

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anthracofibrosis (AF) is a bronchoscopic finding and defined as bronchial narrowing with black pigmentation of the bronchial mucosa.1 In previous reports, AF was found to be common in elderly female patients who do not smoke.2 Although AF has rarely been reported in Western countries, it is common in Asian countries such as South Korea, Iran and India.123456
AF has several clinical significances. It can present as obstructive airway disease,234 and patients with chronic obstructive pulmonary disease (COPD) or asthma who do not respond to treatment often have undiagnosed AF.5 Additionally, AF is strongly associated with tuberculosis (TB).67 As the aforementioned countries are endemic areas of TB, AF is an important clinical problem in these populations.89
The “gold standard” for diagnosing AF is bronchoscopy.1 However, considering the fact that most AF patients are elderly people, performing bronchoscopy in all suspected patients is unrealistic; thus, more convenient and simpler methods for characterizing AF are needed. Today, computed tomography (CT) scans can be performed at a lower cost and with reduced hazards. Additionally, CT images are now commonly available for lung cancer screenings for many elderly patients. These CT scans enable the detection of characteristic radiologic features of AF.161011 Combining radiologic and clinical parameters could allow for the prediction of AF in high-risk patients. However, to date, there have been no studies aimed at developing a prediction model for AF. Moreover, previous studies on AF are limited and include only small numbers of patients. Therefore, we aimed to evaluate the clinical and radiological parameters for predicting AF and develop a prediction model to be used as a scoring system incorporating these clinical and radiological findings.
MATERIALS AND METHODS
Study design and patients
The study population was selected from a registry and included all patients who underwent bronchoscopies from January 1, 2008 to March 31, 2014, at Seoul Metropolitan Government-Seoul National University Boramae Medical Center Hospital in the Republic of Korea. AF was defined as a bronchial narrowing with multiple dark pigmentation of the bronchial mucosa. According to the presence of bronchoscopic AF, all patients were dichotomized into patients with AF (AF group) and patients without AF (controls). The enrollment criteria for the AF group were defined as patients older than 18 years with confirmed AF based on a bronchoscopy. We excluded patients presenting with simple pigmented spots without bronchial narrowing and patients with endobronchial lung cancer. The control criteria were defined as patients older than 18 years showing no endobronchial lesion on a bronchoscopic examination. Among subjects with no endobronchial lesion, we excluded those with missing data for bronchoscopic or radiologic variables. Fig. 1 shows the flowchart used in selecting the study population.
Common indications for bronchoscopy in the control candidates included possible TB (n=593, 42.7%), lung cancer (n=152, 10.9%), pneumonia (n=239, 17.2%), interstitial lung disease (n=49, 3.5%), atelectasis (n=32, 2.3%), hemoptysis (n=179, 12.9%), and others (n=146, 10.5%).
Indications for bronchoscopy in the AF group and controls included possible lung cancer (n=22, 13.2% vs. n=58, 24%), possible TB (n=63, 37.7% vs. n=0, 0%), pneumonia (n=30, 18.0% vs. n=107, 44.2%), interstitial lung disease (n=3, 1.8% vs. n=1, 0.4%), atelectasis (n=23, 13.8% vs. n=0, 0%), and others (n=26, 15.6% vs. n=76, 31.4%).
This study was conducted in accordance with the Declaration of Helsinki, and approved by the internal Institutional Review Board of Seoul National University Boramae Hospital (IRB No. 26-2015-7).
Clinical, bronchoscopic, and radiographic variables
The clinical characteristics, comorbidities, findings on the bronchoscopy and chest CTs were analyzed retrospectively. AF was confirmed and reviewed by two independent pulmonologists. The pulmonologist team consisted of three staff members and seven pulmonology fellows. The AF lesions were described as segmental or subsegmental divisions using a visual approach. The CT analysis included bronchial narrowing, atelectasis, peribronchial soft tissue infiltration or calcification, lymph node enlargement, and location and calcification of lymph nodes. All CT scans were reviewed retrospectively by a chest radiologist and a pulmonologist. The radiologist was unaware of the sites of the lesions and the bronchoscopy findings.
