

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rectal cancer (RC) constitutes 25% of all primary colorectal cancers, and is characterized by a different set of behavior patterns, compared with tumors arising from the colon.1 In this regard, specific guidelines and protocols were conceived for the diagnosis, staging, and treatment of RC. Since the introduction of sharp rectal dissection along the mesorectum by Heald,2 total mesorectal excision (TME) has become the cornerstone of RC treatment, making a significant impact on local recurrence and functional outcomes. A complete, margin-negative resection is essential to confer the highest possibility of cure.3 Enhancements in imaging modalities have substantially improved RC staging and patient stratification. The use of magnetic resonance imaging (MRI) has allowed for the high-resolution characterization of the extent of tumor involvement, lymph node spread, and encroachment to neighboring organs. Moreover, extramural vascular invasion and a positive circumferential resection margin (CRM) on MRI have become important prognostic factors of recurrence and survival.45
In the last decade, there has been remarkable progress in RC treatment, characterized by relentless efforts to make substantial improvements in local control and the widespread adoption of a multidisciplinary approach. The use of neoadjuvant chemoradiotherapy (CRT) has resulted in significant downstaging and downsizing of tumors, thereupon enabling the performance of sphincter-saving procedures in some cases.67
Despite the emergence of cutting-edge advancements, the management of low-lying RC remains challenging. Low RC is defined as a tumor located <6 cm from the anal verge, although other studies arbitrarily describe it as a tumor lying <5 cm from the anal verge.89 Although the surgical treatment of RC may be well standardized for tumors located in the high and middle rectum, the surgical treatment of low RC remains debatable. The higher risk of local recurrence in low RC, as well as the higher incidence of bowel dysfunction, has made its treatment a formidable endeavor.8 In addition, the critical location of a low RC tumor predisposes it to a CRM that tends to involve the sphincters and the surrounding organs, pelvic lymph node metastasis, and anastomotic issues associated with radiation therapy.8 As a result, patients are susceptible to uncontrolled pelvic tumor, leading to sepsis, bleeding, fecal incontinence, sexual and urinary dysfunction, and pelvic pain.
In response to these challenges, alternative strategies have been explored and attempts to standardize the treatment of low-lying RC have been undertaken. In this review article, we critically examine recent advances in available techniques and contrasting philosophies, and highlight the critical and challenging issues confronted by colorectal surgeons in the management of low-lying RC in order to provide an avenue for a discussion about emerging progress in the field.
MODIFICATIONS OF THE ABDOMINOPERINEAL RESECTION TECHNIQUE
Introduction
In previous years, abdominoperineal resection (APR) was deemed the standard surgical treatment for low-lying RC.1011 Advances in preoperative CRT and refinements in surgical skills led to a reduction in the number of patients undergoing the procedure; however, it is still indicated in patients with tumor invasion to the external anal sphincter and levator muscles and in those with poor anorectal function and inadequate response to CRT.6 A combination of anatomic and surgical challenges complicates conventional APR surgery. In the distal rectum, the mesorectal tissue tapers down at approximately 2 cm above the levator ani muscles; thus, there is less protective tissue volume for the tumor to traverse before involving the CRM.1213 Moreover, the conventional APR technique is associated with the technical difficulty of dissecting deep in the pelvis.1415 Because of these inherent challenges, APR is associated with oncologic outcomes that are inferior to those of low anterior resection, as well as with higher risks of intraoperative perforations and CRM involvement.6
Patient selection
The extralevator abdominoperineal excision (ELAPE) technique has been introduced to answer increasing calls for a modification of the conventional APR technique.10 Holm, et al.16 from the Karolinska University Hospital in Stockholm developed a more radical procedure based on Miles' original technique17 by applying an extended posterior perineal approach, which created a cylindrical specimen and avoided the “waisting” associated with conventional APR. The technique was performed in patients in whom MRI showed a T3 or T4 tumor located within 6 cm from the anal verge or in those with fixed and tethered tumors on rectal examination.16 However, for tumors with encroachment into the external sphincter or levator muscles and poor response to preoperative CRT, APR is still indicated.6
Surgical technique
The ELAPE technique closely resembles Miles' original operation, 17 which involves careful mobilization of the mesorectum up to the level of the levator muscles; however, in this approach, the abdominal and perineal dissections meet just above the levator muscles, leaving the levators attached to the mesorectum and creating a cylindrical specimen with more tissue covering the tumor in the distal rectum. The perineal phase of the procedure is executed with the patient in the prone position. The extended perineal dissection follows the inferior surface of the levator muscles up until the level of the abdominal dissection termination. To enhance visualization, the coccyx is usually removed along with the main specimen. In cases where primary closure is not feasible, a gluteus maximus flap reconstruction of the pelvic floor is performed to cover the perineal defect.1516
Perioperative outcomes
In terms of perioperative outcomes, the initial results by Holm, et al.16 revealed that the extended perineal approach is associated with a lower risk of wound complications. In a study by West, et al.18 comparing ELAPE with traditional APR, ELAPE was associated with a longer operative duration (median operative time: 300 min vs. 185 min, p<0.001), as well as an increased incidence of coccyx removal (99 vs. 3, p<0.001), use of flap reconstruction (80 vs. 0, p<0.001), and perineal wound complications (from 20% to 38%, p=0.019). On the other hand, data from our institution revealed that ELAPE was better than conventional APR in terms of operative time (median: 285 min vs. 355 min, p=0.074), intraoperative bleeding volume (median: 300 mL vs. 360 mL, p=0.546), and length of hospital stay (median: 10 days vs. 17 days, p=0.016). There was no significant difference in terms of postoperative complications between the two.19
Oncological outcomes
