

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although there are different tests for colorectal cancer (CRC) screening, colonoscopy is the most effective method for ruling out precancerous colonic lesions and for preventing cancer by allowing removal of adenomatous lesions during endoscopic examinations.123 Furthermore, colonoscopy is the standard method for examining most diseases of the colon.45 Despite the necessity of colonoscopy, patients are often reluctant to receive colonoscopy because of the inconvenience of bowel preparation and discomfort during colonoscopy.
Adequate bowel preparation is an important factor in determining the diagnostic yield, difficulty, procedure time, and completeness of colonoscopy.6 Prior abdominal or pelvic surgery is related to difficult colonoscopy, which may prolong the procedure, necessitate the need for more sedation and analgesia for the patient, and increase the risks of complications.789 Accordingly, adequate bowel preparation in patients with a prior abdominal or pelvic surgery is very important.
To date, only four studies have evaluated whether prior abdominal or pelvic surgery affects bowel preparation quality for colonoscopy.10111213 A recent prospective study from Korea suggests that a history of colorectal resection, appendectomy, and hysterectomy is associated with poor bowel preparation.13 Among abdomino-pelvic (AP) surgeries, colectomy comes out consistently as a poor prognostic factor for bowel preparation. However, a history of other AP surgeries has shown different results among studies.10111213 In addition, it is still unclear what kind of surgical procedures affects bowel preparation quality for colonoscopy, owing to the ambiguity of the descriptions in each study regarding the types of abdomino-pelvic surgery, including its range. Furthermore, the number of enrolled subjects was as small as 184–362 in prospective studies and 2811 in a retrospective study.
Therefore, in this study, we examined the relationship of patient factors (e.g., type of prior AP surgery) with bowel preparation quality in a large-scale retrospective cohort.
MATERIALS AND METHODS
Study population
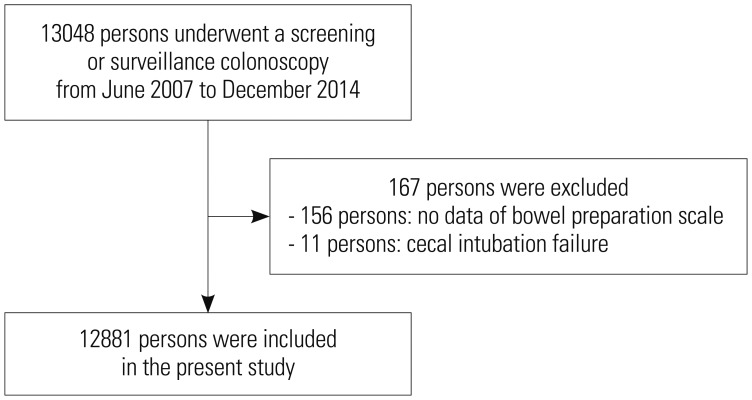
The protocols of the research were approved by the Institutional Review Board of National Cancer Center (NCC2015-0281). This study was a retrospective cohort study using a large self-motivated health screening cohort from the National Cancer Center, Korea.14 Participants underwent colonoscopies for screening or surveillance after polypectomy without symptoms. The flow of inclusion and exclusion of the study population is described in Fig. 1. We included 13048 participants who underwent screening or surveillance colonoscopy and completed questionnaires from June 2007 to December 2014. We excluded 167 participants who had no data on bowel preparation (n=156) and experienced failed cecal intubation (n=11). Therefore, 12881 participants were included in the present study. Personal data were collected by reviewing patient medical records that contained information on age, sex, medical history, smoking status, drinking status, and colonoscopy findings with pathologic results.
Colon cleansing methods
All patients were educated to follow a low-fiber diet for 3 days before the test and a liquid diet at dinner on the day before, while fasting over midnight. The medications used in this study were Fleet Phospho-soda (NaP), 4-L polyethylene glycol (4L-PEG), Coolprep (2-L PEG+Ascorbic acid, 2L-PEG+Asc), Picolight (Sodium picosulfate-magnesium citrate, SPMC).
