

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lung transplantation has remained the only treatment option for chronic progressive lung disease since the first successful unilateral lung transplantation procedure in pulmonary fibrosis patients in 1983.1 However, median survival thereafter is relatively low (5.9 years), compared with other solid organ transplantation approaches. Notably, however, median survival increases to 8.1 years for patients who survive for the first year or more.23 Previous studies have revealed several factors related to mortality, which could be used to predict prognosis.456789 However, quality of life and performance differ according to the degree of recovery of pulmonary function, even if patients survive after lung transplantation.
Lung function recovery is an important predictor of prognosis in lung transplant recipients and is used as a diagnostic parameter for bronchiolitis obliterans syndrome (BOS).10 BOS is defined as a sustained decline in forced expiratory volume in 1 second (FEV1).11 While inflammation, destruction of small airway, and fibrosis are putative mechanisms of BOS, this condition is not easy to diagnose through biopsy. Therefore, lung function deterioration on pulmonary function test (PFT) has been suggested as a diagnostic criterion for BOS.11 Pulmonary function is known to be influenced by acute rejection, infection, recurrence of primary disease, and complication at the anastomosis site; therefore, early prediction of pulmonary function deterioration is an important factor for the survival of recipients.121314 While increasing the 1-year survival rate to improve long-term survival rate is important, although lung function recovery also serves as an important prognostic factor for surviving patients.4 Notwithstanding, there has been no definitive study of factors affecting lung function recovery at the first year of lung transplantation. Thus, the purpose of this study was to identify factors affecting the recovery of pulmonary function in patients who survive for >1 year after lung transplantation.
MATERIALS AND METHODS
Study design and patient population
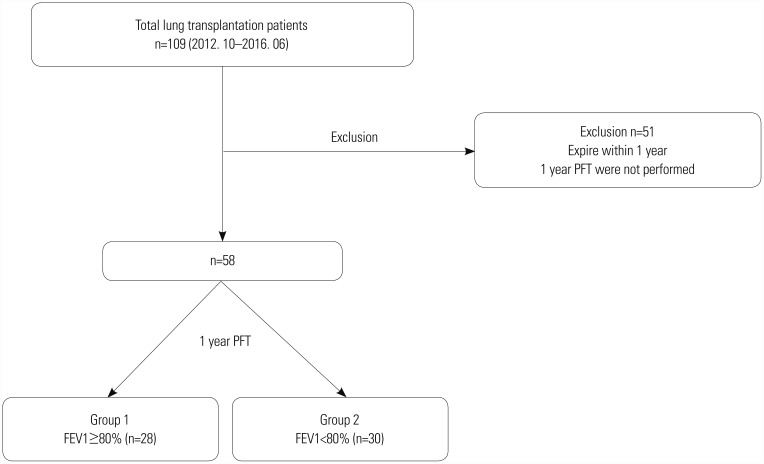
We retrospectively reviewed the electronic medical records of lung transplantation patients in a single tertiary medical institution in South Korea for the period between October 2012 and June 2016. As described in Fig. 1, 109 patients underwent lung transplantation during the study period; 58 patients were included in the study. Patients who died within one year after lung transplantation (n=47, 43.1%) or who did not complete PFTs (n=4, 3.7%) were excluded. A follow-up PFT was scheduled every 3 months after transplantation. The patients were divided into two groups according to whether they recovered to a normal range of FEV1 (FEV1 ≥80% of predicted value vs. <80%). The study protocol was approved by the Institutional Review Board (IRB) of Severance Hospital (IRB No. 4-2013-0770).
Variables and definitions
We analyzed various clinical characteristics, including recipient, perioperative, postoperative, and donor factors. The recipient factors included age, gender, body mass index (BMI), smoking history, transplant type, primary or underlying disease, and preoperative prognostic nutritional index (PNI). PNI was calculated using the following equation: [10×albumin (g/dL) + 0.005×total lymphocyte count (per mm3)].15 Perioperative and postoperative factors, such as mechanical ventilator (MV) use or extracorporeal membrane oxygenation (ECMO) use before and after transplantation, intensive care unit (ICU) duration, and hospitalization duration, were analyzed. Primary graft dysfunction (PGD) and acute rejection requiring steroid pulse therapy were also reviewed. PGD was scored based on the International Society of Heart and Lung Transplantation (ISHLT) criteria; grade 2–3 was classified as high-grade PGD.16 Factors related to the operation included operation time, ischemic time, and size mismatch between donor and recipient. Donor information, such as age, gender, BMI, smoking history, total lung capacity (TLC), size match, arterial partial pressure of oxygen (PaO2), fraction of inspired oxygen (FiO2), and ventilation time, was collected through the Korean Network for Organ Sharing.
