

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Trampoline-related injuries are steadily increasing. National health morbidity data from Australia showed an average of 1737 trampoline injuries per year, and the frequency of injuries has grown yearly.1 The National Electronic Injury Surveillance System (NEISS) in the United States reported an estimated 1002735 emergency department (ED) visits for trampoline-related injuries between 2002 and 2011; 288876 (29%) were sustained fractures.2 In addition to the growing frequency of trampoline-related injuries, trampoline use is a subject of public health interest because it poses a considerable risk of severe injuries, including fractures or cervical cord injuries leading to quadriplegia.34 The U.S. Consumer Product Safety Commission announced that there were a total of 22 trampoline-related deaths in the 10-year period between 2000 and 2009.5 One study showed that emergency room visits due to trampoline injuries accounted for 31% of fractures, and that half of them required surgery.6
Despite the known risks and recommendations, trampolines continue to be popular.7 The incidence and characteristics of trampoline injuries have been well documented in North America and Europe.18910 As a result of these reports, the American Academy of Pediatrics released a policy statement and safety recommendations regarding trampoline use.7 Unlike in North America and Europe, there is a lack of trampoline-related injury studies in Asia. To our knowledge, there have been very few reports of trampoline-related injuries in Asian children. This study aims to investigate the features of pediatric trampoline-related injuries in Korean children, using prospective nationwide injury databases.
MATERIALS AND METHODS
Study design and data source
We conducted this retrospective cohort study using the Emergency Department-based Injury In-depth Surveillance (EDIIS) database of Korea, which is organized and sponsored by the Korea Centers for Disease Control and Prevention. EDIIS is a nationwide prospective database of injured patients who visit the ED. It was developed based on the International Classification of External Causes of Injuries of the World Health Organization. EDIIS collects injury-related information to help establish national policies for the prevention of injuries.
The database gathers patients' demographic features, injury-related information, prehospital emergency medical service records, ED diagnosis, ED treatment, ED disposition, and patients' outcomes after admission (for patients who are admitted). Data are primarily collected by physicians in EDs. The recorded data are supervised and corrected by trained research coordinators and emergency physicians who are responsible for EDIIS. Research coordinators, who complete a training course before participating in the project, input the collected information into a web-based database system. A quality management committee reviews the database and provides feedback to EDIIS participants regularly.
Inclusion criteria and collected variables
We used the data for patients with trampoline injuries in the EDIIS database between 2011 and 2016. The Code C10.03.10 (for trampoline) in the “underlying object of the injury” section in the EDIIS database was used to identify trampoline injuries. Cases were also included if the narrative comments included words that meant trampoline in Korean, such as “pong-pong,” “bang-bang,” or “trampoline.” Patients between 0 and 17 years of age were included. Information was collected on the following characteristics of the patients: age, sex, mechanism of injury, location of injury, type of injury (soft tissue injury or fracture), area of injury, and treatment. In EDIIS, injury location is classified into 13 categories: home, group dwelling (e.g., nursing home), medical facility, school, gymnasium, road, other traffic area, industrial place, farm, recreational facility, commercial facility, outdoors, and unknown location. For this study, we classified injuries that occurred at recreational or commercial facilities as trampoline park injuries.211
Statistical analysis
SPSS software (ver. 22.0, IBM SPSS Statistics, IBM Corp., Armonk, NY, USA) was used for statistical analysis. Continuous variables are presented as medians and interquartile ranges because of their skewed distributions. Comparisons of continuous data were performed using the Mann-Whitney U test or the Kruskal-Wallis test. When the Kruskal-Wallis test revealed a significant difference, the Mann-Whitney U test was applied with a Bonferroni correction for five groups to identify differences between individual groups [significant difference at p<0.005 (0.05/10)]. Categorical variables are presented as frequencies and percentages, and comparisons were performed using the chi-square test or Fisher's exact test. p values less than 0.05 were considered statistically significant.