In the NaP group, the participants ingested 45 mL of aqueous Fleet Phospho-soda (Fleet Company, Inc., Lynchburg, VA, USA) in 240 mL of water, followed by 1500 mL of water at 7 pm the day before colonoscopy. They ingested another 45 mL of aqueous Fleet Phospho-soda (NaP) in 240 mL of water, followed by 1500 mL of water at 10 pm. In the 4-L PEG group, the patients ingested 4 L of PEG (Taejoon Pharmaceuticals, Seoul, Korea; 236 g PEG, 22.74 g Na2SO4, 6.74 g NaHCO3, 5.86 g NaCl, and 2.97 g KCl), starting at 6 am on the day of colonoscopy. All patients were asked to drink PEG at a rate of 200 mL/10 min. In the SPMC group, the participants ingested Picolight (Pharmbio Korea, Seoul, Korea), which consists of 10 mg of sodium picosulfate hydrate, 3.5 g of magnesium oxide, and 12 g of citric acid, and water the day before colonoscopy at 7 pm, followed by 2000 mL of water at 10 pm. In the 2L-PEG+Asc group, the participants ingested Coolprep (Taejoon Pharmaceuticals), which consists of 2 L of PEG-based laxative with ascorbic acid (100 g PEG 3350, 1.015 g potassium chloride, 5.9 g sodium ascorbate, 2.691 g sodium chloride, 7.5 g sodium sulfate anhydrous, and 4.7 g ascorbic acid), and water the day before colonoscopy at 7 pm, followed by 1000 mL of water at 10 pm. All bowel preparation methods included 10 mg bisacodyl tablets that were to be ingested the day before colonoscopy.
Colonoscopy procedure
We performed colonoscopy using a colonoscope (Q260AL, Olympus Optical Co., Ltd., Tokyo, Japan), recording the location and size of all polypoid and sessile lesions. All polyps or cancers removed endoscopically or surgically were fixed in formaldehyde and sent to the pathologic laboratory for routine histologic examination. The histological evaluation was conducted in accordance with the World Health Organization criteria. All of the endoscopic examinations were performed by experienced endoscopists.
Measurements of bowel preparation quality
Bowel preparation quality was assessed by the performing endoscopist using the Aronchick scale [excellent (small volume of clear liquid or >95% of the surface seen), good (large volume of clear liquid covering 5–25% of the surface, but >90% of the surface seen), fair (some semisolid stool that could be suctioned or washed away but >90% of the surface seen), poor (semisolid stool that could not be suctioned or washed away and <90% of the surface seen), and inadequate (repeat preparation needed)].15 In this study, bowel preparation quality was categorized as satisfactory for excellent to good bowel preparation or unsatisfactory for fair to inadequate bowel preparation.