Statistical analysis
All statistical analyses were performed using SPSS Statistics version 23 (IBM Corp., Armonk, NY, USA). Unadjusted variables of study groups were analyzed by chi-squared test or Mann-Whitney test, then described as numbers (percentages) or medians [ranges or interquartile ranges (IQRs)]. Relationships between variables and lung function recovery were assessed by logistic regression models for multivariate analysis. p values ≤0.05 were regarded as significant.
RESULTS
Characteristics of the patients
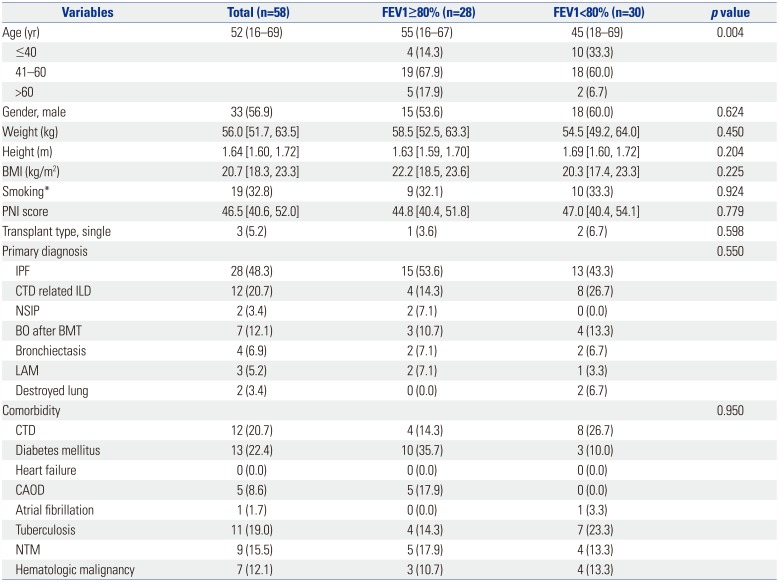
A total of 109 patients underwent lung transplantation during the study period; 58 patients who survived more than one year and who underwent PFTs at the first year after transplantation were enrolled. The patients were divided into two groups according to their FEV1 values at 1 year after lung transplantation: 28 patients (48%) were classified as FEV1 ≥80% of the predicted value group (FEV1 ≥80% group); the remaining patients (52%), whose FEV1 was less than 80%, were classified into FEV1 <80% of the predicted value group (FEV1 <80% group). Baseline characteristics and variables of recipients are presented in Table 1. Median age was significantly younger in the FEV1 <80% group (55 years vs. 45 years, p=0.004). Gender, BMI, smoking history, and PNI were not significantly different between the two groups. Most operations were bilateral lung transplantations, except one case (3.6%) in the FEV1 ≥80% group and two cases (6.7%) in the FEV1 <80% group. Idiopathic pulmonary fibrosis (IPF) was the most common cause of lung transplantation in both groups [15 patients (53.6%) in the FEV1 ≥80% group vs. 13 patients (43.3%) in the FEV1 <80% group, p=0.550]. The proportions of primary pulmonary diagnoses or comorbidities were not statistically different.