RESULTS
Baseline characteristics of the study population
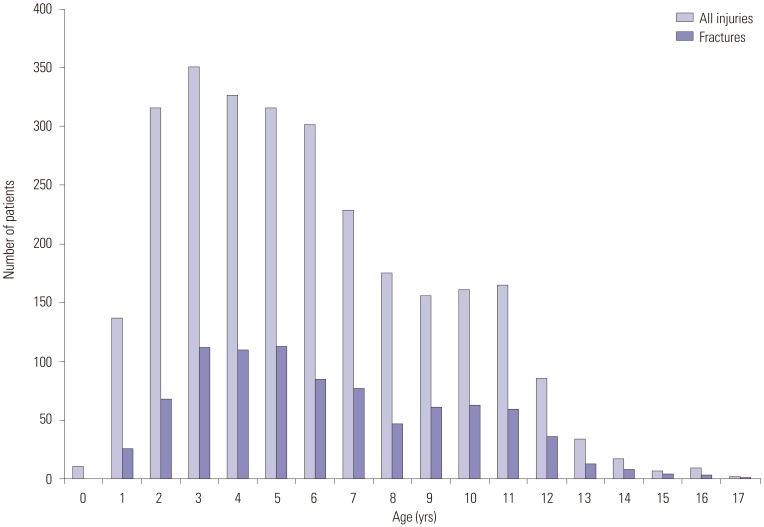
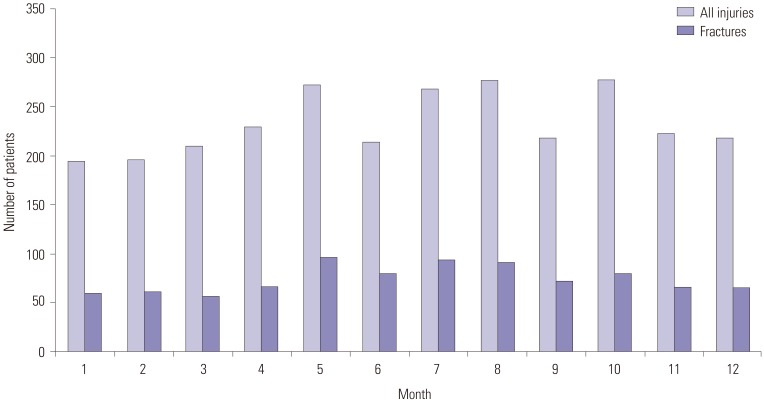
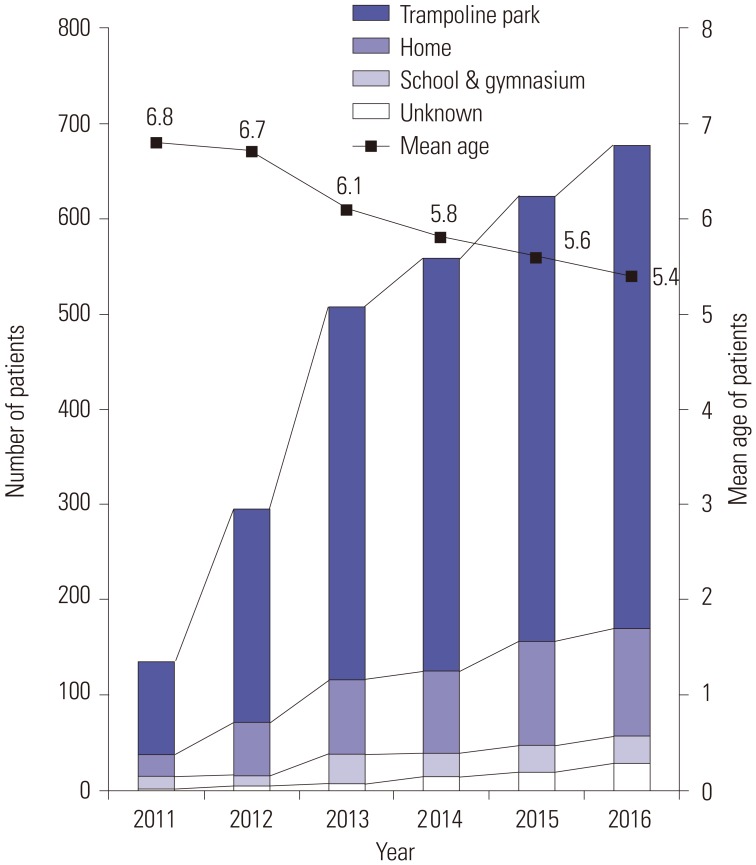
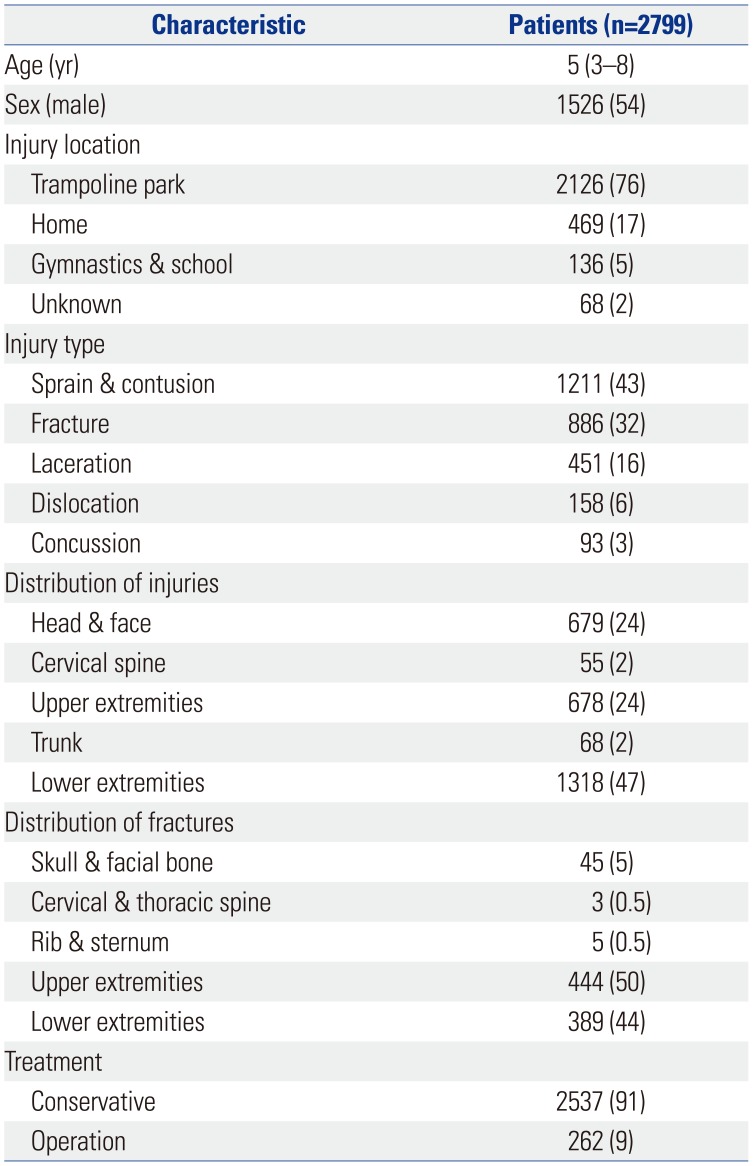
Of 263712 patients between 0 and 17 years of age, 2799 patients with trampoline injuries visited EDs. Their demographic and injury characteristics are summarized in Table 1. Of the patients, 1526 (54.2%) were male. The median age of the patients was 5 years old (interquartile range, 3–8 years old), and 63% of the patients were under 6 years old. The age distribution of patients with trampoline injuries is shown in Fig. 1. The seasonal variation in the incidence of trampoline injuries was little (Fig. 2). There was also no seasonal variation in the occurrence of fractures from trampoline injuries (p=0.422). Trampoline injuries increased steadily from 2011 to 2016, while age at injury decreased gradually over the same period (p<0.001) (Fig. 3).
