

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Brain banks seek to obtain human brain tissue and to store it along with clinical and neuroimaging data. It is critical to obtain brain tissue for definitive diagnosis and to better understand neurodegenerative diseases. In Western countries, the importance of brain banks is well established, and various brain bank studies are underway. The Baltimore Longitudinal Study of Aging is the oldest cohort in the United States: collection began in 1958.1 Of 238 deaths, 211 were autopsied, confirming neurologic changes in neurodegenerative diseases, as well as normal aging.1 In the Rush Religious Orders Study, started in 1993, more than 1135 participants have been enrolled, and over 485 autopsies have been performed.2 Since the Rush Memory and Aging Project started in 1997, more than 1350 participants have been enrolled, and more than 650 autopsies have been conducted.2
In South Korea, due to the influence of Confucian culture, brain donation is a sensitive issue, and the establishment of brain banks has thus been limited, compared to other countries. However, there has been a recent change in awareness, with cremation becoming more common and more people understanding the importance of body donation. In addition to these social and cultural changes, the importance of obtaining brain tissue and establishing brain banks has been consistently presented. Therefore, we established the National Neuropathology Reference and Diagnostic Laboratories for Dementia (NRD) in South Korea in 2016. Through continuous efforts to collect brain tissue via donation, we have built a nationwide brain bank network, including Samsung Medical Center, Pusan National University, Kyungpook National University, Chonnam National University, Ajou University, Jeju National University, and Hallym University.
The NRD seeks to facilitate clinic-pathological correlation and image-pathological correlation analyses of neuropathological diseases and to broaden understanding thereof. In terms of clinicopathologic correlation, a discrepancy between clinical diagnosis and neuropathology has been found. In a community-based autopsy study, 25% of clinically diagnosed probable Alzheimer's disease (AD) cases had non-AD pathology.3 A high rate of additional neuropathological findings was also found, and only about 30% of the cases reflected pure AD on neuropathology.3 Accumulation of neuropathological data helps with understanding such discrepancies and furthermore contributes to accurate clinical diagnosis. It is also important to understand imaging-pathology correlations on various imaging techniques. As the development of new diagnostic agents is based on neuropathological studies, new diagnostic agents can only be accurately assessed through image-neuropathology correlation analyses. Advancement of therapeutic research has been based on a detailed understanding of disease pathogenesis in brain tissue. Therefore, diagnosis and treatment of disease are closely related to neuropathology.
In this study, we described the process of recruiting brain participants and their evaluation at Samsung Medical Center. Reporting our experience is worthwhile because other neuropathology centers can follow the same path and/or modify it to suit their own needs. We also presented distribution data for autopsy case diagnosis and participants of the brain bank.
MATERIALS AND METHODS
Participants and recruiting process
We recruited participants though two routes, from memory clinics and from the community. In clinics, all participants and their family, regardless of the severity of illness, were provided with a brochure on brain donation during outpatient visits and hospitalization. The doctor explained brain donation in detail, and the participants had time to discuss brain donation with their family members. The purpose of doctor counseling was 1) to communicate the importance of brain autopsy for clinical diagnosis and medical development; 2) to encourage participants to consider autopsy; and 3) to address misunderstanding and concerns about autopsy. The decision to allow autopsy was made voluntarily by the participants and their families, and there was no external pressure. If the decision was not made after the first counseling session, the doctor raised the question again after 6 months. If the participants and their family opted for an autopsy, they were provided with detailed information and instructions regarding what to do at the time of death, including contact information for the research coordinator, along with instructions to share this information with their family members or the person in charge.
For community-based recruitment, we collaborated with the Department of Anatomy, selected those who met inclusion criteria from the list of those who wanted to donate their body to the medical school, and sent them information by mail. The subjects were eligible for recruitment if they were aged over 70 years, lived in the Seoul, Gyeonggi, and Incheon areas, and agreed to donate their body in 2010–2016. We limited the duration of physical donation to a relatively recent period so that we could choose a person who was sure to donate. Donors were asked to participate in baseline and follow-up assessments, and their families were asked to have their body delivered to the hospital as soon as possible after death to facilitate timely autopsy. For that reason, we limited the residence area to Seoul and nearby areas, such as Gyeonggi and Incheon.
