

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Adenoid cystic carcinoma (ACC) is a locally aggressive salivary gland neoplasm characterized by its long clinical history with multiple recurrences and late distant metastasis.1 Distant metastasis can develop over more than 10 years after the initial treatment, and 10-year survival has been shown to decrease by 30% in ACC patients with distant metastasis. Distant metastasis has often been associated with advanced stage tumors, although one study reported occurrence of distant metastasis in 47% of patients with early stage ACC, suggesting that distant metastasis can readily occur in ACC patients regardless of the tumor stage.2
One of the main oncogenic drivers of ACC is the tumor type-specific chromosomal translocation t(6;9) (q22–23;p23–24) resulting in Myb-NFIB fusion oncogene. Myb-NFIB fusion contributes to Myb overexpression and activation of critical Myb target genes, including those associated with apoptosis, cell cycle control, cell growth, angiogenesis, and cell adhesion.3 Recent studies in surgical pathology have shown that overexpression of Myb occurs in most ACCs (89%), including ACCs without Myb-NFIB fusion, suggesting Myb expression as a useful marker for ACC.45 Despite Myb activation being an important diagnostic marker of ACC, its value as a prognostic marker was rather limited.3
Ataxia telangiectasia mutated (ATM) is a 370-kd protein belonging to a family of phosphoinositide 3-kinases with roles in DNA processing, regulation of the cell cycle, and control of telomere length. The principal function of ATM is the integration of cellular responses to DNA double-strand breaks.6 Homozygous mutation of the ATM gene results in the loss of detectable protein, triggering ataxia-telangiectasia (A-T),7 an autosomal recessive disorder characterized by neurological and immunological symptoms, radiosensitivity, and predisposition to cancer, particularly of the lymphoid system.89 Accumulating evidence indicates that A-T heterozygotes also have increased risk of developing cancer, breast cancer in particular, for which female ATM carriers have increased risk, compared with the general population.10 Intriguingly, a recent study demonstrated that ATM expression in cancer-associated stroma, as well as cancer cells, can serve as an independent prognostic marker in early stage breast cancer.11 Loss of ATM expression has also been associated with poor prognosis in pancreatic cancer and gastric cancer.1213
As a downstream target protein of ATM, p53 is recognized as the most common tumor suppressor in human malignancies. The mutational status of p53 is an independent unfavorable prognostic marker in many malignancies.14 Due to the lack of biological markers for assessing the prognosis of ACC patients, this study attempted to investigate the role of ATM and p53 expressions in predicting the survival of ACC patients. The prognostic biomarkers obtained in this study will likely facilitate more accurate assessment of ACC patients, thereby allowing more timely application of proper treatments and improving prognosis.
MATERIALS AND METHODS
Human tissue samples
This study included 48 surgical samples identified as ACC of the salivary glands at the Department of Oral Pathology, Dental Hospital, Yonsei University from 1990–2015. This study was approved by the Institutional Review Board of the Faculty of Dental Sciences, Yonsei University, South Korea (2-2015-0031). The clinical information of all patients was collected retrospectively through medical records (Table 1). All cases were confirmed histologically in accordance with the guidelines of the latest World Health Organization classification of salivary gland tumors, based on hematoxylin and eosin-stained tissue sections.15 There was no age, sex, ethnicity, or tumor stage restriction on patient enrollment. Follow-up was calculated as the time from the first visitation at the institution for the primary tumor to the latest follow-up or deceased date.
Immunohistochemical staining
The staining was performed on 4-µm-thick sections using an EnVision-HRP detection system (Dako, Carpinteria, CA, USA). All procedures were performed at room temperature. Sections were deparaffinized through a series of xylene baths and rehydrated in graded concentrations of alcohol. To retrieve antigenicity, the slides were steamed with 10 mmol/L of citrate buffer (pH 6.0; DakoREAL™). Tissue sections were treated with 3% hydrogen peroxide to block endogenous peroxidase activity, followed by incubation in 5% bovine serum albumin. The sections were then incubated with primary antibodies diluted with phosphate buffered saline for 90 min in a humid chamber. All information on primary antibodies is listed on Supplementary Table 1 (only online). The slides were then incubated with secondary EnVision reagent (Dako) for 30 min, followed by incubation with diaminobenzidine chromogen. Next, the sections were counterstained with Mayer hematoxylin for visualization. The phosphate-buffered saline solution without primary antibody treatment was applied as the negative control for all antibody staining. Human lymphocytes and normal salivary glands were used as positive controls for ATM staining as recommended by Villaruz, et al.16 A paraffin-embedded breast cancer cell line was used to determine appropriate dilution ratio and as a positive control for p53 and phospho-p53 (S15).