Distribution of injuries
The lower extremity (47.1%) was the most common site of injury. A fracture was sustained by 886 (31.7%) patients (Table 1). The distal humerus and proximal tibia were the most common fracture sites (34% and 23%, respectively). Operative treatment was required for 262 (9.4%) patients, and their median age was significantly higher than the median age of patients who received conservative treatment (7.0 vs. 5.0 years, p<0.001).
Comparison of patients with trampoline injuries by injury mechanism
The most common mechanism of injury was falling or landing incorrectly, which generally occurred at younger ages than did the other mechanisms (p<0.001) (Table 2). Injuries of the head and face were more frequent in the “collision with other jumpers” and “fell off trampoline” groups (p<0.001). The incidences of fracture and operation were higher in the “landed incorrectly” and “contact with other structures” groups (p<0.001).
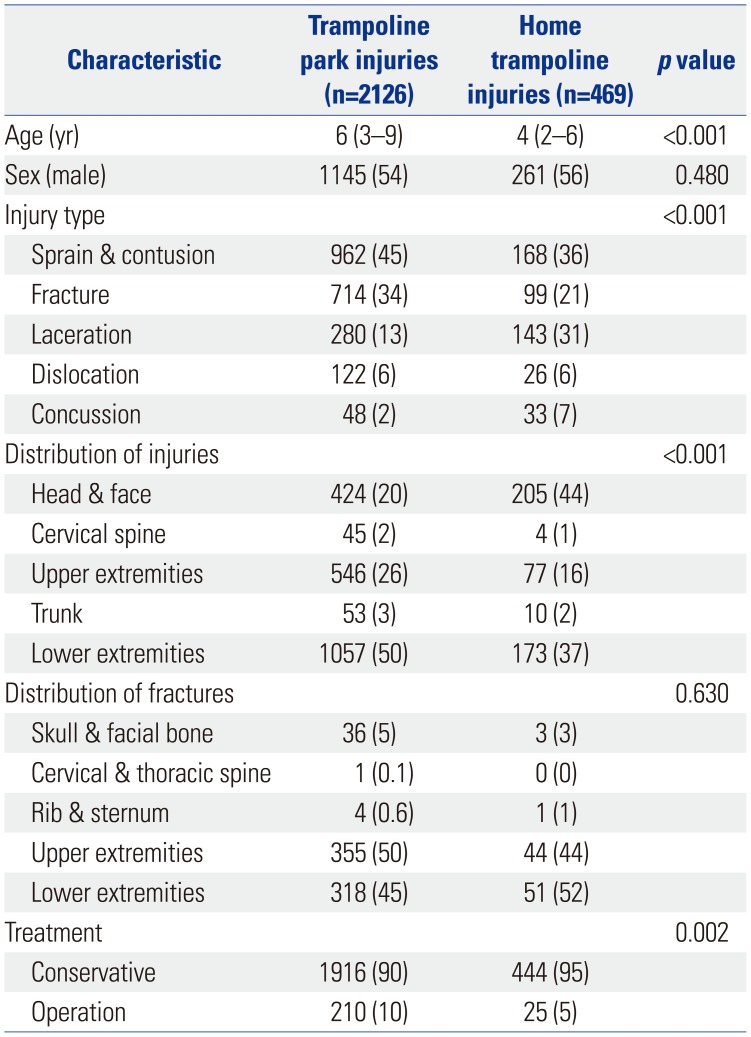
Trampoline park injuries
Trampoline park injuries accounted for 76% of all injuries, and their proportion has steadily increased from 72% in 2011 to 75% in 2016 (p=0.044) (Fig. 3). Sprain and contusion and injuries of the lower extremity were common among trampoline park injuries, and laceration and injuries of the head and face were relatively frequent among home injuries (Table 3). Patients injured at trampoline parks were more likely to have fractures [odds ratio (OR) 1.89; 95% confidence interval (CI) 1.49–2.40] and to require operations (OR 1.95; 95% CI 1.27–2.98).