We sent mail to selected participants and included an explanation of the need for brain donations and the baseline assessment conducted. We tried to explain everything succinctly, but strongly emphasized the importance and necessity of brain donations, explaining that such donations can be useful for the study of neurodegenerative diseases, including dementia, and will benefit our descendants. We also emphasized that they could expect to monitor their own cognitive function during the study by briefly describing the baseline and follow-up tests that they would receive. Those who received the letter and expressed interest were contacted by phone, and we arranged a time to meet with each subject in the clinic. In the clinic, we provided detailed information about the study to each individual, after which they signed an informed consent form. This study was approved by the Institutional Review Board of Samsung Medical Center (SMC 2016-11-032-002).
Evaluation and follow-up
As a baseline evaluation, a structured clinical interview was undertaken, including assessment of the subjects' baseline cognitive function, past medical history, current medications, familial medical history, and social history, including education level, previous or present job, alcohol consumption, and smoking habits. A neurological examination was also done. After a detailed clinical interview, all participants underwent laboratory tests, including a complete blood count, blood chemistry, vitamin B12/folate levels, syphilis serology, and thyroid function tests. Every participant also underwent neuropsychological tests, MRI scan, and amyloid PET scan. Follow-up evaluations including clinical interviews and Mini-Mental Status Examination (MMSE) were planned every year. Detailed neuropsychological tests and MRI scans were planned every three years after the baseline evaluation.
Neuropsychological tests
All patients were followed annually using the Seoul Neuropsychological Screening Battery (SNSB).45 The battery contains tests for language, visuospatial function, verbal and visual memory, and frontal-executive function. Language was considered abnormal when the score on the Korean version of the Boston Naming Test (K-BNT)6 was below the 16th percentile of the norm. Visuospatial function was considered abnormal when the copying score on the Rey-Osterrieth Complex Figure Test (RCFT) was below the 16th percentile of the norm. Memory function was considered abnormal when the 20-min delayed recall score on the Seoul Verbal Learning Test (SVLT) or RCFT score was below the 16th percentile of the norm. Frontal-executive tests were classified into three groups: motor executive function (contrasting program, go/no-go, fistedge-palm, alternating hand movement, alternative square and triangle, and Luria loop), Controlled Oral Word Association Test (COWAT), and Stroop test. Abnormal frontal-executive function was operationally defined as impairment in at least two of the three groups. The norms for each of the above tests, based on the test results of 447 normal Korean participants, were used for comparison.
In this study, to assess verbal and visual memory functions, we analyzed the results from SVLT delayed recall (range 0 to 12) and RCFT delayed recall (range 0 to 36) tests, respectively. To assess frontal-executive function, we analyzed digit span backward (range 0 to 8), phonemic COWAT (range 0 to 45), and Stroop color reading test (range 0 to 112) scores. General cognition was assessed by clinical dementia rating sum of boxes (CDR-SOB, range 0 to 30). The Korean version of the MMSE (K-MMSE, range 0 to 30) was also administered.
MRI acquisition
Both structural and functional magnetic resonance images of all subjects were acquired on a Philips 3.0-T Intera Achieva MRI scanner (Philips Medical Systems, Best, the Netherlands). Whole-brain three-dimensional (3D) fast field echo T1-weighted structural imaging was acquired with the following scan parameters: 1-mm sagittal slice thickness, over-contiguous slices with 50% overlap, no gap, TR of 9.9 ms, TE of 4.6 ms, flip angle of 8°, and matrix size of 240×240 pixels. Images were reconstructed to 480×480 over a 240-mm field of view. All axial sections were acquired parallel to the anterior commissure-posterior commissure line.