Statistical analyses
To compare cases and controls, we used the t-test or Wilcoxon rank-sum test for continuous variables and the χ2 test for categorical variables. Logistic regression modeling was used to find significant factors for predicting AF. Correlations between the variables (nominal scale) were analyzed by the phi coefficient. We assigned scores to predictors that were identified with the regression analysis, and the score was weighted in proportion to the exponential beta odds. The prediction score was then calculated for each patient by summing the weighted point scores. A receiver operating characteristic (ROC) curve was prepared using the weighted scores, and the area under the curve (AUC) for the new scoring system was calculated to evaluate the diagnostic ability in the two groups: patients with and without AF. A p value of <0.05 was considered to indicate a significant difference. To check the degree of overfitting of the prediction model, we used fivefold cross-validation. All statistical analyses were performed using the SPSS software (ver. 21.0 for Windows; SPSS Inc., Chicago, IL, USA) and MedCalc (ver. 14.12.0, MedCalc Software, Ostend, Belgium).
RESULTS
Baseline clinical and radiological characteristics
Among the 3214 patients who underwent bronchoscopies, 167 were enrolled as patients with AF and 242 were enrolled as controls from the 1390 patients with no endobronchial lesion (Fig. 1). All patients in this study were native to Korea. The demographic and clinical characteristics of patients with and without AF are summarized in Table 1. Females (67.7%) and non-smokers (88.6%) were predominant among patients with AF. As a comorbid disease, active TB was more common in patients with AF (38.3% vs. 10.3%). Additionally, asthma and heart disease were also more frequent in patients with AF. In clinical symptoms, cough and sputum were the most common in both groups. Among symptoms, dyspnea (n=38, 22.8%) was more common in the AF group, while chest pain, blood tinged sputum and fever were more common in the control group.
The anatomical distribution of AF in the bronchial tree is described in Table 2. The upper and middle bronchi are frequently involved by AF. The AF lesions tend to be present in multiple lobar bronchi (85.0%) or bilaterally (73.7%).
In Table 3, we summarize the radiological characteristics, including bronchial stenosis and wall thickening, atelectasis, peribronchial calcification, and pleural calcification. Additionally, we characterized the number, extent, and pattern of calcification of the mediastinal and peribronchial lymph nodes in detail, as well as their distribution. Except pleural calcification, all other bronchial findings were more commonly detected in the AF group. Reviewing the distribution of lymph nodes, lymph node enlargements were common in patients in the AF group (n=62, 37.1%), while only 38 patients (15.7%) showed lymph node enlargement in control group. With regard to the location, both subcarinal or lower paratracheal nodal enlargements were most common in both groups (Table 3). Calcified lymph nodes were observed in 61 patients (36.5%) with AF, much higher than only 9 patients (3.7%) without AF. Additionally, patients with calcified lymph nodes involving more than two sites were more common in the AF group. Calcified lymph nodes larger than 1.0 cm, focally calcified lymph nodes, and lymph nodes with the extent of calcification less than 50% were the most common findings in the AF group.
In addition, we evaluated clinical and radiological findings in endobronchial lung cancer confirmed by bronchoscopy. Among 3214 patients, we selected 1657 with endobronchial lung cancer and abnormal bronchoscopy findings. A total of 117 patients, aged 18 years or more, with visible endobronchial tumors were included in the endobronchial cancer group. All cases were histologically proven on the basis of bronchoscopic biopsy, and patients with coexisting AF were excluded. The differences between endobronchial lung cancer and AF are presented in Supplementary Table 1 (only online). Several factors correlated with the presence of AF, such as the following: older age, female gender, non-smoker status, active TB, multiple areas of involvement, bilateral involvement, stenosis, bronchial wall thickening, peribronchial calcification, lymph node enlargement, and lymph node calcification.
Predictive factors of AF
Using the logistic regression model, we found that the statistically significant variables associated with AF were age >70, gender, active TB, bronchial stenosis, bronchial wall thickening, atelectasis, and lymph node enlargement and lymph node calci-fication (Table 4). Based on the phi coefficient (φ coefficient from 0.07 to 0.69), only weak correlation was observed between the variables. The Hosmer-Lemeshow goodness-of-fit test statistic was 0.841, indicating good calibration of the model.
