

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The incidence of cervical cancer varies between countries and is associated with the implementation of cervical cancer screening programs.1 In Korea, because of increased use of organized screening programs, the incidence of cervical cancer decreased during the period of 1999 to 2012; however, it is still the seventh most common cancer among women. In contrast, cervical cancer is still increasing in young and older adult patients.2 In 2015, an estimated 3100 patients were newly diagnosed with cervical cancer, and it was the third most common cancer in reproductive-aged women in Korea.234 Human papilloma virus (HPV) is an important oncogenic factor for cervical cancer. Persistent infection with high-risk (HR) HPV causes progression of precancerous lesions to invasive cancer.56
Among cervical cancer screening tests, the Papanicolaou test has contributed to a 75% decrease in the incidence of cervical cancer and reduced cervical cancer associated mortality.7 However, it has some limitations: 1) it has low sensitivity and reproducibility, 2) it has low coverage and poor patient compliance, and 3) its results are subjectively interpreted.89 Cotesting with the Papanicolaou and HPV tests is used to detect cervical cancer early according to the 2012 American Cancer Society screening guidelines.9
Currently, more than 100 HPV genotypes have been identified and classified according to their oncogenic potential as HR HPV (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 67, 68, 69, and 82), low-risk (LR) HPV (6, 11, 40, 42, 43, 44, 54, 55, 62, 70, 72, 81, 87, 90, and 91), and intermediate-risk HPV.610 Four HPV tests, Hybrid Capture 2 (HC2; Qiagen Inc., Valencia, CA, USA), cobas 4800 HPV (Roche, Pleasanton, CA, USA), Cervista HPV (Hologic Inc., Marlborough, MA, USA), and Aptima HPV (Hologic Inc., San Diego, CA, USA), have been approved by the US Food and Drug Administration.7101112
The cobas 4800 HPV test performs DNA extraction, PCR amplification, and real time detection in an automated fashion. It can distinguish HPV 16/18 from other HR HPVs.13 The HC2 test is a reliable, signal amplification hybridization assay. It can detect viral load and determine the presence of a clinically significant HPV infection. This assay detects 13 HR HPV genotypes; however, it cannot determine the genotype or distinguish between single and multiple infections.1415 The PANArray HPV test (PANArray™ HPV Genotyping Chip; Panagene Co., Seoul, Korea) uses PCR amplification of the HPV L1 gene that includes DNA bases for each genotype. This amplified PCR product is hybridized to each DNA probe for determination of HPV infection and genotypes. This assay can distinguish 19 HR HPV genotypes (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 69, 70, and 73) from 13 LR HPV genotypes (6, 11, 32, 34, 40, 42, 43, 44, 54, 55, 62, 81, and 83).
The aims of this study were to evaluate the performance of PANArray HPV test, a PCR-based DNA microarray assay, in detecting HPV infection in patients with atypical squamous cells of undetermined significance (ASCUS) cytology, in comparison to the cobas 4800 HPV and HC2 assays, and to assess any discordance between the assays.
MATERIALS AND METHODS
Patients and cervical samples
We reviewed medical records of study subjects, including cervical cytology and results of HPV tests. A total of 504 cervical swab specimens were collected from women with ASCUS cytology, between June 2012 and June 2014, from five hospitals (Seoul St. Mary's Hospital, Cheil General Hospital, Korea University Guro Hospital, Asan Medical Center, and Samsung Medical Center). This study protocol was approved by the Institutional Review Boards of each participating hospital (Seou St. Mary's hospital KC12DIMI0107, Cheil General Hospital CGH20120303, Korea University Guro Hospital KMC120017, Asan Medical Center AMC2012-0703, and Samsung Medical Center SMC12-0104). This study included patients aged 20–49 years with ASCUS cytology. We excluded patients with the following: 1) in pregnancy, 2) who had undergone cervical surgery, including conization, within the last year, and 3) who had undergone a hysterectomy. All specimens were collected with a cytobrush or cytobroom, and placed in ThinPrep PreservCyt solution (Hologic Inc., Marlborough, MA, USA).