Amyloid PET imaging acquisition and data analysis
Participants underwent florbetaben PET using a Discovery STe PET/CT scanner (General Electric Medical Systems, Milwaukee, WI, USA) or a Biograph mCT PET/CT scanner (Siemens Medical Solutions, Malvern, PA, USA) in a 3D scanning mode that examined 35 slices of 4.25-mm thickness spanning the entire brain. A bolus mean dose of 381 MBq was injected into an antecubital vein. Ninety minutes after injection, a 20-minute emission PET scan in a dynamic mode (consisting of 4×5 min frames) was performed. The florbetaben PET data were visually assessed by trained experts. Regional cortical tracer uptake (RCTU) (1=no uptake, 2=moderate uptake, 3=pronounced uptake) in the frontal, lateral temporal, posterior cingulate/precuneus, and parietal regions were assessed. Cases with an RCTU score of 1 in all four brain regions were classified as a brain amyloid plaque load (BAPL) score of 1, while cases with an RCTU score of 2 in any brain region and no regions with a score of 3 were classified as a BAPL score of 2. An RCTU score of 3 in any region was classified as a BAPL score of 3. Cases with a BAPL score of 1 were considered to be negative for amyloid, and those with a score of 2 or 3 were considered to be positive for amyloid.7
Autopsy
An autopsy was performed as soon as possible after patient death. Before the autopsy, we once again confirmed the legal guardian's consent to autopsy. We followed the guidelines for standardized operating procedures for brain autopsy, which was provided by the NRD.8 Brain autopsies were performed at Samsung Medical Center (n=9), Jeju National University Hospital (n=1), and Ilsong Institute of Life Science, Hallym University (n=1). The autopsy of the Creutzfeldt-Jakob disease (CJD) patient was undertaken at the Korea CJD Diagnostic Center (Ilsong Institute of Life Science, Hallym University).
Neuropathological assessments
Pathological assessments were performed using institution-specific protocols rendered at consensus conferences, as previously described.8 All autopsies included tissue sampling in regions relevant to the differential diagnosis of dementia based on published consensus criteria.91011121314 Tissue staining included some combination of hematoxylin/eosin, silver staining with modified Bielschowsky or Gallyas methods, and immunohistochemistry for Aβ, hyperphosphorylated tau, α-synuclein, ubiquitin, and transactive response DNA binding protein 43 (TDP-43). AD-related changes were assessed according to the Thal amyloid phase,15 Braak neurofibrillary tangle stage,16 and Consortium to Establish a Registry for Alzheimer's Disease (CERAD) plaque score.17 The overall severity of AD neuropathological change (ADNC) was assessed using the National Institute on Aging and Alzheimer Association (NIA-AA) criteria for AD.17 Archival cases assessed prior to release of the NIA-AA criteria were re-evaluated to confirm ADNC levels if additional staining was needed and feasible. When additional staining was needed but not feasible due to lack of available tissue, we reported the range of possible ADNC scores in light of the missing data.
ADNC levels were further dichotomized in two ways to allow us to compare groups using two different AD detection thresholds: 1) no ADNC versus low to high ADNC (low detection threshold) and 2) no to low ADNC versus intermediate to high ADNC (high detection threshold). Coexisting cerebral amyloid angiopathy, vascular brain injury, arteriosclerosis, atherosclerosis, argyrophilic grain disease, Lewy body disease, incidental TDP-43 proteinopathy, and hippocampal sclerosis were noted when present in available records.