Recovery of pulmonary function after transplantation
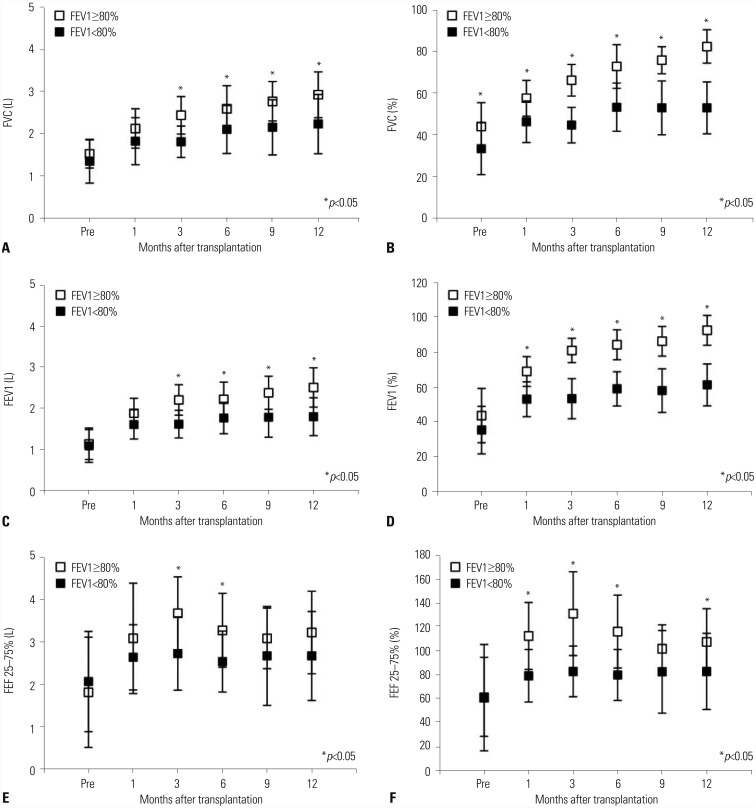
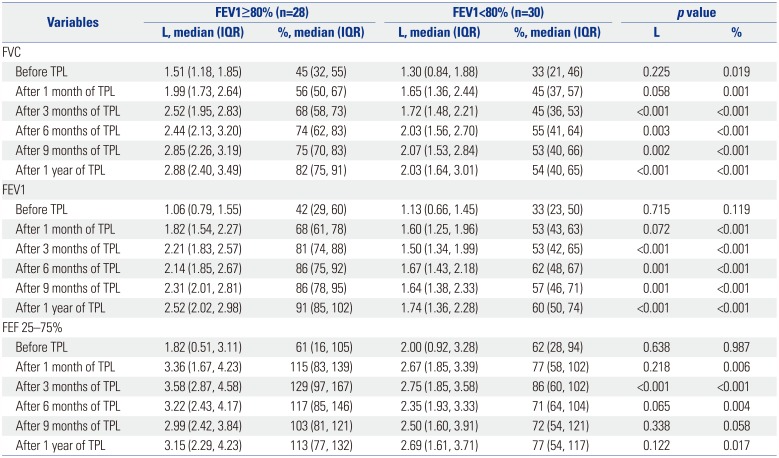
The postoperative recovery of pulmonary function was assessed by PFT. The results are presented in Table 2 and Fig. 2. In preoperative PFTs, the forced vital capacity (FVC) of the FEV1 <80% group was lower than that of the FEV1 ≥80% group (45% vs. 33%, p=0.019), while FEV1 and forced expiratory flow 25–75% (FEF 25–75%) were not significantly different before operation between the two groups. After transplantation, PFTs were performed at 1, 3, 6, 9, and 12 months after transplantation. All median values of FVC, FEV1, and FEF 25–75% showed better recovery in the FEV1 ≥80% group (FVC: 82% vs. 54%, p<0.001; FEV1: 91% vs. 60%, p<0.001; FEF 25–75%: 113% vs. 77%, p=0.017).
Perioperative factors associated with lung function recovery
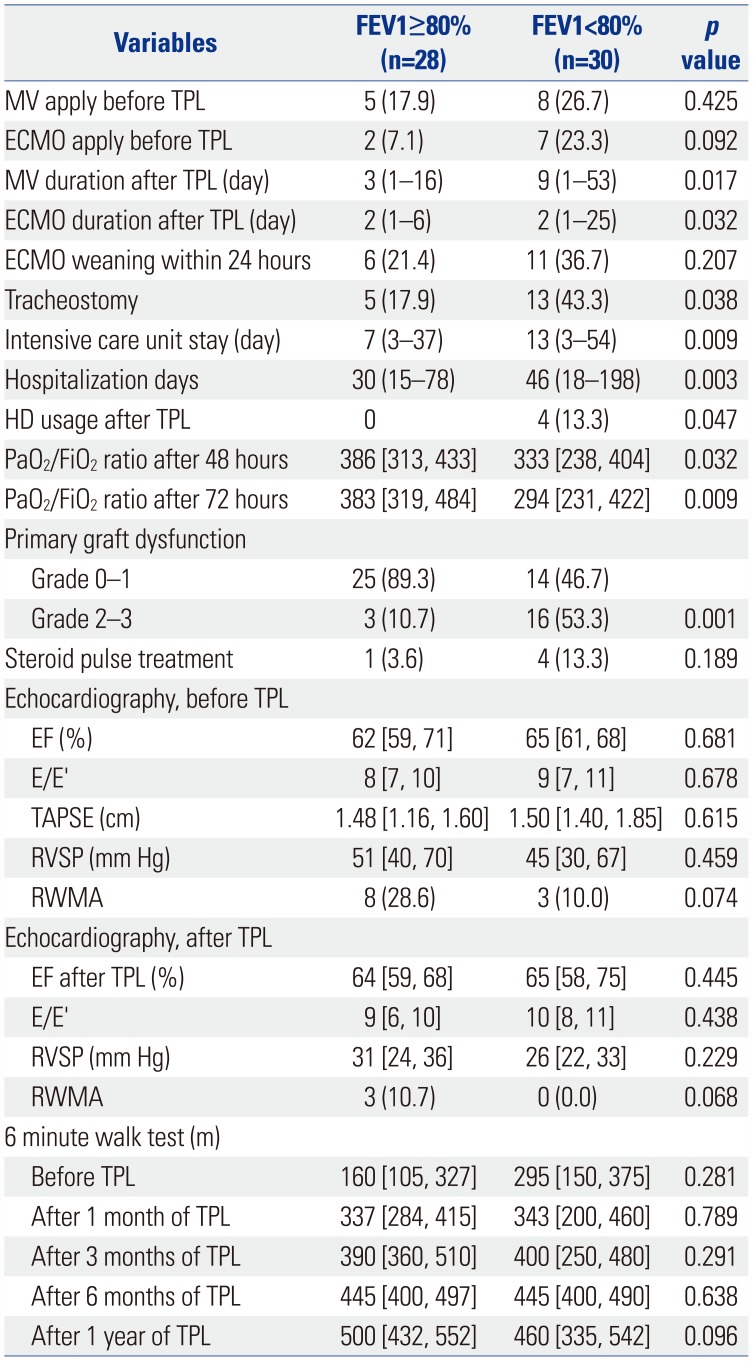
Perioperative variables associated with lung function recovery are presented in Table 3. Echocardiographic variables and 6-minute walk test (6MWT) results were not significantly different between the two groups. There was no difference in preoperative MV or preoperative ECMO use between the two groups. However, the median duration of postoperative MV and postoperative ECMO was longer in the FEV1 <80% group than in the FEV1 ≥80% group [MV duration; 3 (range, 1–16) vs. 9 (1–53) days, p=0.017; ECMO duration: 2 (range 1–6) vs. 2 (1–25) days, p=0.032]. The proportion of tracheostomies was larger in the FEV1 <80% group (17.9% vs. 43.3%, p=0.038). Furthermore, FEV1 <80% group patients were hospitalized for longer periods and received longer ICU care than patients in the FEV1 ≥80% group (hospitalization: 30 days vs. 46 days, p=0.003; ICU duration: 7 days vs. 13 days, p=0.009). During the postoperative period, four of the FEV1 <80% group patients needed renal replacement therapy, while none of the FEV1 ≥80% group required this therapy [FEV1 ≥80% vs. FEV1 <80%: 0 patients (0.0%) vs. 4 patients (13.3%), p=0.047]. At 72 hours after transplantation, compared with the FEV1 ≥80% group, patients with FEV1 <80% had more high-grade PGD [FEV1 ≥80% vs. FEV1 < 80%: 3 patients (10.7%) vs. 16 patients (53.3%), p=0.001], while graft rejection and acute rejection requiring steroid pulse treatment within 1 year were not significantly different.
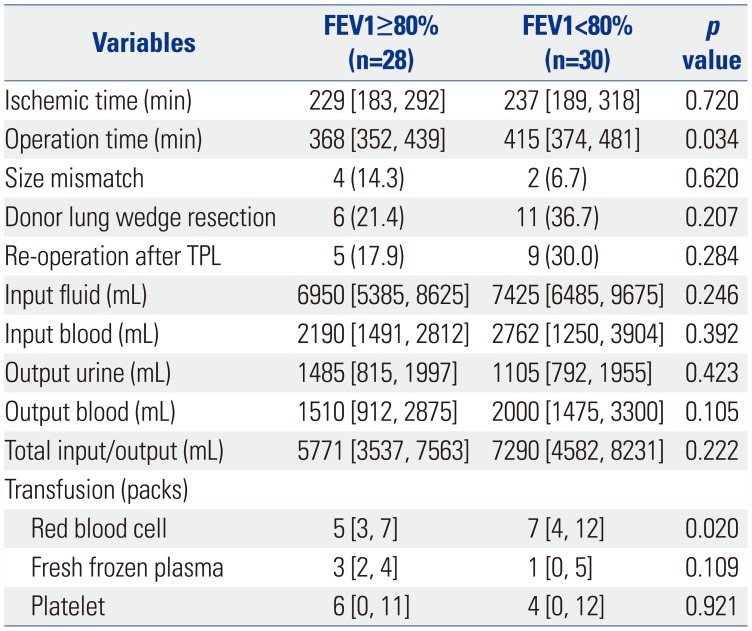
Intraoperative variables are presented in Table 4. The median time of operation was longer in the FEV1 <80% group than in the FEV1 ≥80% group (368 min vs. 415 min, p=0.034), while ischemic time, size mismatch, proportion of donor lung wedge resection, and re-operation after transplantation were not significantly different. There was no difference between the two groups in total fluid control, except for the quantity of red blood cell transfusion (FEV1 ≥80% vs. FEV1 <80%: 5 packs vs. 7 packs, p=0.020).