Cobas 4800 HPV test
The cobas 4800 HPV test features fully automated sample preparation combined with real-time PCR technology and software that integrates the two components. The test is designed to extract, amplify, and detect a broad spectrum of HR HPV genotypes, as well as the human cellular globin gene. One-milliliter aliquots of PreservCyt fluid were transferred to 13-mL barcoded tubes provided by the manufacturer. The cobas 4800 HPV test was performed according to the manufacturer's protocol. DNA extraction was carried out using the automated cobas x 480 instrument, and real-time PCR amplification of HR HPV and β-globin DNA was performed using the cobas z 480 instrument. PCR amplification and detection occurred in a single tube, where 4 different reporter dyes track different targets (HPV 16; HPV 18; HPV 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68; and β-globin to provide a control for cell adequacy in the multiplex reaction).
HC2 test
Four milliliters of each PreservCyt specimen was tested by HC2 according to the manufacturer's protocol. We used a protocol for converting the liquid cytology sample to a specimen transport medium™ equivalent. The converted specimens were denatured at 65℃ for 45 minutes and hybridized under high-stringency conditions with a mixture of RNA probes that detect 13 different oncogenic HPV genotypes: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68. The resultant DNA-RNA hybrids were captured on the surface of the microtiter plate wells coated with anti-DNA-RNA hybrid antibody. The immobilized hybrids were then incubated with alkaline phosphatase-conjugated anti-hybrid monoclonal antibody, and the light intensity was measured with a luminometer. All specimens with a relative light unit/control (RLU/CO) ratio of ≥1.0 were considered positive. The RLU/CO ratio range of 1–10 was considered a gray zone.
PANArray HPV Genotyping Chip test and direct sequencing
For HPV DNA genotyping, the PANArray HPV Genotyping Chip was used according to the manufacturer's protocol. One PCR mix contained 5 µL of target DNA, 3 µL of PCR primer No. 1, and 17 µL of reaction mixture No. 1 supplied by the manufacturer (containing Taq DNA polymerase, PCR buffer, and deoxynucleoside triphosphate mixture) for a total volume of 25 µL. A second PCR mix contained 5 µL of the same target DNA, 3 µL of PCR primer No. 2, and 17 µL of reaction mixture No. 2. All tubes were incubated for 15 minutes at 94℃ before the PCR was started. A primary step consisting of 10 cycles of 30 seconds at 94℃, 30 seconds at 60℃, and 30 seconds at 72℃, followed by a second step consisting of 40 cycles of 30 seconds at 94℃, 1 minute at 47℃, and 30 seconds at 72℃. The PCR products were electrophoresed in a 2% agarose gel to confirm successful amplification of the PCR product. A mixture of hybridization buffer No. 1 and No. 2 (70 µL) was mixed with 5 µL of PCR product No. 1 and 5 µL of PCR product No. 2, and then applied to the PANArray chip and incubated for 1 hour at 50℃. After washing, array images were scanned and taken using a fluorescent scanner (GenePix 4000B; Axon Instruments, Union City, CA, USA). Clearly visualized double-positive spots for a specific HPV type were considered HPV-positive for that genotype. Samples negative in chip scanning but positive for the 150-bp HPV specific band using gel electrophoresis were interpreted as negative for 19 HR HPV and 13 LR HPV test types, but ‘HPV-other type’ positive. Lack of visualized spots and negativity for the 150-bp HPV-specific band using gel electrophoresis was considered ‘HPV’ negative. The samples that were interpreted as ‘HPV-other’ type positive in the PANArray HPV test were confirmed by direct sequencing. Direct sequencing was performed using a type specific HPV primer set that detects a wide range of HPV types. A total of 89 cases were analyzed by direct sequencing; of which 5 (7.6%) did not provide the type and two (3.0%) did not include HPV DNA.