RESULTS
Participants from memory clinics
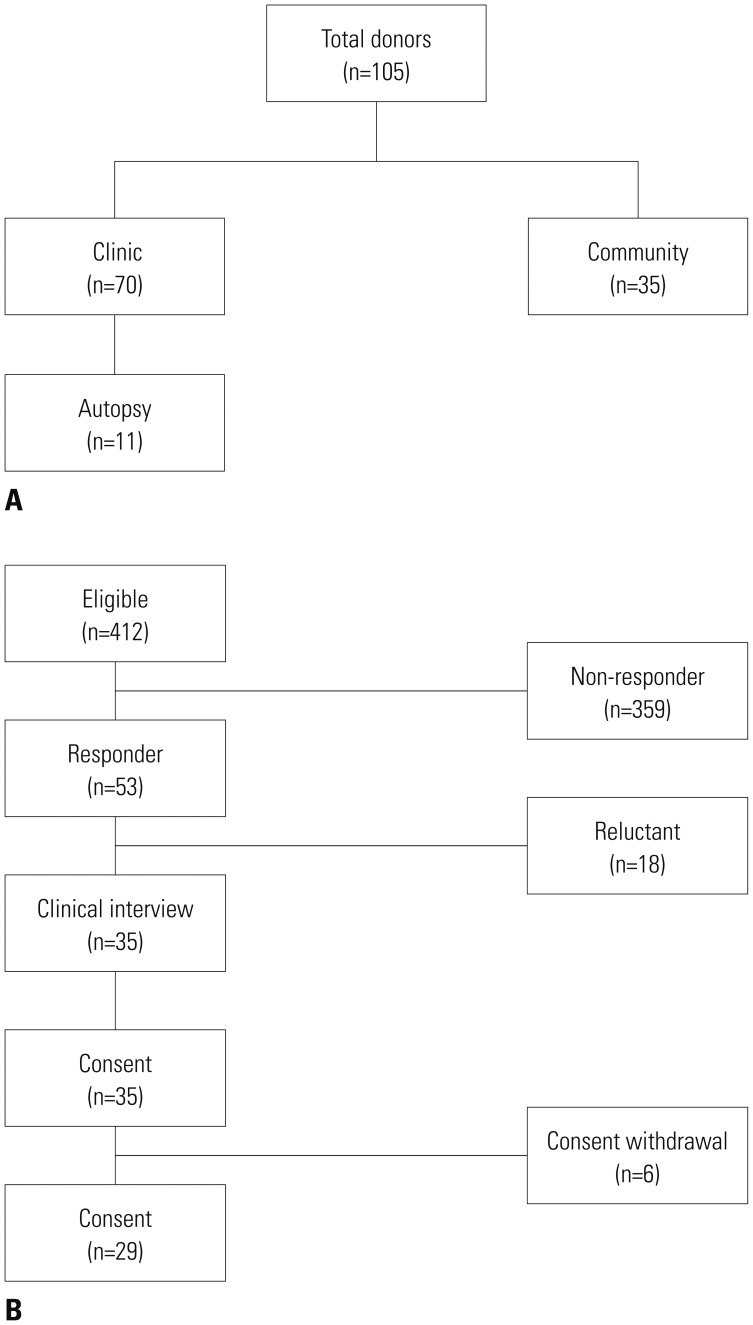
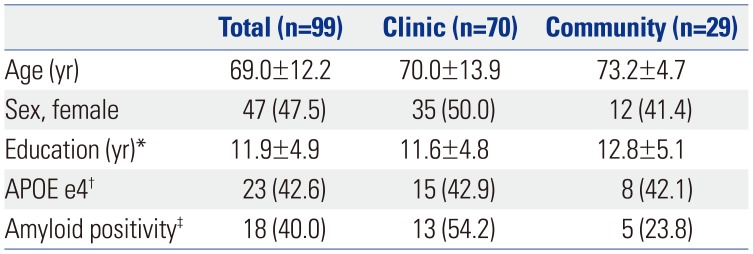
From the clinics, we recruited 70 participants for brain collection over 2 years. Of these patients, 75.7% contacted us after receiving counseling from a doctor, and 24.3% contacted us after they saw a poster or leaflet promoting the brain donation program. Among them, 11 participants died and underwent autopsy (Fig. 1A). The mean age of the participants from the memory clinics was 70.0 years (SD, 13.9 years) and 50.0% were female. The mean number of years of education for these participants was 11.6 years (SD, 4.8 years) (Table 1).
