontitis and dental caries. Therefore, we should always consider the impact of increasing age.
Although we cannot explain the biological mechanism of MS and tooth loss in this study, metabolic status and/or blood circulation system may play an important role in the health of the periodontium.35 Tooth loss in adults is caused by periodontal diseases defined by destruction of periodontium. In this study, we could expect that persons at higher risk of MS tend to lose teeth. The results of this study might support this mechanism. Therefore, we would like to recommend that patients with MS should receive intensive regular periodontal management at dental clinics.
This study had limitations, the first of which was its cross-sectional study, which may have introduced bias in patient selection. Second, a dentist did not conduct a direct oral examination to determine the cause of tooth loss; we only used information obtained from oral health questionnaires. Third, patients with cancer or cardiovascular disease were excluded from the study, although those who had chronic diseases, such as renal diseases or rheumatic diseases, were considered. Also, this study was limited because of a relatively low frequency of MS, compared with the Korean National Health and Nutrition Survey data. This study can be meaningful because it included a relatively large number of subjects, although not with a sample size as large as national surveys conducted by trained specialists at large hospitals in Korea. The risk of tooth loss was higher in the group 50–64 years of age with MS than the group 30–49 years of age. As the difference in age was relatively large and since residual confounding can occur, we adjusted once again for age. The OR was 1.59 (95% CI, 1.07–2.37) in the group of individuals 50–64 years of age. Similarly, there was a significant difference.
In conclusion, this study suggests that the presence of at least one MS component is associated with the prevalence of tooth loss in female and that its age-combined effect with an age between 50–64 years could have a stronger relationship. Prevention against MS for female of older age could help prevent teeth loss. Further well-designed studies are needed.
 XML Download
XML Download