Statistical analysis
The concordance rates (CRs) between results of the three HPV tests were evaluated using kappa coefficient (κ) with 95% confidence intervals (CI) by McNemar's test using SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA). Patients positive for single or multiple HR genotypes with or without LR HPV or ‘HPV-other’ type positivity were categorized as HR HPV-positive. Patients with samples negative for HPV 16/18 but positive for other HR HPV types with or without LR HPV or ‘HPV-other’ type positivity were categorized as non-16/18 HR HPV positive. Patients with samples positive for LR HPV or ‘HPV-other’ type, or those that were ‘HPV-negative’ were categorized as HR HPV-negative.
RESULTS
A total of 504 women were enrolled in the study. Their mean age was 38.5 years old, ranging from 20 to 49 years of age. Among the 504 patients, 230 (45.6%), 271 (53.8%), and 177 (35.1%) were positive for HR HPV in the cobas 4800 HPV, HC2, and Panagene PANArray tests, respectively. For HPV 16, 42 (8.3%) and 35 (6.9%) patients were positive in the cobas 4800 HPV and PANArray HPV tests, respectively. For HPV 18, 19 (3.8%) and 14 (2.8%) patients were positive in the cobas 4800 HPV and PANArray HPV tests, respectively. For non-16/18 HR HPV genotypes, 169 (33.5%) and 127 (25.2%) patients were positive in the cobas 4800 HPV and PANArray HPV tests, respectively. In the PANArray HPV test, 29 (5.8%) and 89 (17.65%) patients were LR HPV and ‘HPV other’ type positive, respectively. Among these patients, 12 (2.4%) were positive for 16 and other HR HPV infection in PANArray, two (0.4%) were positive for HPV 18 and other HR in PANArray. Twenty four (0.8%) were positive for other type HPV and LR HPV in PANArray, whereas 14 (2.8%) were positive for 16 and other HR in cobas 4800 HPV test and seven (1.4%) were positive for 18 and other HR HPV in cobas 4800 HPV test.
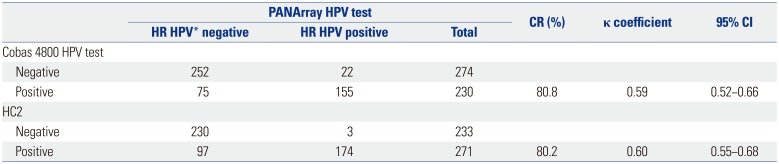
The CRs were 80.8% (κ=0.59, 95% CI, 0.52–0.66) between results of the cobas 4800 HPV and PANArray HPV tests and 80.2% (κ=0.6, 95% CI 0.55–0.68) between those of the HC2 and PANArray HPV tests for HR HPV genotypes (Table 1). For the detection of HPV 16, the CR between the results of cobas 4800 HPV and PANArray HPV tests was 98.2% (κ=0.87, 95% CI 0.79–0.96), while for the detection of HPV 18 the CR was 99.0% (κ=0.84, 95% CI 0.71–0.98) between these two assays (Table 2).
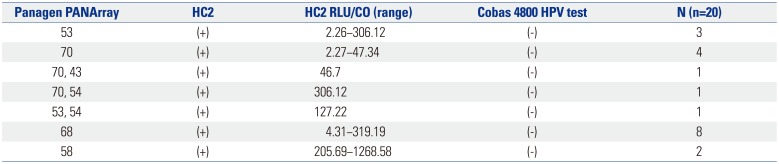
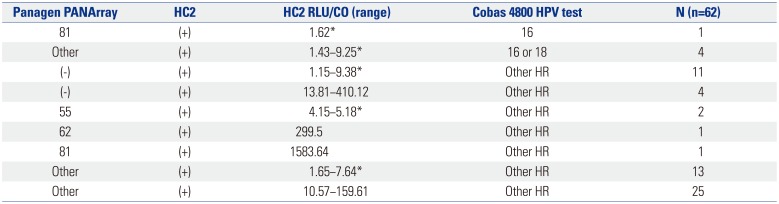
Twenty patients (4.0%) were negative in the cobas 4800 HPV test only. Of these patients, 10 (50%) were infected with HPV genotypes 43, 53, 54, and 70 by the PANAarray HPV test, which are not included in the cobas 4800 HPV test. Among the remaining 10 (50%) patients, eight were HPV 68-positive and two were HPV 58-positive by the PANArray HPV test (Table 3). One patient (0.2%) tested negative in the HC2 test only; this patient showed HPV 18 positivity in both the cobas 4800 HPV and Panagene PANArray tests. Sixty-two patients (12.3%) were negative in the PANArray HPV test, but positive in both the cobas 4800 HPV and HC2 tests. Of these patients, 42 (67.7%) showed positivity for ‘HPV-other’ type in the PANArray HPV test and 31 (50.0%) had results that fell within the gray zone (RLU/CO≤10) in the HC2 test. Patients negative for HR HPV only in the PANArray HPV test included 5 patients with HPV 16 or 18 positive results in the cobas 4800 HPV test; all of them were positive by HC2 but their results fell within the gray zone (RLU/CO ratio, 1.4–9.25) (Table 4).