Characteristics of the donors
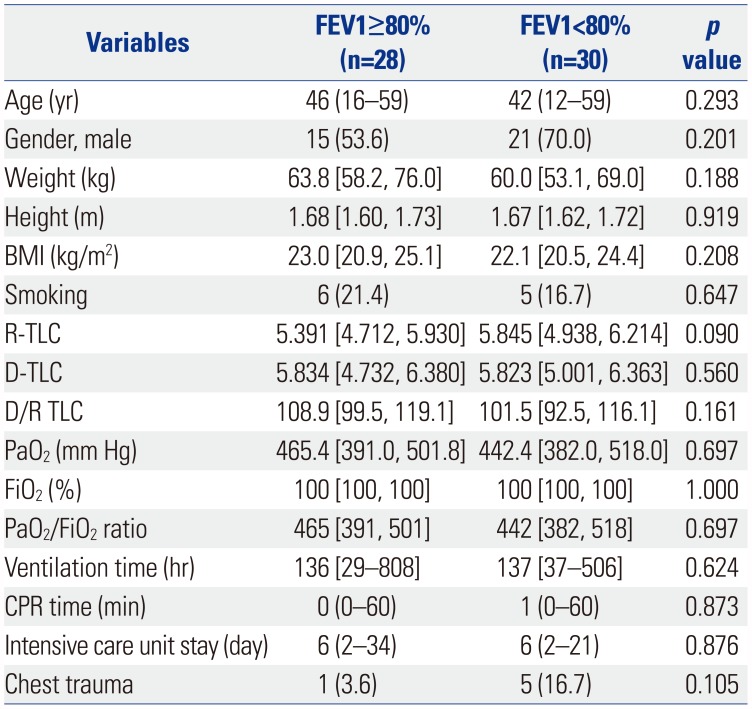
Regarding donor variables, there was no significant difference between the two groups in regards to age, gender, BMI, smoking history, D/R TLC, PaO2/FiO2 ratio, ventilation time, CPR time, duration of ICU stay, or chest trauma history. The results are shown in Table 5.
Multivariate analysis of the variables
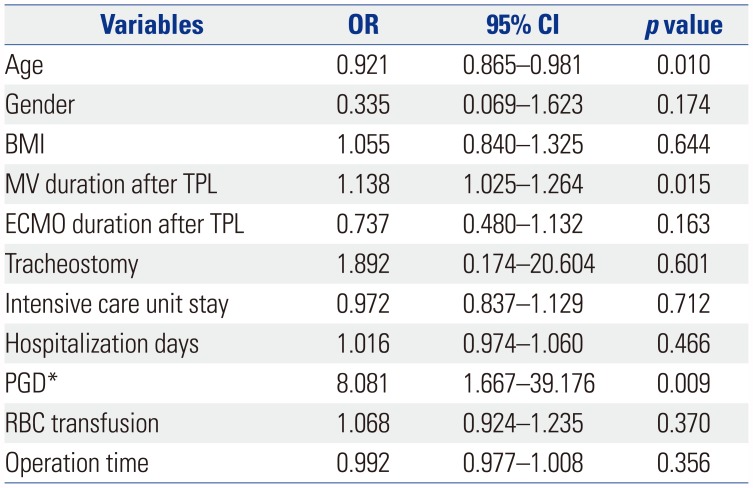
Multivariate analysis revealed that younger recipients [odds ratio (OR), 0.92; 95% confidential interval (CI), 0.87–0.98; p=0.010], longer duration of MV use after surgery (OR, 1.14; 95% CI, 1.03–1.26; p=0.015), and high-grade PGD (OR, 8.08; 95% CI, 1.67–39.18; p=0.009) were independent risk factors associated with a lack of full recovery of lung function at 1 year after lung transplantation (Table 6).