Results of the cross-validation
We performed a stratified fivefold cross-validation by dividing the sample into five subgroups. The mean AUC from the five-fold validation was 0.926 [95% confidence interval (CI)=0.896–0.949]. The AUC for the proposed model based on the total observations used to develop the model was 0.936 (95% CI=0.924–0.947), indicating a bias of 1%. Thus, the analysis did not show substantial overfitting of the prediction model. When we investigated the five models created during cross-validation, the predicting factors, including female gender, age >70 years, active TB, stenosis and lymph node calcification, occurred in all five models, while lymph node enlargement, bronchial wall thickening and atelectasis were observed in only three models.
Development of the AF risk score
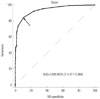
On the basis of results of the logistic regression analysis (Table 4), we assigned points to each of the AF predicting factors in proportion to the exponential beta odds of the variable, to calculate the risk score. As a result, points were assigned as follows: 1 point for female gender [β=1.34, odds ratio (OR)=3.83], lymph node enlargement (β=0.89, OR=2.43), atelectasis (β=0.87, OR=2.39) and bronchial wall thickening (β=1.43, OR=4.19); 2 points for TB (β=1.90, OR=6.69); 3 points for age >70 years (β=2.34, OR=10.37) and lymph node calcification (β=2.48, OR=11.90); and 13 points for stenosis (β=3.97, OR=53.10), resulting in 25 possible points. The scoring of each patient was determined by summing the weighted points for each predictor. A ROC curve was prepared using the total weighted scores. The diagnostic ability of the risk scoring model for detecting AF is shown in Table 5. Using the ROC curve, the optimal cutoff point in diagnosing AF was determined as 4 points. This cutoff represented an AUC of 0.939 (95% CI=0.911–0.960) (Fig. 2), which was similar to the AUC obtained from the internal validation using the fivefold validation method. The Youden index “J” was 0.741, and the cutoff value of >4 points showed a sensitivity of 84.43% and a specificity of 89.67% for diagnosing AF (Table 5).
DISCUSSION
In this study, we summarized the clinical and radiographic characteristics of AF and developed a simple and useful scoring system using clinical and radiographic findings such as gender, age, TB in clinical characteristics, and atelectasis, stenosis, bronchial wall thickening, enlarged lymph nodes and calcified lymph nodes. Score >4 points showed good predictive ability in detecting AF, by using only clinical and radiographic variables, which can be obtained readily in the clinic.
We developed the points-based scoring system and performed cross-validation to minimize substantial overfitting.12 Our prediction model showed good predictive performance and contained well recognized clinical and radiological factors. If our scoring model is appropriately validated in an external population, it can be a useful tool for detecting AF. In particular, given that most patients with AF are elderly, this score can be easily implemented due to its non-invasive nature.
The demographics of our AF population were similar to those of previous reports, and our model seems to similarly represent the characteristics of AF populations.813 In addition, we also described the distribution of AF and specified the location, size and the characteristics of calcification of the mediastinal and peribronchial lymph nodes in patients with AF. To our best knowledge, this is the most detailed reported description of lymph nodes associated with AF, although a number of previous studies have mentioned some radiographic characteristics of AF.111415
Another noticeable finding of our study is that patients with dyspnea and asthma were more frequently found in the AF group than in the control group. As well as TB, the long-term exposure to biomass smoke can result in the depositing of black pigmentation and is regarded as a major culprit in nonsmoking airway diseases.1617 Previous studies confirmed that the most common abnormal finding of the pulmonary function test in AF is an obstructive pattern.71819 No, et al.9 reported that 37% of AF patients showed evidence of airway diseases such as asthma or COPD, confirmed by other studies in respiratory function tests.202122 In clinical findings, according to the extent of stenosis, the symptoms of AF are variable and patients are usually treated with different methods depending on their presenting symptoms. Because dyspnea and wheezing are frequent symptoms of AF, it is often misdiagnosed as intractable asthma or COPD.823
Although bronchoscopy is the gold standard method for detecting AF, it is difficult to perform bronchoscopy in all suspected patients. Therefore, our prediction score can be helpful for detecting these AF patients at high risk in the clinical field. For example, diagnosis of AF can be aided by using this tool in specific patient groups, such as those with old age, a long history of wheezing, or non-responsiveness to inhaled therapy.