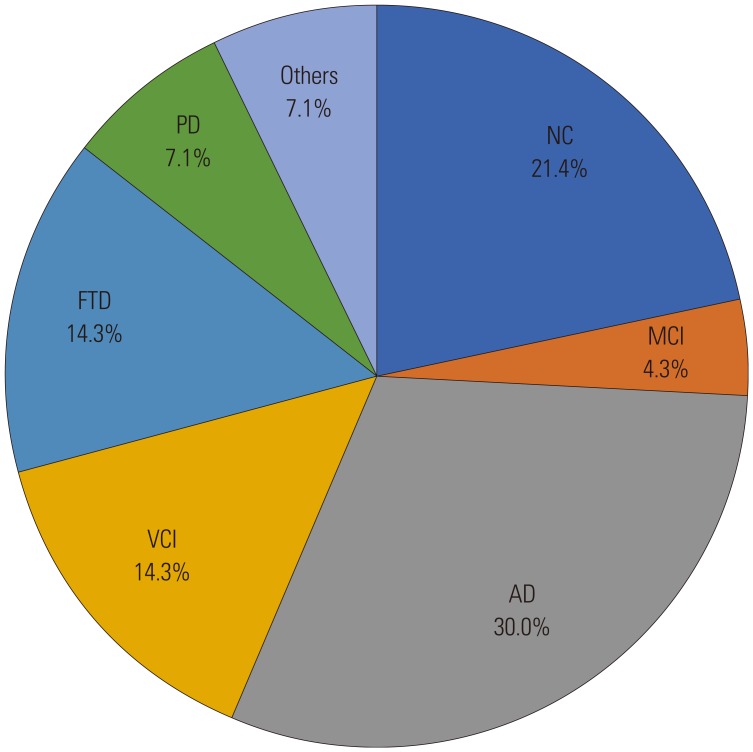
Diagnoses in these participants varied. There were 24 cases of Alzheimer's disease-related cognitive impairment (ADCI), which consisted of three cases of mild cognitive impairment (MCI), and 21 cases of AD; 10 cases of vascular cognitive impairment (VCI); 10 cases of frontotemporal dementia (FTD); four cases of idiopathic Parkinson's disease; one case of dementia with Lewy bodies; 15 cases of normal cognition; and six cases with diagnoses other than those listed above. Regarding the ‘other’ diagnoses, there was one patient with CJD, one patient with amyotrophic lateral sclerosis, two patients with leukoencephalopathy, and two patients with epilepsy (Fig. 2).
Participants from the community
Regarding community-based enrollment, among the 412 people contacted by mail, 53 people contacted us. Thirty-five agreed to donate their brains after death (Fig. 1B). The characteristics of our study participants are shown in Table 1. The mean age of the participants from the community was 73.2 years (SD, 4.7 years) and 41.4% were female. The mean number of years of education for these participants was 12.8 years (SD, 5.1 years).
Six of the 35 participants withdrew their consent. Of the remaining 29 participants, 20 underwent clinical interviews, 20 underwent neuropsychological tests, 19 took an apolipoprotein E (APOE) genotype test, 20 underwent MRI, and 20 underwent amyloid PET. None of them went undiagnosed or were treated at the clinic due to decline of cognitive function. Among the participants who underwent the neuropsychological tests, there were 10 (50.0%) with normal cognition, nine (45.0%) with MCI, and one with dementia. Eight of the 19 participants were APOE e4 carriers. The percentage of cases that were amyloid positive was 23.8% (Table 1). Among the participants who showed amyloid positivity, one was cognitively normal, three exhibited MCI, and one exhibited dementia.
Clinicopathologic correlations
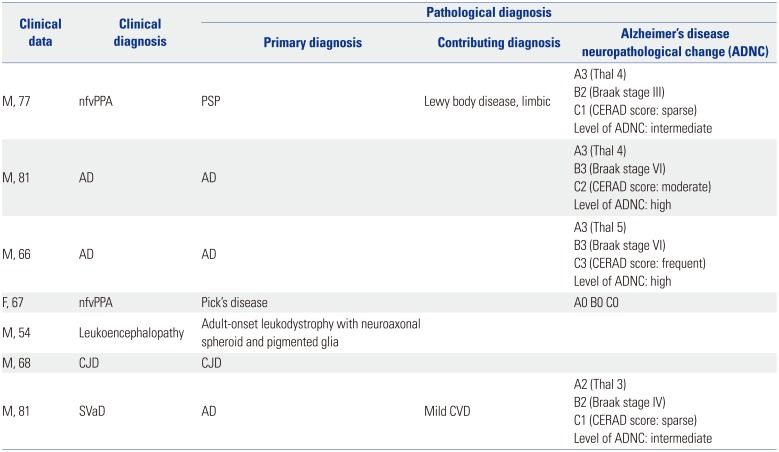
Eleven of the 99 participants died and were autopsied (Table 2). The average time to death after completing the consent form was 117 days. The clinical diagnosis of the patients who underwent autopsy was ADCI in four, VCI in two, nonfluent variant primary progressive aphasia (nfvPPA) in two, and HDLS, FTD, and CJD in one patient each.