DISCUSSION
Lung transplants are increasing worldwide. According to the ISHLT registry, a total of 60107 lung transplants had been performed by June 2016, although with a median survival of 6.0 years. While the median survival of lung transplant patients improves slightly (up to 8.1 years) in those surviving more than one year after surgery, it remains lower than the survival rate of other solid organ transplants.2 Therefore, most previous studies have involved finding survival-related risk factors to improve the overall survival of lung transplant recipients.456789 Meanwhile, a comparative study of the recovery of pulmonary function in surviving patients has not been a research priory. While there are some patients whose lung function recovers well, there are some who fail to fully recover lung function. The purpose of this study was to investigate factors affecting pulmonary function recovery in patients surviving at least 1 year after lung transplantation.
In our study, younger recipients, a longer duration of MV use after surgery, and high-grade PGD were independent risk factors associated with a lack of full recovery of lung function at 1 year after lung transplantation. According to the 2017 ISHLT registry report, an older recipient age is associated with a higher rate of mortality in the first year.2 The current study applied an analysis of only surviving patients; we excluded those who expired within the first year of transplantation. Comparing the baseline characteristics of the patients excluded from and included within the study, we noted that the median age of the excluded patients was significantly higher (included patients vs. excluded patients: 52 years, range 16–69 years vs. 61 years, range 16–75 years; p<0.001). Therefore, it is difficult to interpret age as a significant risk factor for the lack of full recovery of lung function among survivors.
Comparing reasons for lung transplantation according to age, we found that IPF was the most common cause in patients over 40 years of age [age ≤40 vs. age >40: 3 patients (21.4%) vs. 25 patients (56.8%), p=0.022]. However, in individuals under 40 years of age, transplantation was most frequently performed because of bronchiolitis obliterans after bone marrow transplantation [age ≤40 vs. age >40: 5 patients (35.7%) vs. 2 patients (4.5%), p=0.002]. According to the ISHLT registry, infection is the most common cause of death within 1 year after lung transplantation.2 In patients with Graft-Versus-Host disease, mucosal barriers are also affected, and susceptibility to infections is increased, affecting lung function recovery.17
One study has described a relationship between PGD at 72 hours after transplantation and 6MWT performance.18 In our study, high-grade PGD was more common in the FEV1 <80% group. Although there was no significant difference in 6MWT after 1, 3, 6, and 12 months of transplantation in our study, we did exclude patients who did not undergo PFT, which may account for the discrepancy between the results of this and the aforementioned study. We suspect that PGD may have a negative effect on functional status after lung transplantation.
Interestingly, we noted no relationship between MV or ECMO application before transplantation and recovery of pulmonary function after transplantation. However, there was a significant difference therein during the postoperative period. In the FEV1 <80% group, the duration of MV or ECMO usage was longer and tracheostomies were performed more frequently during the postoperative period. Additionally, univariate analysis revealed significant differences in the use of renal replacement therapy, ICU stay, and total hospitalization days. These findings suggested that immediate postoperative graft function recovery is an important factor for prognosis. In multivariate predictive models of overall mortality recorded in the 2017 ISHLT registry, only allograft ischemic time was identified as an operative variable for prediction models. Although we did not analyze mortality, our results indicate that the degree of lung function recovery can influence overall survival, consistent with previous studies.29
This study has limitations in that it was performed on a small number of subjects from a single institution. Age can be considered an important factor; however, older adult patients were generally excluded from this study. Thus, we could not clarify the correlation between age and pulmonary function recovery. Among the components that were used to grade the degree of PGD, chest radiographs were difficult to interpret because they included mixed infiltration by pulmonary edema, infection, and changes due to vascular complications or postoperative changes. Further research including additional patients from multiple centers, as well as more clarified clinical factors, is needed. Nevertheless, our study has strengths. To date, many studies have been conducted to investigate mortality after transplantation. However, depending on lung function recovery, survivors may have a very different quality of life. Thus, in this study, we evaluated factors affecting pulmonary function recovery in patients who survived more than one year. This study lays the groundwork for further study.
In conclusion, postoperative MV duration and graft dysfunction at 72 hours were identified as important factors affecting lung function recovery after the first year of lung transplantation. Therefore, immediate postoperative status may be associated with recovery of lung function after lung transplantation. Clinicians should carefully follow the degree of PFT in lung transplant patients who experience postoperative complications.
 XML Download
XML Download