Numerous studies have shown the oncologic superiority of the ELAPE technique, especially in terms of CRM involvement and intraoperative perforations. A study by West, et al.18 demonstrated the oncologic superiority of the ELAPE technique in a retrospective study by comparing specimens obtained from ELAPE to those taken using the conventional APR technique. Besides the clinical and pathologic parameters, tissue morphometry was used to ascertain the volume of tissue removed around the tumor in both surgical techniques. The ELAPE technique cleared away more tissue at the distal rectum, which consequently resulted in lower rates of CRM involvement (14.8% vs. 40.6%, p=0.013) and intraoperative perforations (3.7% vs. 22.8%, p=0.0255), than conventional APR.15 Subsequently, West, et al.18 performed a multicenter study on ELAPE involving 11 colorectal surgeons based at nine European institutions. The results revealed that the ELAPE technique removed more tissue (median area: 2120 mm2 vs. 1256 mm2, p<0.001), causing a decrease in CRM involvement (from 49.6% to 20.3%, p<0.001) and intraoperative perforations (from 28.3% to 8.2%, p<0.001), than conventional APR. In a retrospective study from our institution, ELAPE achieved a longer lateral margin (median: 7.5 mm vs. 4.0 mm), harvested more lymph nodes (median: 17 vs. 12, p=0.076), and decreased the rate of harvesting <12 lymph nodes (23.1% vs. 46.2%, p=0.295), compared with conventional APR (23.1% vs. 11.5%).19
Functional outcomes
Although studies have been limited, the functional outcomes of ELAPE have been encouraging. In the study by West, et al.,18 there was no significant difference in terms of postoperative sexual and urinary dysfunctions between conventional APR and ELAPE. Likewise, in a prospective study by Vaughan-Shaw, et al.,20 quality of life (QoL) analysis after ELAPE showed high physical, emotional, and social functioning scores that were comparable to published data on functional outcomes of conventional APR.
Summary
ELAPE is a feasible technique with acceptable perioperative, oncologic, and functional outcomes. Moreover, the aforementioned studies solidify the perception that it is comparable and not inferior to conventional APR. Clearly, the modified technique offered the advantages of reducing CRM involvement by removing the levator muscles along with the mesorectum and anal canal en bloc and increasing the amount of protective tissue around the tumor. In addition, the prone jackknife position provided better visualization by allowing the rectum to descend outward after opening the pelvis, thereby revealing the plane between the rectum and the adjacent organs and preventing inadvertent tumor perforation.18 The increased susceptibility to perineal wound complications has been considered the main drawback of the ELAPE procedure; however, this can be partially circumvented with the use of myocutaneous flaps. In this regard, more studies are needed to determine the factors that would assist in identifying patients with an increased risk of perineal wound infections.
TRANSANAL TME: A NEW APPROACH TO TME
Introduction
Oncological outcomes, particularly local disease control, in RC depend heavily on obtaining a quality TME specimen with an intact mesorectum and adequate radial and distal margins. TME is a challenging procedure for even the best colorectal surgeons. In particular, visualization can be difficult in an obese patient with a bulky tumor and a narrow pelvis, leaving limited space for pelvic dissection. Having an anteriorly located distal tumor can also complicate the situation for these patients by predisposing them to a higher risk of CRM involvement.21 Furthermore, difficult introduction of instruments and poor stapler ergonomics in the pelvis are obstacles in ensuring a secure distal margin, requiring multiple stapler firings that can result in asymmetrical staple lines and increased risk of anastomotic leakage.3 The use of a minimally invasive approach was introduced to provide better visualization and assist in rectal mobilization; however, the same anatomic challenges seen in open rectal surgery remain unanswered, especially the capability of securing an adequate distal margin and achieving a complete TME with an uninvolved CRM.322 Robotic surgery was introduced to compensate for the technical limitations of traditional laparoscopy. The robotic system provided improved dexterity and ergonomic efficiency through its stable camera, stereoscopic views, three-dimensional imaging, and seven degrees of articulation; nonetheless, it has failed to address the problems of securing an adequate distal margin and the difficult retraction deep in the pelvis.222324 In response to these challenges, transanal TME (taTME), also referred to as “bottom-to-up” TME, was developed to provide a more direct approach to the most complicated phases of dissection in the distal rectum, to assure an adequate distal resection margin, and to facilitate sphincter preservation.24
Patient selection
The performance of TME via a transanal approach evolved from previous experience with transanal local excision and advances in microsurgical endoscopic surgery.21 Indeed, it is an acquired concept combining important surgical techniques, such as transanal endoscopic microsurgery, transanal transabdominal approach, and transanal minimally invasive surgery.25 A consensus about the indications of taTME was published after the Second International Transanal Total Mesorectal Excision Conference. Experts recommended taTME in patients with the following characteristics: 1) male sex, 2) narrow and deep pelvis, 3) obesity, 4) tumor >4 cm, 5) prostatic enlargement, and 6) distorted planes caused by irradiation.26
Surgical technique
Over the years, the taTME technique has gradually undergone refinements to allow for careful excision of low rectal tumors. At present, it is commonly executed as a combined procedure with both abdominal and perineal phases. These phases can be performed simultaneously, with separate surgical teams, or in sequence, beginning either transanally or transabdominally. The transanal phase is initiated by exposing the anal canal using a Lone Star retractor (Lone Star Medical Products, Houston, TX, USA). Initial rectal incision would vary depending on the location of the tumor in the anorectal canal. For tumors located distally or invading the anorectal junction (<1.5 cm), a partial intersphincteric dissection is carried out before the placement of a distal purse string at least 1 cm below the tumor. For more proximal tumors, the rectal purse string is positioned at a safe distance that can secure a clear distal margin. The abdominal phase commences with trocar insertion and carbon dioxide insufflation at 15 mm Hg to facilitate the performance of a full-thickness rectotomy. During this step, surgeons must be aware that an intramural dissection may occur and result in a positive margin. Subsequently, TME dissection is performed. After completion of the TME, the specimen is extracted either via the transanal or transabdominal route. Following specimen extraction, a hand-sewn or stapled colorectal anastomosis or coloanal anastomosis (CAA) is performed.2728 Penna, et al.27 summarized taTME in five essential steps: 1) placement of a distal circumferential purse string, 2) full-thickness rectotomy, 3) TME, 4) specimen extraction, and 5) anastomosis.