Statistical analysis
Continuous variables are expressed as means±standard deviations and categorical variables as numbers (%). In univariate analyses, the satisfactory bowel preparation group and unsatisfactory bowel preparation groups were compared using Student's t-test for continuous variables and the chi-square test or Fisher's exact test for categorical variables. In multivariate analysis, binomial logistic regression analysis was used to analyze factors associated with unsatisfactory bowel preparation. Results were considered to be statistically significant if the p value was <0.05. All statistical analyses were performed using SPSS version 14.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics of the included participants
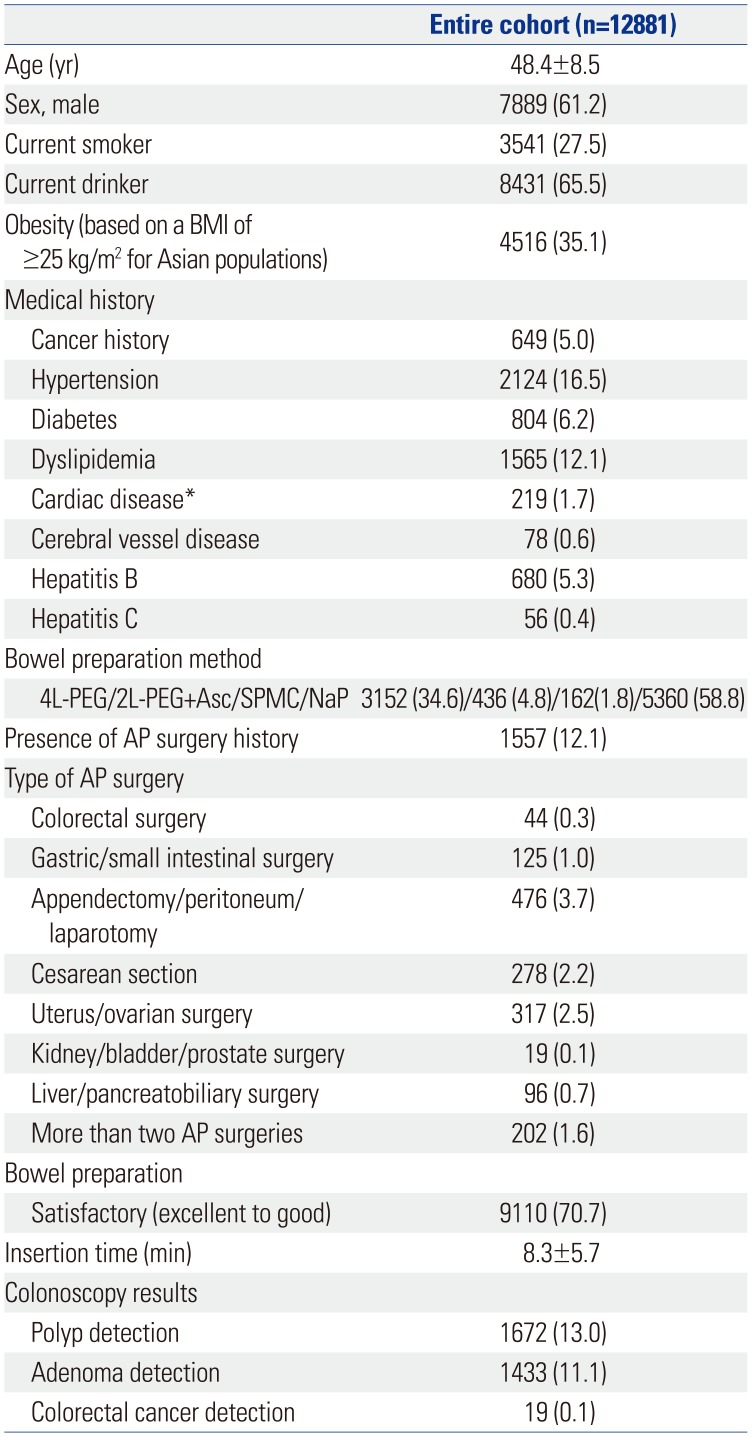
The baseline characteristics of the 12881 participants are described in Table 1. Their mean age was 48.4±8.5 years, and 61.2% were men. Further, 27.5% were current smokers, and 35.1% had obesity [body mass index (BMI) of ≥25 kg/m2 for Asian populations]. Eight hundred and four (6.2%) participants had diabetes, and 649 (5.0%) had a history of cancer. Bowel preparation was performed using NaP, 4L-PEG, 2L-PEG+Asc, and SPMC in 58.8, 34.6, 4.8, and 1.8% of the patients, respectively.
A total of 1557 (12.1%) participants had a history of AP surgery. The type of AP surgery was colorectal surgery (44 participants), gastric/small intestinal surgery (125 participants), appendectomy/peritoneum/laparotomy (476 participants), cesarean section (278 participants), uterus/ovarian surgery (317 participants), kidney/bladder/prostate surgery (19 participants), and liver/pancreatobiliary surgery (96 participants). In addition, 202 participants underwent more than two AP surgeries (Table 1).
Colonoscopy revealed satisfactory bowel preparation in 70.7%. The mean colonoscopy insertion time was 8.3±5.7 minutes. The adenoma detection rate was 11.1%, and the cancer detection rate was 0.1% (Table 1).