Thirteen patients (2.6%) tested positive in the cobas 4800 HPV test only. Of these patients, three were HPV 16 positive, one was HPV 18 positive, and nine were non-16/18 HR HPV positive. Thirty-five patients (6.9%) were deemed positive only by HC2. Among them, 23 (65.7%) had results that fell within the gray zone (1–10 RLU/CO). Two patients (0.4%) tested positive in the PANArray HPV test; all these patients were infected with HPV 69, which is not detected by either the cobas 4800 HPV or the HC2 test.
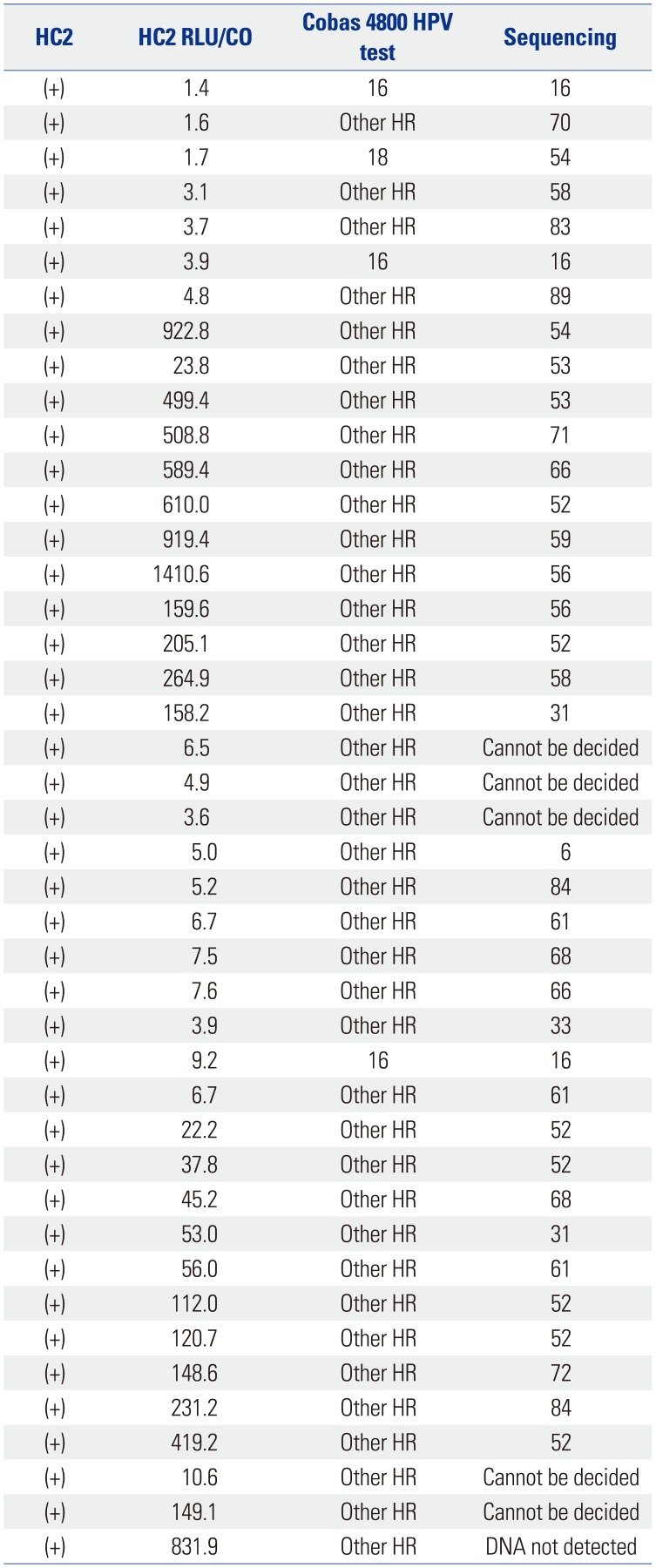
Eighty-nine samples showing other-type positivity in the PANArray HPV test were confirmed by direct sequencing. Three samples (3.4%) had no HPV DNA and seven samples (7.9%) did not provide definite results. Table 5 summarizes the results of direct sequencing which showed other-type positivity in PANArray HPV test, HC2, cobas 4800 HPV tests. In 43 samples (48.3%), HR HPV infection was confirmed by the HC2 and cobas 4800 HPV tests. Among them, genotype could not be decided six samples; eight were positive for genotypes 89, 71, 61, 84, and 72, for which the PANArray HPV cannot detect. Four samples were positive for LR HPV 6, 54, and 83. Twenty five samples were positive for HR HPV 16, 31, 33, 52, 53, 58, 59, 66, 68, and 70. Of these samples, eight (32%) fell within the gray zone (1–10 RLU/CO). All samples positive for HPV 16 by direct sequencing also showed HPV 16 in the cobas 4800 HPV test and were positive in the HC2 test. In addition, they had the gray results (1.7–9.2 RLU/CO).
DISCUSSION
Persistent infection with HR HPV is an important cause of the progression of precancerous lesions to invasive cancer. Compared to infection with non-16/18 HR HPVs, HPV 16/18 infection increases the risk of high-grade cervical lesions.1216 Accordingly, previous studies have focused on detecting HPV genotypes 16/18.7121417 However, non-16/18 HR HPV genotypes can be further categorized by risk stratification. According to HPV 9G DNA chip results, the odds ratios for worse than or equal to high grade squamous intraepithelial lesions (≥HSIL) of patients infected with HPV 16/18, HPV 31/33/35/45/52/58, and HPV 39/51/56/59/66/68, compared with HR HPV negative, were 18.1, 11.9, and 2.4, respectively.18
In the present study, the positivity rates of HR HPV infection in women with ASCUS cytology using cobas 4800 HPV, HC2, and PANArray HPV tests were 53.8%, 45.6%, and 35.1%, respectively. Overall, the positivity rate of the PANArray HPV test was lower than that of the cobas 4800 HPV and HC2 tests. However, the positivity rate for the detection of HPV 16 and 18 were similar between the cobas 4800 HPV and PANArray HPV tests (8.3% vs. 6.9% for HPV 16, 3.8% vs. 2.8% for HPV 18). Among healthy Korean women, the prevalences of HPV 16 and 18 have been reported as 4.5% and 1.8%, respectively.19 Moreover, among Korean women with ASCUS or low grade squamous intraepithelial lesion cytology, the prevalences of HPV 16 and 18 have been reported as 12.3% and 6.0%, respectively.6