Perioperative outcomes
Since the initial experience of Sylla, et al.29 and Lacy, et al.,30 numerous studies have demonstrated encouraging results about the safety and efficacy of taTME. From 2011 to 2014, Lacy, et al.31 conducted a study in a prospective series of 140 taTME cases. The results showed no conversions or intraoperative complications. Pathological analysis revealed that a complete TME specimen was obtained in 97.1% of patients, whereas 2.1% had a nearly complete mesorectum. Minor complications occurred in 24.2% of the patients, whereas 10% experienced major complications. No mortality was recorded in the series. Penna, et al.25 of the International taTME Registry Collaborative published the results of the first 720 taTME cases from 66 registries in 23 countries. taTME obtained intact TME specimens in 85%. Abdominal conversion occurred in 6.3%, whereas perineal conversion to a more extensive abdominal surgery was required in 2.8%. In short-term outcomes, the rates of postoperative mortality and morbidity were 0.5% and 32.6%, respectively.
Oncologic outcomes
In terms of oncologic outcomes, studies on taTME have demonstrated encouraging results. In the series of de Lacy, et al.,31 2.3% had local recurrence and 7.6% had systemic recurrence after a follow-up period of 15 months. Recently, Marks, et al.24 published the first report on long-term outcomes of taTME for RC in a cohort of 373 patients. After a mean follow-up period of 5.5 years, the local recurrence and distant metastasis rates were 7.4% and 19.5%, respectively, and the 5-year survival rate was 90%. The long-term results of the study showed that taTME is a promising technique that can yield adequate distal margins and CRMs with good-quality specimens.
Functional outcomes
The first prospective assessment of patients' functional outcomes and QoL after taTME has recently been published by Koedam, et al.32 Using validated questionnaires, patients who underwent taTME were evaluated at the VU University Medical Center in Amsterdam (Vrije Universiteit Amsterdam). One month after taTME, QoL, functioning, fatigue, functional bowel disturbance, generalized body pain, and anal scores were significantly reduced; however, the scores reverted to baseline values after 6 months, except for anal pain and social function parameters.32
Summary
Initial experience suggested that taTME has the potential of yielding better specimen quality, less morbidity owing to improved anastomosis, and more sphincter-saving procedures without risking oncologic outcomes. Moreover, preliminary results on functional outcomes are comparable to those of laparoscopic TME in published data, showing significant reduction in QoL parameters at 1 month after surgery, with subsequent recovery to baseline values by 6 months.33 The COLOR III trial, the first multicenter randomized clinical trial to compare taTME vs. laparoscopic TME, has begun. The trial was built on the premise that taTME would yield superior oncologic outcomes to those of conventional laparoscopic TME, thereby reinforcing the results of previous cohort studies.34 Despite the encouraging initial results, surgeons must be judicious in adopting taTME into surgical practice. taTME is technically demanding and requires steep learning curve. In addition, owing to the technical difficulties of distinguishing the correct tissue planes, surgeons should be aware of certain intraoperative complications that may occur during taTME procedures, such as injuries to the urethra and major pelvic vessels.2125 The wait for the results of the COLOR III trial is fueled with anticipation. In the meantime, structured taTME training and mentorship are essential for surgeons who wish to adopt the taTME technique, and more trials should be undertaken before its widespread implementation in surgical practice.26
SPHINCTER PRESERVATION
Intersphincteric resection and CAA: anal preservation in RC surgery
Introduction
Better understanding of sphincter anatomy, enhanced surgical techniques, and advances in CRT have brought about the evolution of RC treatment from APR to sphincter-preserving surgery (SPS).35 In recent years, ultralow anterior resection (uLAR) with or without intersphincteric resection (ISR) and CAA has been performed, enabling anal preservation with secure distal and radial margins and striking a balance between oncologic cure and maintenance of anal function.36 In 1994, Schiessel, et al.36 introduced the groundbreaking technique involving the removal of the internal sphincter and dissection extending into the intersphincteric plane. To achieve an adequate distal margin, a portion of the puborectalis or external sphincter may be removed with the specimen.36 With its acceptable oncologic outcome and preservation of anal function, adaptation of ISR with CAA has increased and has largely replaced APR; nevertheless, APR is still indicated when there is infiltration of the intersphincteric space to avoid leaving tumor cells at the resection margin.37
Patient selection and types of ISR
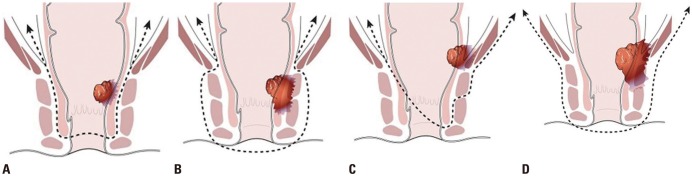
Intersphincteric resection is indicated for patients with distal rectal tumors confined to the internal sphincter, not involving the external sphincter, and located below the anorectal ring within the surgical canal. In recent years, the technique has undergone significant refinements and modifications. Partial removal of the external sphincter is also performed if there is invasion into the intersphincteric space and/or external sphincter muscles.3738 A Japanese study group defined three types of ISRs: Total ISR is performed when the tumor has spread beyond the dentate line, and involves complete removal of the internal sphincter. Subtotal ISR is performed when the distal edge of the tumor is >2 cm from the dentate line, and involves resection of two-thirds of the internal sphincter. Partial ISR is performed when there is enough distal margin above the dentate line, and involves only resection of one-third of the internal sphincter (Fig. 1).38394041
Surgical technique