Among the 11 patients who underwent autopsy, seven patients had their clinical diagnosis confirmed neuropathologically. Two clinically diagnosed AD patients were pathologically proven to have AD. Their ADNC levels were high. Among two clinically diagnosed nfvPPA patients, one was pathologically diagnosed with progressive supranuclear palsy (PSP) and Lewy body disease (limbic), while the other was pathologically diagnosed with Pick's disease. One clinically diagnosed small vascular dementia (SVaD) patient was pathologically diagnosed with mixed pathologies of AD and cerebrovascular disease (CVD). The clinically diagnosed HDLS case and CJD case were pathologically confirmed to be HDLS and CJD, respectively.
Imaging-pathologic correlations
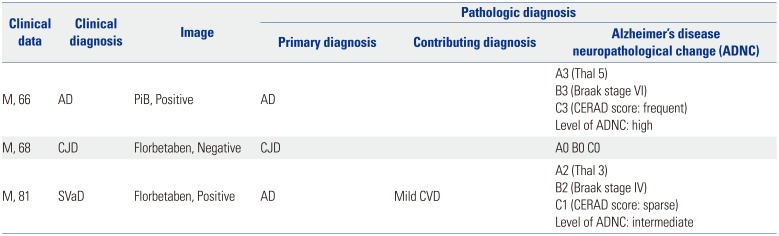
There were five patients who underwent amyloid PET during their lives: two with AD, one with mixed AD and vascular dementia (VaD), one with FTD, and one with CJD (Table 3). The mean interval from PET to autopsy was 34.9 months (range, 13.2–64.8 months). One case that exhibited amyloid uptake in diffuse regions showed a high CERAD score, while another case that had amyloid uptake in focal regions showed a moderate CERAD score. The CJD case, which was amyloid negative, showed a zero CERAD score.
DISCUSSION
We established the NRD in South Korea and recruited brain bank participants through two routes: from clinics and from the community. Participants from the clinic were composed mainly of individuals with ADCI, FTD, and SVCI individuals. Although participants from the community were not diagnosed with or treated at a clinic due to declining cognitive function, 45% showed abnormal cognitive function. Some clinical diagnoses, including AD, CJD, and leukoencephalopathy, were highly correlated with specific pathologies. Amyloid PET also predicted moderate to severe degree amyloid pathological burden. Therefore, future clinicopathologic or imaging-pathological correlation studies from this cohort will provide a deeper understanding of the pathobiology of dementia in Asia, especially South Korea.
In our cohort, the frequency of ADCI (34.3%) seemed to be lower than that in the Clinical Core of the Rush Alzheimer's Disease Center, which had a proportion of probable AD of 71.2% (n=280).2 Compared with other cohorts, the frequencies of VCI and FTD seemed to be higher in our study, although the total numbers of these patients were as relatively small. Our patient group comprised an SVCI cohort, and we previously investigated amyloid or tau PET uptake in SVCI patients using PET.18 About 30% of the SVCI patients showed amyloid positivity on PET, which was interpreted as a mixed pathology.18 They also showed higher prevalences of certain clinically significant factors, such as a faster deterioration and a worse prognosis.19 In particular, cerebral small vascular disease (CSVD) and AD pathologies interact.2021 Therefore, it is important to investigate the frequency of AD pathology in VaD and the correlation between CSVD and AD pathological burden on pathological examination.
FTD clinical syndromes include a behavioral variant and two subtypes of primary progressive aphasia.92223 Some patients with FTD also show motor neuron disease (MND), in which the syndromic diagnosis rendered is FTD-MND.10 In addition, PSP syndrome and corticobasal syndrome are often included in the FTD spectrum due to their prominent frontal cognitive and behavioral impairments.11 Collectively, these six clinical syndromes are united by overlapping clinical and anatomical features and their link to underlying frontotemporal lobar degeneration pathology.1223 Despite attempts to associate these FTD clinical syndromes with specific frontotemporal lobar degeneration neuropathological diagnoses, to date, no such correlation have proven invariant.2425 However, clinicopathologic correlation study is very important in cases of FTD syndrome. The wide variety of pathologies underlying the FTD clinical spectrum emphasizes the need for molecule-specific biomarkers that will improve antemortem disease prediction and the purity of future clinical trial cohorts.