Because AF and bronchogenic cancer shares similar radiologic and clinical features, this model may not be suitable to distinguish AF from bronchogenic cancer. However, additional information can be used to facilitate differentiation of endobronchial lung cancer from AF. In our study, older age, female gender, TB, bilateral or multiple areas of involvement, bronchial wall thickening, bronchial wall calcification, lymph node enlargement, and calcification favored a diagnosis of AF. Another study also reported that bronchial wall stenosis with enlarged calcified lymph nodes was a useful marker to differentiate between the two.11
In our study, 64 patients (38.3%) in the AF group were confirmed by a culture test to have TB. As TB has been determined to be a possible causative factor of AF, it is no surprise that such a high prevalence of TB is seen in the AF group.11124
The important thing is the activities of TB. Even though no endobronchial TB (EBTB) findings were detected, there were still a large proportion of individuals with active TB in the AF group. A possible explanation may be that the anthracofibrotic lesions, which contain silicon, are vulnerable to TB infection, emphasizing the need for bronchial washing or further evaluation for detecting TB in AF patients.18
The radiologic and bronchoscopic findings can be explained in the same manner. Lymph node enlargement, lymph node calcification, stenosis, bronchial wall thickening and atelectasis in the AF group are found frequently in EBTB patients.1425
In addition, possible TB or atelectasis was the most common indication for bronchoscopic examination in the AF group.
Other studies suggest that the direct invasion of TB in the bronchial mucosa and implantation of acid-fast bacilli or drainage to the bronchus can cause granulomatous inflammation, which eventually results in bronchial fibrosis.2627
Additionally, upper and middle lobe predominance of AF can suggest a preferred site of TB. One hypothesis is that the right middle lobes adjacent to the lymph nodes and these lymph nodes may result in a narrower lumen compared to the other bronchi.9 However, the exact cause is still unknown, and further research is needed to determine whether the pre-existing AF lesion increases vulnerability to TB infection or if the post inflammatory stenosis is due to TB. Nonetheless, the possibility of active TB should be always considered in AF patients.
This study has several limitations. First, it was a single-center, retrospective design. Second, some significant variables may have been excluded from the model due to a posterior variable selection. Additionally, we used cross-validation to decrease overfitting. However, problems may arise from differences between patient populations, which can only be addressed by external validation in further studies. Another limitation is the absence of exposure history. Although we adopted “old age” and “female gender” as a predictive model, these variables can fluctuate because the risk of noxious exposure in old age or females tends to be cumulative over time and can be influenced by socio-environmental circumstances. Furthermore, even though the exposure history is necessary for broader applications, it was difficult to determine in our retrospective data setting. Therefore, we used available data including old age and female gender as indirect surrogate factors in predictive models.
We excluded bronchogenic cancer from the study cohort. In the clinical setting, discriminating bronchogenic cancer with or without atelectasis from AF is difficult. As validation of this model did not confirm the ability to distinguish lung cancer from AF, another prediction model may be required to detect bronchogenic lung cancer. In this study, we additionally evaluated clinical and radiological findings of endobronchial lung cancer to differentiate AF from lung cancer. Finally, the CT protocol differed from case to case. Despite these issues, we believe that an easily applicable, non-invasive model predicting AF will be beneficial in a clinical setting and a meaningful step in expanding research on AF and its related respiratory diseases. This can be promoted by further studies for external validation of our results.
In conclusion, AF is not rare disease in Asian countries and has significant clinical importance. We identified eight clinic-radiographic variables that are significantly associated with AF and developed a scoring system predicting AF. It is easily applicable and an accurate predictive tool for detecting AF without bronchoscopic examination in the study population.






 XML Download
XML Download