Meticulous dissection of the anatomical plane between the internal and external sphincters forms the basis of the ISR technique, which frequently involves three essential phases: an abdominal phase, followed by a perianal phase, and concluded by a second abdominal phase. The initial abdominal phase commences with ligation of the inferior mesenteric artery at the root of its origin from the abdominal aorta, with clearance of the lymph nodes along its course and division of the inferior mesenteric vein beneath the pancreas. After adequate mobilization of the descending and sigmoid colon up to the level of the splenic flexure, TME is performed and dissection proceeds down to the anal canal through the intersphincteric plane. The perianal phase of the procedure follows the complete dissection of the rectum and mesorectum. A Lone Star retractor (Lone Star Medical Products) is applied to expose the mucosa and allow better access and visualization. In this phase, a 1–2-cm distal resection margin is of utmost importance and must be ensured whenever possible. A circumferential incision is utilized commencing at the intersphincteric groove. Posterior dissection is initiated at the intersphincteric groove for total ISR, at the level of the dentate line for partial ISR, and in between the dentate line and intersphincteric groove for subtotal ISR. The intersphincteric plane is utilized for the anterior and lateral dissections, progressing until the intraperitoneal rectum is reached. The tumor-bearing rectum is eventually delivered either through the anus or abdominal wound, and resected with an adequate proximal margin. A coloanal tension-free anastomosis is then performed. The procedure concludes with a second abdominal procedure for the placement of closed suction drains and creation of a diverting ileostomy.4243
Postoperative outcomes
Numerous studies have demonstrated favorable surgical, oncological, and functional outcomes for ISR.383944 In 2005, Schiessel, et al.45 published the long-term follow-up data of 121 patients who underwent ISR. Their findings revealed that the 30-day complication rate after the operation was 7.7% (n=9), whereas the mortality rate was 0.8% (n=1). Among the 9 patients who experienced early postoperative complications, 7 patients (5.1%) developed anastomotic fistula, which healed spontaneously, whereas the other 3 patients required surgical intervention. In terms of late complications, anastomotic stricture occurred in 11 patients (9.4%), necessitating perianal dilatation.45 These findings were supported by a systematic review by Akagi, et al.,38 which revealed an overall complication rate ranging from 7.5% to 38% and an operative mortality rate of <2%. Anastomotic leakage occurred in 4.3–48%, with the development of subsequent stricture observed in 8.4–15.9%. Aside from anastomotic leakage, postoperative complications also included ileus, colonic ischemia, pelvic abscess, and development of ano-vaginal fistula.38 In recent years, a robotic platform has been introduced to overcome the inherent challenges of laparoscopy.46 Baek, et al.35 compared outcomes in 84 patients who underwent uLAR with those in patients who underwent CAA with or without ISR using the robotic or laparoscopic approach. The results revealed that patients who underwent robotic surgery had lower conversion rates (robot 2.1% vs. laparoscopy 16.2%, p=0.011) and had shorter hospital stays than patients in the laparoscopic group (robot 9 days vs. laparoscopy 11 days; p=0.011). Likewise, a subsequent study at our institution revealed that postoperative recovery was significantly faster after minimally invasive surgery (robotic and laparoscopic) than after open surgery. The period of hospitalization, time until first flatus, and time until the initiation of soft diet were significantly shorter after minimally invasive surgery (unpublished).47 Recently, Kim, et al.48 evaluated robotic ISR by comparing ISR and APR using either robotic or open approaches. The results revealed that the use of robotic surgery was the most significant predictor of ISR achievement [odds ratio (OR) 3.467, 95% confidence interval (CI) 2.095–5.738, p<0.001]. Postoperatively, surgical complications were more common in the open ISR group (16% vs. 7.7%, p=0.01).
Oncologic outcomes
Mounting evidence suggests that ISR is an oncologically acceptable surgical alternative to APR for low RC. In the long-term cohort of Schiessel, et al.,45 5.3% (n=6) patients developed local recurrence and 3.5% (n=4) died within a median follow-up time of 94 months. The systematic review by Akagi, et al.38 yielded satisfactory oncologic outcomes, with reported overall recurrence, distant metastasis, and local recurrence rates of 13.3–19.4%, 2.5–19.0%, and 0–22.7%, respectively. Similarly, the survival rates were favorable with disease-free and overall 5-year survival rates ranging from 69% to 86% and 79% to 97%, respectively. The use of robotic systems has considerably influenced the oncological outcomes of the ISR technique in recent years. Studies comparing long-term feasibility between robotic ISR and laparoscopic ISR have demonstrated that there are no significant differences in terms of local recurrence, overall survival, or disease-free survival between the two techniques. Moreover, investigators have lauded the ergonomic efficiency of the robotic platform, with its improved dexterity and visualization.4849
Functional outcomes
Despite the introduction of anal preservation with ISR, anal dysfunction remains a major concern. Low anterior resection syndrome (LARS), consisting of symptoms of stool frequency, fecal incontinence, or urgency, frequently occurs after sphincter-preserving operations.38 In the long-term study by Schiessel, et al.,45 ISR resulted in a reduction of anal resting pressure, remaining constant during the whole observation period. In contrast, maximum squeeze pressure, which was significantly diminished after ISR, was gradually restored during the follow-up period. Clearly, the aspect of time is essential in evaluating functional outcomes after ISR. Several factors have been found to be inimical to anal function, predisposing patients undergoing ISR to strictures, stool frequency, and fecal incontinence.6 Particularly, preoperative CRT has been highlighted as an adverse factor affecting anal continence after ISR. In a long-term study by Saito, et al.,50 despite 70% of patients showing good continence (Wexner score ≤10) at >5 years post-ISR, neoadjuvant treatment and male sex were shown to result in poor postoperative functional outcomes. In their experience, a more effective CRT was strongly associated with anal dysfunction, thereby reflecting the extent of neural degradation that would ensue during treatment.