With a cutoff of >25% positive cells, positivity of nuclear Myb expression was determined according to previously reported guidelines,17 whereas “loss of ATM expression” was determined as tumors showing >25% ATM-negative cells.18 Because mutant p53 proteins generally have longer half-lives than wild-type p53 protein, which leads to their nuclear accumulation, tumors showing >20% nuclear p53 or phospho-p53 (S15)-positive tumor cells were determined as having positive p53 or phospho-p53 (S15) expression.19
Statistical analysis
Correlation between clinical findings and patient survival was analyzed by Fisher's exact test. Cumulative survival probabilities were estimated using the Kaplan-Meier method. All statistical analyses were performed using statistical software (SPSS version 21.0, IBM Corp., Armonk, NY, USA), and the level of statistical significance was set at p<0.05.
RESULTS
Characteristics of the patients
The clinicopathological characteristics of the patients are listed in Table 1. The age range of the patients was 26–71 years; median age at diagnosis was 55 years. Among the 48 patients, 25 (52.1%) were male; 26 (54.2%) were younger than 55 years old. Thirty-six tumors (75%) were found in minor salivary glands, and most of them (47.9%) were in the palate, followed by the submandibular gland (16.7%), floor of the mouth (12.5%), and parotid glands (6.3%). Histologically, 13 tumors (27.1%) were diagnosed as ACC solid type; 35 tumors (72.9%) were diagnosed as ACC tubular and cribriform type. perineural invasion was found in 29 cases (60.4%) of ACC samples.
The median follow-up period for the patient population was 5 years. During that time, local recurrence and distant metastasis were identified in two (4.2%) and 18 (37.5%) of 48 patients, respectively. Five (10.4%) of the 48 patients died during follow-up (Table 2). Of the deceased patients, four (80%) were older than 55 years, and all tumors were found in minor salivary glands: two of them were solid type, three of them had perineural invasion, and four of them showed distant metastasis. Since the hallmarks of poor prognosis are solid histological type, perineural invasion, and distant metastasis,2 Kaplan-Meier analysis was performed to evaluate whether these factors affected prognosis. Histological type and perineural invasion were not significantly correlated with survival rate, whereas distant metastasis was found to be significantly correlated with poor survival (p=0.044) (Supplementary Fig. 1A-C, only online).
Myb expression pattern in ACC
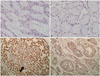
All 48 ACC patient samples were screened for Myb staining. Myb expression was not detected in nontumoral salivary gland parenchyma. Overall, 41 of 48 ACC samples (85.4%) were positively stained for Myb. Myb expression was detected in the nucleus and ranged from negative to strongly positive in intensity. In tubular foci, positive signals were predominantly found in myoepithelial cells (Fig. 1). Myb expression did not significantly differ depending on the anatomic site of tumors or clinical features of the patients. However, Myb expression differed significantly based on the histological type of ACC (Table 1). Thirty-three cases of tubular and cribriform ACC (94.3%) showed Myb positivity, whereas eight cases of solid type ACC (61.5%) showed Myb positivity (p=0.011), according to Fisher's exact test. Myb expression had no significant effect on survival rate when Kaplan-Meier analysis was performed (Supplementary Fig. 1D, only online).
Relationship between ATM levels and patient outcomes in ACC
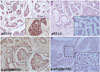
Antibody specificity was validated using human lymph node tissue as a positive control. For negative control, the entire procedure was conducted with the omission of ATM antibody (Fig. 2A and B). For normal salivary glands, ATM protein was detected in the nucleus of acinar and ductal cells (Fig. 2C). ATM expression was reduced/absent in cancer cells and stromal fibroblasts in 58.3% and 60.4% of patients, respectively, compared with that in adjacent normal tissue (Fig. 2D-G). ATM levels in cancer cells were negatively correlated with age (p=0.003). Moreover, perineural invasion was significantly associated with the loss of ATM expression in stromal fibroblasts (p=0.008), according to Fisher's exact test, as shown in Table 3. Kaplan-Meier analysis revealed that low ATM expression in cancer cells was correlated with poor survival (p=0.037). Low ATM expression in stromal fibroblasts, however, was not significantly related to patient survival (Fig. 3A and B). Furthermore, low ATM expression, either in cancer cells or stromal fibroblasts, was not significantly correlated with metastasis-free survival (Fig. 3C and D).
Relationship among p53, phospho-p53 (S15), and patient outcomes in ACC
Of the 48 patients, 38 (79.2%) had p53 expression and 30 (62.5%) had phospho-p53 (S15) expression (Fig. 4). No positive correlation was observed between the expression patterns of these proteins and clinical findings, except for histological type, according to Fisher's exact test (p=0.016) (Table 3). Although statistical significance was not attained, positive p53 expression or negative phospho-p53 (S15) expression showed tendencies of being correlated with poor survival rate (Fig. 5A and B).