The HPV DNA chip test is widely used in clinical practice and for research, especially in Asian countries. The reasons for this are as follows: 1) the HPV DNA chip and HC2 test have similar sensitivity and specificity for predicting ≥HSIL, and 2) it allows for genotyping. In previous studies, the CRs between the results of HPV DNA chip and DNA sequencing were reported to be 61.5–91.1%, which is probably due to different viral detection thresholds and cross reactivity.202122
The CR between the results of cobas 4800 HPV and PANArray HPV tests was 80.8%, while the CR between results of the HC2 and the PANArray HPV tests was 80.2% for HR HPVs, which is relatively high. When we analyzed the discrepant cases, 20 patients (4.0%) tested negative in the cobas 4800 HPV test only. Of these patients, 10 (50%) were infected with HPV genotypes 43, 53, 54, and 70 by the PANArray HPV test, which are not included in the cobas 4800 HPV or HC2 assays. Among the remaining 10 (50%) patients, eight tested as HPV 68-positive and two as HPV 58-positive by the PANArray HPV test, and nine were not within the gray zone (16-1265.6 RLU/CO) in HC2 (Table 3). One patient tested negative only in the HC2 test; this patient tested positive for HPV 18 in both the cobas 4800 HPV and PANArray HPV tests. With respect to the PANArray HPV results, the HR HPV positivity rate (35.1%) was lower than that of the cobas 4800 HPV (53.8%) or HC2 (45.6%) tests, and the LR HPV and ‘HPV-other type’ positivity rates were 5.8% and 17.65%, respectively. In PANArray HPV tests, positivity for ‘HPV-other type’ is indicated by no clearly visualized double-positive spots for 19 HR HPVs and 13 LR HPVs, but the presence of a 150-bp HPV specific band detected using gel electrophoresis. Among the 89 (17.65%) patients deemed ‘HPV-other type’ positive by PANArray HPV test, 62 patients (69.7%) tested as positive in both the cobas 4800 HPV and HC2 tests. This result suggests that the Panagene PANArray test might fail to detect a portion of HR HPVs during the hybridization process and that HPV-other type positive results in the PANArray HPV test should be carefully interpreted. Moreover, among these 89 (17.65%) HPV-other type positive patients, 31 (50.0%) had gray zone results (RLU/CO≤10) in the HC2 test. Patients who tested negative for HR HPV only in the PANArray HPV test included five patients who tested positive for HPV 16 or 18 infection in the cobas 4800 HPV test: all of them were positive by HC2, but the results fell within the gray zone (RLU/CO ratio, 1.4–9.25) (Table 4). This result suggests that the PANArray HPV test did not show consistent results in cases near the diagnostic threshold.