Summary
The introduction of the ISR technique has challenged the conventional belief that adequate fecal continence necessitates the preservation of an intact internal sphincter. Moreover, it has offered a feasible alternative for patients who would otherwise need an APR. In our opinion, adequate preoperative planning, proper patient selection, and a precise technique with minimal trauma should be ensured to achieve success with this procedure. The implementation of a robot-assisted approach for ISR has allowed for efficient dissection into the intersphincteric plane with its enhanced mechanical dexterity and clear visualization of the deep pelvis. Thus, we recommend careful patient selection to achieve adequate distal clearance and better functional results. The use of preoperative radiotherapy has been shown to have a negative impact on anal function, making ISR patients susceptible to anastomotic strictures, stool frequency, and urinary incontinence.6 In this regard, we propose that assessment of anal function be performed before planning this type of surgery, taking into account the patient's age and level of activity.
Hemilevator excision
Introduction
The advances in CRT, improvements in surgical instrumentation, and excellent pathological outcomes have allowed low-lying RC to be approached in a multidisciplinary manner. The choice of procedure is always a matter of debate, especially when the goals are sphincter preservation and oncologic safety. Despite the recent advances in surgical techniques, total levator ani muscle excision to achieve an adequate CRM has routinely been performed for tumors at the level of the anorectal junction. Nevertheless, there is the possibility that en bloc resection of the tumor-bearing rectum can be performed without compromising anal function in tumors limited to an ipsilateral levator ani muscle with an intact external anal sphincter. Anatomic studies have conveyed the existence of an anatomic separation between the puborectalis muscle and the external anal sphincters.5152
Patient selection and methodology
Recently, our institution introduced the hemilevator excision (HLE) technique followed by ISR and CAA to provide greater sphincter preservation and obtain oncologic clearance for tumors partially invading one side of the levator ani. This technique exploits the advantages of the robotic platform in the dissection at the levator ani muscles and the 1-sided excision of the levator ani and deep part of the external sphincter through the intersphincteric plane.53 A preliminary report about this novel technique has recently been published. Data on 13 patients who underwent HLE at our institution were collected. RC tumors located at the level of the anorectal ring and invading or abutting the ipsilateral levator ani were included in the study, whereas tumors invading beyond the levator ani muscle with extension toward the external sphincter, recurrent tumors, and anal cancer were excluded. Preoperative long-course chemoradiation (LCRT), consisting of 50.4 Gy in 28 fractions for 6 weeks with two cycles of 5-fluorouracil or capecitabine-based chemotherapy, was administered to all patients, after which surgery was performed 4–8 weeks later. All of the 13 patients included in the study presented with low rectal tumors at the anorectal ring level that were suspected to encroach or border on the ipsilateral levator ani or pelvic floor muscles on MRI, even after preoperative LCRT.41
Surgical technique
HLE was carried out with the patient placed in a steep Lloyd-Davies position. The procedure consisted of an abdominal and a perineal phase. The abdominal phase commenced with mobilization of the colon until the splenic flexure and ligation of the central vessels. Thereafter, TME was performed followed by dissection toward the levator ani muscles. Then, rectal tumor and ipsilateral levator ani extirpation was performed with an adequate margin. After pelvic floor dissection and HLE were achieved, the perineal phase of the procedure was initiated. During the perineal phase, the patient's hips were placed in a flexed position to provide better access and visualization. The perineal phase commenced with an incision at the line of Hilton on the rectal tumor side to approach the intersphincteric space. Dissection was then advanced in between the internal and external anal sphincters 0.5–1 cm below the rectal tumor, where the course of dissection took a diagonal turn to include the deep portion of the external sphincter. The dissection was continued in the cephalad direction to encompass the levator ani muscle, before the pelvic cavity was entered. On the opposite side of the tumor, incision was made on top of the dentate line and dissection progressed to the medial plane of the internal sphincter, allowing entrance to the pelvic cavity. After complete removal of the rectum, the rectum and sigmoid colon were drawn out through the anus and transected. A sleeve-fashioned resection was performed to the distal rectum; thereafter, bowel continuity was restored using a hand-sewn CAA. A loop ileostomy was created in all patients who underwent the procedure.41
Postoperative, oncologic, and functional outcomes
The HLE technique demonstrated favorable postoperative surgical outcomes. Anastomotic leakage necessitating percutaneous drainage manifested in 2 patients. Parastomal hernia occurred in 1 patient, requiring stomal revision. Oncologically, a clear resection margin from the tumor was achieved in all cases. During follow-up, 1 patient had local recurrence at the anastomotic site 4 months after surgery, whereas 2 patients had systemic recurrences in the lung and liver at 25 and 6 months after surgery, respectively. In terms of functional outcomes, incontinence was evaluated using the incontinence grading scale recommended by Jorge and Wexner. Among the 6 patients who underwent takedown of ileostomy after the initial operation, 2 patients experienced fecal incontinence. One patient experienced two to three episodes of bowel movement per day that required a pad. The other incontinent patient experienced frequent episodes of bowel movement of >10 per day, but did not require the use of a pad. Among the patients who underwent ileostomy reversal, the mean Wexner score was 9.4.41
Summary
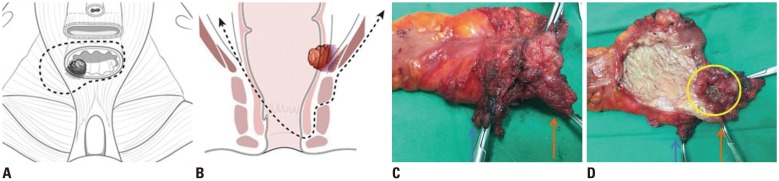
The preliminary results of the HLE technique exemplify that the advent of cutting-edge imaging modalities has made preoperative evaluation more accurate, enabling a meticulous selection of patients for a specific surgical procedure. Particularly, MRI has been helpful in delineating the exact location of a tumor, allowing patients otherwise considered to be APR candidates to undergo less extensive surgery.41 In contrast to the high rates of positive CRM after APR and extralevator APR in the literature, all patients in our series presented with negative CRM involvement. In addition, no patient presented with a positive distal resection margin, further reinforcing the oncologic feasibility of the HLE technique. Moreover, the use of robotic systems has permitted more precise dissections in the pelvic cavity, which has allowed HLE to be performed with adequate margins. On the basis of these preliminary results, we concluded that HLE might be a sensible alternative to APR or extralevator APR for low RC with invasion to the ipsilateral side of the levator ani muscle (Fig. 2). Notwithstanding the promising results, long-term outcomes, especially the effects on anorectal function, should be investigated, and a larger trial needs to be undertaken before the technique can be widely implemented.