DISCUSSION
This study is the first to investigate trampoline injuries using a nationwide database of an Asian country. Analysis of the database showed different patterns of injury than have been reported in previous studies. In Korea, trampoline injuries increased sharply during the study period, while age at injury decreased gradually. Most of the injuries occurred in trampoline parks, and most injured children were under 6 years of age.
Young age at injury
The children who suffered from trampoline-related injuries were younger in our study than in reports from the United States and Europe (Table 4). Previous studies have reported that early school-aged children are injured most frequently, with an average age between 8 and 9 years.26121314 In those reports, patients younger than 6 years comprised 22–37% of the injured children.6 In our study, however, the median age at injury was 5 years, and 63% of the injured children were younger than 6 years. These results indicate that children in Korea start to use a trampoline at earlier ages than in other countries. We know that younger children are more prone to bone injuries, including fractures.15 It is noteworthy that age at injury is steadily decreasing in the EDIIS database. Proper guidelines are needed to prevent trampoline injury among young children.
Lack of seasonal variation
In the present study, we did not observe seasonal variations in trampoline-related injuries. Klimek, et al.16 reported that the majority of trampoline injuries (75%) occur between April and September. They inferred that the frequency of injury is reduced in the winter because it is often too cold to jump on home trampolines, which are usually located outdoors.16 However, our Korean study showed an even distribution of injuries across the year. This unique seasonal distribution may be attributable to increased use of indoor trampolines.
Trampoline park injuries
In agreement with previous research, we found that trampoline park injuries pose higher risks of fracture and operation than home trampoline injuries.11 Trampoline park injuries are an emerging concern, and there are few studies on this topic. In previous studies, nearly all trampoline injuries occurred at home. In the United States, the NEISS reported that trampoline park injuries accounted for only 11% of all trampoline-related injuries in 2014.11 Reports from New Zealand and the United Kingdom have shown similar results. However, our study demonstrated that 76% of trampoline-related injuries took place at trampoline parks. We postulate that the distinct injury patterns found in this study, including the early use of trampolines and even seasonal distribution, might be due to increases in the number of trampoline parks in Korea. Unlike in the United States and Europe, the growing popularity of trampolines in Korea is linked to interest in indoor trampoline parks.1718
Safety guidelines for trampoline injury
The American Academy of Pediatrics and the American Academy of Orthopedic Surgeons have repeatedly advised against recreational trampoline use. In addition, several guidelines have been published for pediatric trampoline use.1920 The guidelines include the following safety rules: there should be strict supervision by an adult at all times, only one person should use the trampoline at a time, those using trampolines should be older than 6 years of age, no ladders should be used, no stunts should be performed, safety equipment (shock-absorbing pads, enclosure netting) should be used, the trampoline should be at ground level, it should be placed away from structures, and bounces should be made near the center of the mat.
While, in Korea, trampoline parks are increasing more and more, there is no legal obligation to designate a trampoline safety manager. There is also no age limit for using trampolines. Considering this context and our results, children in countries with many trampoline parks, such as Korea, are in danger of trampoline injuries. In these countries, safety policies for pediatric trampoline use are needed. Our results will help to promote safe trampoline use and aid in the development of future policies for trampoline use.
Some limitations of this study should be acknowledged. First, although this is a multicenter study, the study population was enrolled from only 23 largest EDs in Korea. Because there are several dialectal expressions that mean “trampoline” in Korea, there may be missing patients who had trampoline injuries, but who we could not identify in EDIIS database. Second, information on the outcomes of patients is not included in the EDIIS database. The outcomes of patients with trampoline-related injuries need to be studied further.
In conclusion, in Korean children, trampoline injuries increased steadily over the years, while age at injury decreased gradually. Trampoline parks were the most common location of injury. Although further investigations are required to confirm the distinct features of trampoline-related injuries in Korea, our results suggest that policies need to be developed to prevent pediatric trampoline injuries.


 XML Download
XML Download