It has been reported that in the HC2 test, samples with weakly positive values (between 1.0 and 10.0 RLU/CO) do not show consistent results, especially near the diagnostic threshold.2223 Specifically, PreserveCyt samples, like those used in our study, require a pre-analytical manual conversion process in order to perform the HC2 and may test as pseudo positives since residual traces of undenatured DNA can generate results that fall within a gray zone with low (1–2.5) RLU/CO ratios.2425 The discrepancies in results might result from contaminations, which can occur: 1) during transfer of the samples to the microtiter plate after hybridization for subsequent hybrid capture, followed by agitation; 2) during inversion of the plate to empty the wells, and then reversion for addition of the detection reagent; or 3) during washing after addition of the detection reagent and before the addition of the reagent for signal generation.23 In the same context, our study showed that among 35 patients (6.9%) with positive results only by HC2, 23 (65.7%) had gray zone results (1–10 RLU/CO).
Of 89 patients who showed ‘HPV-other type’ positivity, 25 were positive for HR HPV in direct sequencing, the cobas 4800 HPV test, and the HC2 test (Table 5). According to the American Society for Colposcopy and Cervical Pathology guidelines, colposcopy is recommended for women with ASCUS cytology who are positive for HPV genotype and those with normal cytology who are positive for HPV16/18.26 For this reason, many clinicians do not consider patients with LR or othertype HPV infection as important. In our study, however, women who were other-type had HR HPV infection (38.2%) and high viral load.
The results of this study are subject to some limitations. First, since this study compared the results of the aforementioned three HPV tests, it could not provide data on the predictors of clinical outcomes. A second limitation is the small sample size used in the study. However, in the present study, we presented the CRs of the results of PANArray HPV test with two well-known HPV tests and demonstrated why ‘HPV-other type’ positive results should be carefully interpreted.
In conclusion, the CRs between the results of PANArray HPV test and both the cobas 4800 HPV and HC2 tests were relatively high, especially for the detection of HPV 16 and 18. The results deemed ‘HPV-other type’ positive by the PANArray HPV test, as well as HC2 gray zone results (RLU/CO ratio level 1–10), need careful interpretation using comprehensive clinical information. In these cases, short term follow up is mandatory, and HPV tests other than PANArray HPV test are recommended.

 XML Download
XML Download