PELVIC LYMPH NODE METASTASIS: A PHILOSOPHICAL DIVIDE
Introduction
Local recurrence remains a major problem in RC surgery, and is associated with severe morbidity and low survival. Regional lymph node spread and CRM involvement are independent prognostic factors of local recurrence. The presence of extra-regional lymph node metastasis, which refers to lateral pelvic lymph nodes (LPLNs) or para-aortic lymph nodes, however, confers a higher recurrence rate.54 The high incidence of pelvic node metastasis remains a critical issue in the management of low-lying RC, signifying that the disease has already escaped the confines of the regional space.55
Patient selection
The optimal management of LPLNs remains disputed, and has engendered a philosophical tug-of-war between the East and the West. The Japanese Society for Cancer of the Colon and Rectum guidelines for the treatment of cancer 2016 recommend TME/tumor-specific mesorectal excision and LPLN dissection (LPLND) to improve local control and survival in patients with advanced lower RC.56 They reported that, among patients whose lower tumor borders were located distal to the peritoneal reflection, the incidence of lateral lymph node metastasis was 20.1%. These findings imply that TME alone cannot cannot eliminate potentially metastatic lymph nodes. Hence, LPLND is indicated if the tumor is located below the peritoneal reflection and invades further off the muscularis propria.56
Surgical technique
LPLND is a technically demanding technique, commencing after the completion of TME dissection. The ureter and hypogastric nerve are secured to establish the inner border of dissection. After determining the iliac artery bifurcation as the cranial boundary of dissection, dissection proceeds along the external iliac artery and the external iliac vein until the major psoas muscle is reached. Once the presence of the obturator nerve, obturator vein, and obturator artery is confirmed, dissection proceeds in a caudal direction, with the dissection along the obturator artery progressing from its origin toward the periphery to allow complete extirpation of the obturator lymph node. After the removal of the obturator lymph node, dissection of the internal iliac lymph node begins and is carried out until the Alcock canal area to ensure completeness. A nervesparing approach is adopted in removing suspicious malignant lesions or malignant lateral lymph nodes. The extended lymphadenectomy is concluded with the en bloc removal of the tumor and lymph node specimen.5758
Postoperative outcomes
In contrast to Eastern countries, the gold standard in the West for treating pelvic lymph node metastasis involves preoperative CRT followed by TME. LPLND has not been recommended in Europe or North America because of increased complications without improvement in overall survival.54 Lack of evidence and paucity of data have contributed to the controversies about LPLN metastasis. In 2012, the JCOG0212 multicenter, randomized controlled non-inferiority trial was undertaken at 33 major hospitals in Japan. The trial aimed to compare postoperative morbidity and mortality after TME alone with TME with LPLND for stage II–III lower RC. Initial results revealed that TME with LPLND resulted in longer operating times (360 min vs. 254 min, p<0.0001) and greater blood loss (576 mL vs. 337 mL, p<0.0001) than TME alone. There was no significant difference in terms of grade 3 and 4 postoperative complications between the two groups (22% vs. 16%, respectively).59
Oncological outcomes
An update of the JCOG0212 trial has recently been published. There was no difference in terms of relapse-free survival (73.4% vs. 73.3%, p=0.0547), overall survival (92.6% vs. 90.2%), or local recurrence-free survival (87.7% vs. 82.3%) between the two groups. Nonetheless, the trial failed to confirm the non-inferiority of TME alone to TME with LPLND in the intention-to-treat analysis, with TME with LPLND showing lower rates of local recurrence than TME alone (7.4% vs. 12.6%, p=0.024).60
Functional outcomes
The JCOG0212 trial demonstrated that the oncological outcomes could be promising even in the absence of neoadjuvant CRT, which is the standard of care in Western countries. Moreover, the trial debunked previous concerns of an increased risk of urinary and sexual dysfunction after LPLND. According to the report on functional outcomes, the difference between the incidence of sexual dysfunction between patients who underwent LPLND and those who did not was not statistically significant (68% vs. 79%, p=0.37). On further analysis, age was found to be the sole risk factor independently associated with sexual dysfunction after the operation (p=0.02).61 Moreover, LPLND did not significantly affect urinary capability, with an intraoperative blood loss of >500 mL solely predictive of urinary dysfunction (relative risk 1.25, p=0.04).62
Summary
At present, variations in treatment algorithms exist, highlighting the dualism that pervades lateral lymph node management in RC. Ending the ongoing debates would necessitate randomized controlled multicenter studies; however, the lack of expertise in LPLND outside of Japan and the inherent treatment biases across the East and West continue to be persistent barriers.6364 After an extensive review of the literature, we concluded that the ideal approach would be to reconcile the competing tenets of the East and the West, effectively combining neoadjuvant CRT and LPLND. After all, LPLND seems to be beneficial in patients with a lateral pelvic node diameter >10 mm, representing a subgroup at high risk of lateral lymph node recurrence even after neoadjuvant CRT.65 MRI has been useful in determining lateral node metastasis, using a cutoff size of 6.0 mm in patients without CRT and 5.0 mm in patients with neoadjuvant treatment.66 As strides continue to be made in low RC treatment, there remains a pressing need for a more inclusive and cooperative approach to the lateral lymph node compartment, taking into account the merits of LPLND to improve future oncological results and resolve the remaining controversies.