Factors associated with bowel preparation quality
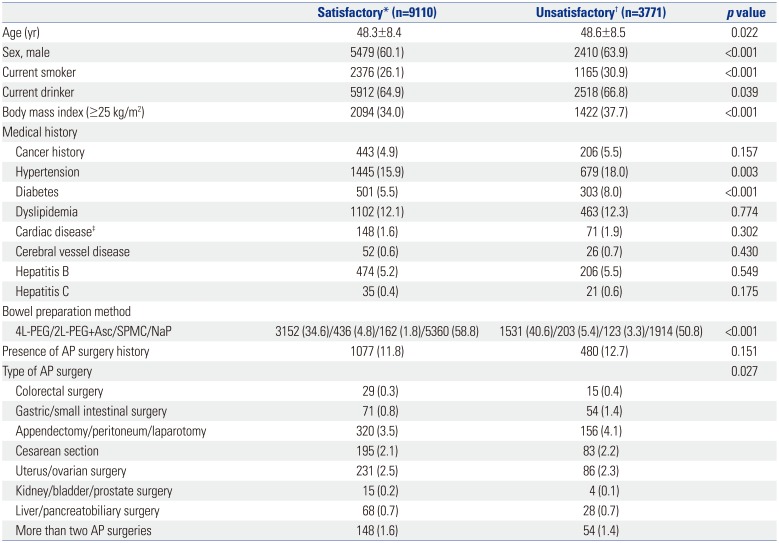
The included participants were divided into two groups based on bowel preparation quality (satisfactory and unsatisfactory). In the univariate analysis, old age (p=0.022), male sex (p<0.001), current smoking (p<0.001), current drinking (p=0.039), obesity (p<0.001), hypertension (p=0.003), diabetes (p<0.001), bowel preparation method (p<0.001), and type of AP surgery (p=0.027) were associated with unsatisfactory bowel preparation (Table 2).
Factors associated with unsatisfactory bowel preparation in multivariate analysis
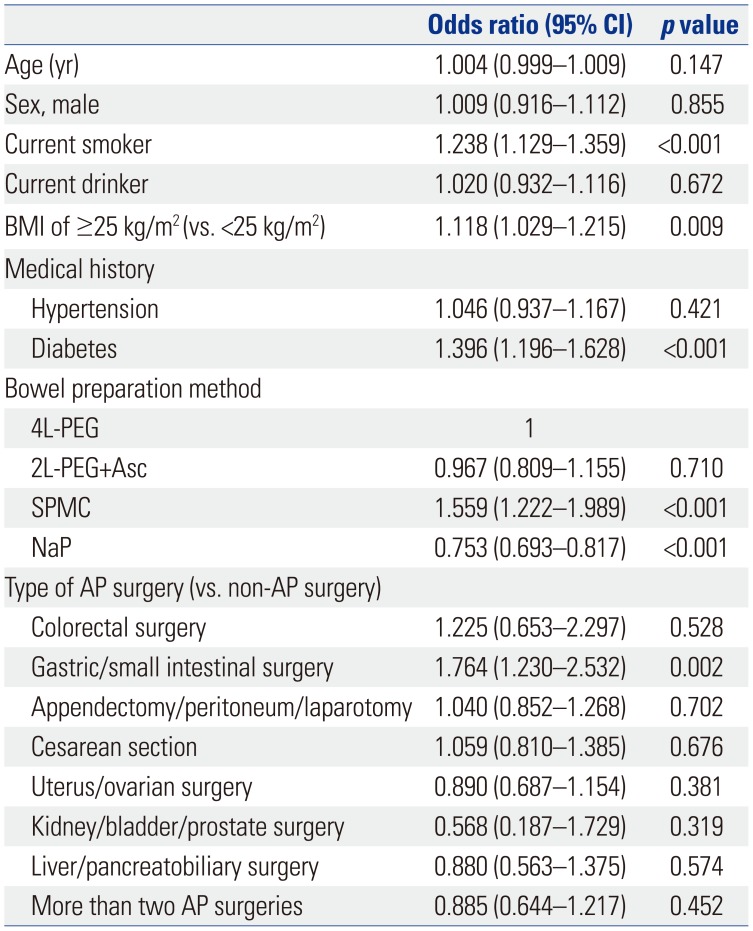
To analyze the factors associated with unsatisfactory bowel preparation, a multivariate analysis adjusted for age, sex, current smoking status, current drinking status, BMI, hypertension, diabetes, bowel preparation method, and type of AP surgery was performed. Unsatisfactory bowel preparation was related to current smoking [odds ratio (OR)=1.238, 95% confience interval (CI)=1.129–1.359, p<0.001], obesity (OR=1.118, 95% CI=1.029–1.215, p=0.009), diabetes (OR=1.396, 95% CI=1.196–1.628, p<0.001), SPMC administration (OR=1.559, 95% CI=1.222–1.989, p<0.001), and gastric/small intestinal surgery (OR=1.764, 95% CI=1.230–2.532, p=0.002). In contrast, NaP administration was related to satisfactory bowel preparation (OR=0.753, 95% CI=0.693–0.817, p<0.001) (Table 3).