We found that among the participants from the community, none of the patients had previously been diagnosed with cognitive impairment; however, only 50% were cognitively normal. The frequency of individuals with normal cognition in the community cohort was comparable to the frequencies of normal cognition from other community cohorts: 32.8% (n=63) in the Memory and Aging Project cohort and 32.1% (n=124) in the Rush Religious Orders Study cohort.2 Although we tried to obtain a better response rate by recruiting subjects who had already decided to donate their bodies, the response rate was lower than 10%. Among 412 eligible subjects, only 53 expressed their interest in donating their brain. The average number of years of education among those who agreed to donate was 12.8 years. Therefore, they were likely to have more medical knowledge, to understand the need for brain donation, and to have interest in maintaining their cognitive function. Also, 42.1% of the participants in the community group were APOE e4 carriers, and 23.8% of them were amyloid-positive on PET. Therefore, individuals who suffer from cognitive decline, either subjectively or objectively, were interested in maintaining healthy cognitive functioning and were willing to donate their brains. Among the 53 responders, 29 consented and 20 completed the evaluations. Some were reluctant to donate their brains because the whole brain would be kept after the donation process. Some did not want to register because they thought the process of consent and evaluation was too complicated. As brain donation can be a sensitive issue, it may be better to give information about the process through face-to-face interactions. It is thought that obtaining informed consent for brain donation at same the time the patient is consenting to donating their body is a way to ensure brain donation at a higher rate.
We also found that clinical and pathological diagnoses were well matched. Among the AD patients who underwent autopsy, two patients had confirmed AD pathology. According to previous studies, the autopsy results for patients with suspected AD could turn out to be pure AD. However, AD pathology also commonly coexists with other pathologies, including concomitant Lewy body disease, cerebrovascular disease, hippocampal sclerosis, argyrophilic grain disease, and TDP-43.14 There were two cases of nfvPPA: one exhibited PSP and Lewy body pathology (limbic), and one was confirmed to have Pick disease. Previous studies showed that approximately 45% of nfvPPA cases showed tau pathology, and 30% showed AD pathology.132627 A recent study suggested that tau pathology in nfvPPA is indicative of Picks, CBD, or PSP, and 66.7% of late-onset nfvPPA cases had Picks disease or PSP.24 Consistent with a previous study, our nfvPPA patients showed late-onset types (62 and 71).
In our cohort, amyloid uptake on PET was highly correlated with pathological amyloid burdens. Patients who were clinically diagnosed with AD and identified as positive on PiB PET were well correlated with autopsy results, which showed a high level of ADNC. In the case of SVaD patients with positive FBB PET results, autopsy revealed amyloid pathology; however, interestingly, these patients showed a relatively lower burden, compared to those with AD who were classified as Thal 3 and had a CERAD score of intermediate. Our findings were consistent with a previous study showing that the accuracy of PiB SUVR for cases of intermediate-to-high or high levels of ADNC was “good” or “excellent.”28
Although the number of participants enrolled at our center so far is small, this is an ongoing cohort that will be useful for comparing clinical diagnoses and patient data with post-mortem pathology. Participants underwent detailed baseline interviews with a neurologist, and changes in their cognitive functions and MRI data will be tracked until death. Furthermore, given that we collected amyloid and tau PET data, our cohort will be helpful for comparing in vivo amyloid pathology and post-mortem amyloid pathology. In order to maintain this cohort in the future, two important efforts must be made. First, participants should be continuously recruited through various methods. Second, registered individuals should undergo regular follow-up evaluations. In addition, we also have begun to recruit through public health facilities and are promoting donation through symposiums for local communities. Clinical and neuropathological information obtained from this cohort in the future will provide a deeper understanding of the neuropathological mechanisms underlying cognitive impairment in Asia, especially Korea.
 XML Download
XML Download