NON-OPERATIVE MANAGEMENT IN DISTAL RC: EXPLORING A NEW TREATMENT PARADIGM
Introduction
The concept of non-operative management (NOM) or a “watch and wait” strategy in low RC has gained popularity in recent years, representing a departure from the conventional treatment paradigm that has long considered TME surgery its cornerstone. Notwithstanding the type of approach, radical surgery has been associated with functional consequences, significant morbidity, and need for stomas. Moreover, the avoidance of surgery has been shown to improve survival in older adults with RC and in those with comorbidities.2167
Patient selection
The observation that neoadjuvant CRT could induce significant tumor regression, with subsequent downstaging and downsizing of tumors, stimulated an interest in organ preservation strategies. Studies have documented that 15–30% of patients treated with neoadjuvant CRT develop complete pathologic response (pCR).68 Moreover, complete response of the tumor, termed complete clinical response (cCR), could be clinically evaluated in a subset of these patients. According to the proponents of the NOM approach, patients who exhibit cCR would be the ideal candidates for organ preservation and the most likely to benefit from it.69
Evaluation of tumor response
Since its introduction by Habr-Gama, et al.70 in 2004, different cohort studies have shown that a NOM approach can be employed in carefully selected patients without oncologic compromise; nonetheless, the lack of standardized parameters in identifying cCR after CRT continue to be persistent issues.707172 Evaluation of the tumor response is of paramount importance in considering patients for NOM. Clinical assessment using digital rectal examination (DRE) and endoscopy serve as essential tools in evaluating response. On DRE, cCR has been characterized by a smooth rectal wall and absence of irregularities, mass, or ulceration. On the other hand, on endoscopy, cCR has been defined as whitening of the mucosa, telangiectasia, and the absence of any residual mass, ulceration, or stenosis.71 Likewise, radiological evaluation has become essential in confirming cCR within the rectal wall and providing information not accessible with finger examination and endoscopy, such as disease dissemination to the mesorectum and regional nodes.21
Oncologic outcomes
The initial oncological results of patients who underwent NOM after achieving cCR following neoadjuvant CRT were reported to be equivalent to those of patients with pCR after surgery.70 Likewise, a recent meta-analysis comparing patients managed non-operatively after cCR versus patients with pCR after TME found no statistical difference between the two groups in terms of non-regrowth recurrence, disease-free survival, overall survival, and cancer-specific mortality.73 Indeed, these studies lend further credence to the notion that patients who achieve cCR after neoadjuvant treatment can be spared from the consequences of radical surgery without oncologic compromise.
Functional outcomes and QoL
The main argument in favor of a NOM approach has been its promise of improved functional results and QoL compared with TME, without compromising good oncological outcomes; however, studies about QoL in NOM have been limited. A case-matched controlled study by Hupkens, et al.74 comparing QoL between patients managed non-operatively and patients who underwent standard resection for RC has recently been published. Their results revealed that patients with NOM had better physical and emotional well-being, improved cognitive and physical function, and superior global health status than those who underwent TME. Moreover, patients with NOM exhibited fewer defecation, sexual, and urinary problems.74
Summary
At present, most of the evidence on the efficacy of NOM derives from non-comparative single-arm studies. A recent propensity-score-matched cohort analysis has demonstrated that a sizable proportion of patients managed non-operatively have avoided surgery and permanent colostomy without compromising oncological outcomes.75 In an age driven by evidence-based recommendations, randomized controlled data demonstrating oncological equivalence of NOM to radical surgery after the attainment of cCR following neoadjuvant CRT is still unavailable, necessitating future trials before NOM can be incorporated into practice as an alternative to radical surgery.
FUNCTIONAL OUTCOMES
Bowel dysfunction
Most of the patients who undergo SPS for low-lying RC develop LARS postoperatively. LARS after SPS can severely affect a patient's QoL. Up to 90% of patients who undergo rectal resection can have altered bowel function after SPS.76 The symptoms are diverse, including increased frequency of bowel movement, urgency, fecal incontinence, sense of incomplete emptying, and fragmentation. Anal sphincter damage during the operation, reduced neorectal compliance as a reservoir, altered motility of the neorectum possibly caused by denervation during deep pelvic dissection, and preoperative CRT are presumed to be the main causes of postoperative bowel dysfunction after SPS.77 Many investigators have used self-made questionnaires that have not been validated or assessment tools focused on specific symptoms, such as fecal incontinence. Among the validated assessment tools, the Memorial Sloan Kettering Cancer Center bowel function instrument (MSKCC BFI) and LARS score are the most widely used. The MSKCC BFI is a detailed tool and deals with a wide symptomatic spectrum of LARS; however, it is time consuming to use. On the other hand, the LARS score is a good and practical tool for the quick screening of bowel dysfunction.