Upon analyzing ATM expression stratified by positive p53 expression or negative phospho-p53 expression, loss of ATM and positive p53 expression significantly reduced overall survival (p=0.017) (Fig. 5C). Loss of ATM and negative phosphop53 expression was associated with worse prognosis, although statistical significance was not attained (Fig. 5D). In addition, loss of ATM, given positive p53 or negative phospho-p53 expression, reduced metastasis-free survival, although statistical significance was not attained (Supplementary Fig. 2, only online). As shown in Table 3, all five deceased patients exhibited a loss of ATM expression, as well as positive p53 and negative phospho-p53 expression, confirming that these markers can predict poor prognosis in ACC patients.
DISCUSSION
ATM is activated within seconds to minutes upon exposure to ionizing radiation and can phosphorylate various downstream substrates, some of which play crucial roles in regulating cell cycle arrest, DNA repair, and apoptosis.20 To illustrate, ATM is an upstream regulator of p53, a well-known tumor suppressor: ATM modulates progression of the cell cycle and apoptosis via activation and stabilization of p53.21 In response to ionizing radiation, the kinase activity of ATM is enhanced, leading to phosphorylation of p53 on serine 15 and activation of the checkpoint kinase Chk2, which, in turn, phosphorylates p53 on serine 20. These interactions result in stabilization and activation of p53:2223 serine 15, threonine 18, and serine 20, being key phosphorylation sites of p53, are involved not only in stimulating p53's interaction with the transcriptional machinery but also in inhibiting MDM-mediated repression of p53.24
Mutated p53 is often characterized by increased half-life, as it inhibits its own degradation by the ubiquitin complex.25 Therefore, the level of p53 can be modulated both by the ATM-dependent pathway and the mutational status of p53 itself. The mutational status of p53 itself is an independent unfavorable prognostic marker in many malignancies.14 In terms of ACC, patients with p53-positive expression had a greater chance of developing metastasis, as well as poorer 5-year overall survival.26 In our study, positive p53 expression showed a tendency of being correlated with poor survival, even though statistical significance was not attained.
This study focused on investigating whether the expression patterns of ATM and p53 and its ATM-mediated phosphorylated form are associated with patient survival. The prognostic role of ATM and p53 has previously been demonstrated in human malignancies, including breast,22 pancreas,12 lung,16 and stomach cancer,27 but data thereof in ACC are lacking. All these studies have shown that ATM expression, either independently or in combination with p53 expression, is correlated with patient outcome. In our study, loss of ATM expression in ACC cancer cells was significantly associated with reduced patient survival. In addition, p53-positive expression or phospho-p53 (S15)-negative expression was weakly correlated with poor survival. Interestingly, combined analysis of ATM and p53 had better predictability than individual analysis of each protein. Given positive p53 or negative phospho-p53 (S15) expression, loss of ATM was associated with worse survival. The loss or reduced expression of ATM may render cells susceptible to irreversible DNA damage and subsequent cancerization, ultimately facilitating cancer progression as the cells lose control of differentiation and proliferation.28
Several researchers have retrospectively studied the clinicopathological features of ACC, attempting to identify significant prognostic factors; however, findings remain controversial. Solid histological type and perineural invasion have been considered as important indicators of poor prognosis in ACC patients.2 In particular, the presence of perineural invasion can result in higher rates of recurrence.2930 In our study, however, the prognostic value of perineural invasion was not significant, possibly due to a small sample size limited to minor salivary glands and relatively short follow-up period.
Of note, ATM loss in stroma was strongly correlated with perineural invasion in our study, even though ATM loss in stroma was not correlated with patient survival. As ATM loss in stroma can serve as an independent prognostic marker in early stage breast cancer,11 further study needs to be conducted to unravel the mechanism underlying the association between the loss of ATM in stromal fibroblasts and perineural invasion.
In accordance with previous studies, Myb-NFIB fusion was not expressed in non-ACC neoplasms of the head and neck, confirming the high specificity of Myb-NFIB fusion for ACC.4 All 48 ACC patient samples were screened for Myb staining: 85.4% were positively stained for Myb, whereas Myb staining was negative in nontumoral salivary gland parenchyma. Myb expression was not significantly associated with patient survival, confirming that Myb is a suitable diagnostic marker for ACC, but not a prognostic marker.
Taken together, expression levels of ATM in cancer cells alone or in combination with positive p53 expression hold strong prognostic value for predicting the overall survival of ACC patients, and thus could serve as promising biomarkers to assess patient outcomes. Prognostic values of well-known clinical factors, perineural invasion, and histological types were not evident in this study, possibly due to small sample size and relatively short follow-up period. Additional studies with a larger sample are warranted.






 XML Download
XML Download