DISCUSSION
The present study demonstrated that gastric/small intestinal surgery is a potential risk factor for poor bowel preparation. The reason for poor bowel preparation quality in patients with a history of bowel resection is unclear. However, there are some possible explanations. First, patients experience altered bowel motility after bowel resection. Second, adhesions can develop after laparotomy as a consequence of the inflammatory response to tissue injury with subsequent healing, and intraabdominal adhesion can cause fixation of the flexible intestine, which may lead to retention of fecal material regionally. Nevertheless, the suggested mechanism for poor bowel preparation in patients with a history of bowel resection is a hypothesis and needs to be proven by additional studies.16 Among the 125 participants who had a prior gastric/small intestinal surgery in this study, 123 underwent gastrectomy mainly due to gastric cancer. Importantly, the incidence of colonic neoplastic lesions in the patients with gastric cancer is higher than that in the general population.171819 Therefore, high-quality colonoscopy is mandatory for these patients.
Meanwhile, however, unlike other intestinal surgery, prior colorectal surgery did not affect bowel preparation quality in this study. In contrast, similar with other bowel resections, prior colorectal surgery was also a risk factor for poor bowel preparation in previous studies.101113 This is probably because the participants with a history of colorectal surgery in the National Cancer Center had previously undergone multiple colonoscopies because of a CRC history. Therefore, several experiences of bowel preparation and the recognition of its importance could affect a successful bowel preparation.
Obesity and diabetes are well-known risk factors for poor bowel preparation in previous studies.20 Further, it is known that the degree of bowel preparation may vary depending on the agents and methods of bowel preparation used.2122232425 Although there is insufficient evidence showing current smoking as a risk factor for poor bowel preparation, a previous study showed the same results with this study.26 The reasons why current smokers were more likely to present with a poorer preparation quality remain speculative. These individuals might have a poorer tolerability to the regimen or failed to follow the preparation schedule completely owing to the relatively lower health consciousness.
A particular strength of this study is its large-scale data compared with those of previous studies. Moreover, colonoscopies were performed by well-trained endoscopists. In addition, numerous patients with a prior abdominal surgery were included because the study was conducted at the National Cancer Center.
Despite the insights provided by the present study, it has some limitations. First, bowel preparation was not conducted using the split method. Second, NaP, which is not used currently owing to safety concerns, was included. Third, we did not use the Boston Bowel Preparation scale, which is the most thoroughly validated scale. Lastly, because of the retrospective study design, some factors that could affect bowel preparation quality, such as completeness of the preparation schedule, compliance rate of low-residual diet, or water intake, could not be investigated. Diet restriction and completeness of the purgatives are crucial factors of a satisfactory bowel preparation.27282930
In conclusion, the present study demonstrates that gastric/small intestinal surgery is a potential risk factor for poor bowel preparation. Further research on patients with a history of gastric/small intestinal surgery is mandatory to determine the appropriate methods for an adequate bowel preparation.
 XML Download
XML Download