In surgery for low-lying RC, patients are at a risk of parasympathetic nerve injury around the inferior mesenteric artery, and pelvic denervation from full mobilization of the rectum is inevitable owing to the low tumor level. Furthermore, the number of patients who receive neoadjuvant CRT has largely increased.
As multiple factors affect postoperative bowel dysfunction, all patients who are candidates for SPS should be counseled about the possibility of LARS, which might be severely detrimental to QoL, before surgery. They should be given the chance to weigh the burden of LARS against that of a permanent stoma.
Mahalingam, et al.78 reported the long-term functional outcome of 33 patients who underwent ISR. After a median of 45 months from restoration of bowel continuity, a mean number of bowel movements of <3 per 24 h was seen in 40% and 3–7 per 24 h in 50%. On the first 1 year after ISR, the patients showed major LARS and high Wexner score; however, bowel dysfunction usually improved after 1 year. They found that most patients had a satisfactory QoL after ISR, and good bowel function was correlated with good QoL.78
In a systematic review of outcomes after ISR by Martin, et al.,79 11–63% of patients complained of fecal soiling and 30–86% showed perfect continence. Although the assessment tools are inconsistent, the rates seem to vary across different studies.79
Reports on the functional outcome after taTME confined to patients with low RC are limited. Most studies included RC at all levels. Koedam, et al.32 reported postoperative bowel function after taTME in patients whose median tumor height was 6.0 cm from the anal verge [interquartile range (IQR) 4.0–8.0]. They found that the mean preoperative LARS score was 15.4 (95% CI 7.3–23.5). The score increased to 35.7 at 1 month, and then decreased to 21.7 at 6 months.32
The TaLaR trial and ETAP-GRECCAR 11 trial are multicenter randomized controlled trials aiming to compare the short- and long-term outcomes between TaTME and laparoscopic TME for low RC.8081 In these trials, the functional outcomes will be included among the secondary endpoints.8081
HLE has a concern of inevitable postoperative bowel dysfunction owing to unilateral excision of the levator muscle. In the preliminary report on 13 patients with low RC who underwent HLE with a postoperative follow-up duration of 11.0 months (IQR 8.5–27.0), the mean Wexner score after stoma closure was 9.4±5.7.41
The functional outcomes of NOM have not been fully investigated; however, the assumed benefit of NOM delays the morbidity and mortality and associated functional detriment of surgery. Maas, et al.82 reported the functional outcomes in their pilot study, in which the MSKCC and Wexner scores were assessed for 21 patients with NOM. Compared with patients who underwent surgery and showed pCR, patients with NOM showed higher MSKCC scores (better bowel function) and lower Wexner scores (lower fecal incontinence).82 Appelt, et al.83 reported that 72% of patients had no fecal incontinence at 1 year, and 69% at 2 years, among a total of 50 patients with NOM (total radiation dose of 66 Gy with concomitant chemotherapy of oral tegafur-uracil). Hupkens, et al.74 recently reported that patients with NOM showed better bowel function than did patients treated with CRT followed by TME, demonstrating lower rates of major LARS (one third in the NOM group vs. 66.7% in the CRT followed by TME group).
Urinary and sexual dysfunction
In terms of sexual and voiding functions, a number of studies have demonstrated the importance of pelvic autonomic nerve preservation and the effect of preoperative radiotherapy. A Dutch TME trial showed overall sexual dysfunction in 76% of male patients and 62% of female patients.84 Voiding dysfunctions, including urinary incontinence, retention, urgency, and incomplete voiding, are known to be less severe than sexual dysfunctions, and the incidence has been reported to be >30%.84 The most widely used validated assessment tools for urinary function are the International Prostate Symptom Score and Bristol female lower urinary tract symptom, and those for sexual function are the International Index of Erectile Function and Female Sexual Function Indices.
The most important point in preventing urinary and sexual dysfunction is to avoid injury to the autonomic nerves, including the superior and inferior hypogastric nerve plexus and neurovascular bundles going into genitourinary organs. Failure in bladder emptying is generally known to resolve within 3 months; however, symptoms persisting after 6 months are reported to be mostly permanent.85 Sexual dysfunction from partial injury of nerves is known to usually resolve within 3–6 months; however, delay in the treatment of sexual dysfunction might lead to permanent dysfunction.86
Solomon, et al.87 reported that there were significant discordance in decision-making, and their study showed that many patients with RC were willing to trade survival for QoL. With more diverse treatment options becoming available, not only oncologic outcomes but also functional outcomes should be taken into account when deciding treatment strategies. Therefore, patients should be informed about the functional aspects and be involved in the decision-making process.
CONCLUSION
As the incidence of colorectal cancer increases, colorectal surgeons should be cognizant of the issues extending beyond the performance of TME. APR and ISR are acceptable surgical procedures for treating low-lying RC; however, improvement of surgical skills is of paramount importance as novel techniques are being introduced. At present, a more cohesive approach that effectively combines LPLND and neoadjuvant CRT is needed to overturn the East and West dichotomy in the treatment of lateral lymph node metastasis. The evidence relative to NOM has demonstrated that the consequences of surgical treatment can be avoided, thereby challenging a treatment paradigm that has long considered surgery its cornerstone. With the increasing treatment options for low RC, QoL has become a major issue; thus, tailored treatment that takes into account both oncologic and anticipated functional outcomes is essential. In this regard, patient participation in the decision-making process is crucial, as this makes them aware of the potential impact of the treatment on their bowel, urinary, and sexual function.

 XML Download
XML Download