

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although radiofrequency catheter ablation (RFCA) for atrial fibrillation (AF) is an effective strategy for rhythm control, there remains a substantial recurrence rate.123 The majority of AF cases are triggered in patients with paroxysmal AF (PAF) derived from pulmonary veins (PVs), although 10-30% of PAF patients and the majority of patients with persistent AF (PeAF) have non-PV triggers.1456 Therefore, post-procedural detection and elimination of non-PV triggers might result in a better clinical outcome. Testing for immediate recurrence of AF after cardioversion is the common method for the detection of AF triggers.78 However, a post-procedural test for immediate recurrence of AF requires time, isoproterenol infusion,6 sedation, and electrical cardioversion. Moreover, repetitive electrical cardioversion may increase the risk of peri-procedural stroke in high-risk patients.9 Therefore, the clinical value of a post-procedural test for immediate recurrence of AF and additional ablation targeting remaining non-PV foci has not been clearly determined. With the development of a three-dimensional (3D)-electroanatomical software mapping system, the mapping and ablation of frequent atrial premature beats (APBs) has become relatively fast and accurate. Therefore, we hypothesized that non-PV-origin APBs may contribute to AF recurrence after catheter ablation. We defined the provocation of immediate recurrence of APBs (IRAPBs) as the detection of post-procedural frequent APBs (≥6 beats per minute) after electrical cardioversion under isoproterenol infusion (5 µg/min). The purposes of this study were to explore whether post-procedural IRAPB provocation and additional ablation for mappable frequent APBs affect the clinical outcome of AF ablation and whether IRAPB provocation lengthens procedure time or increases the complication rate. We also tested whether the type of induced tachyarrhythmias [AF or atrial tachycardia (AT)] and the presence of IRAPB are risk factors for clinical recurrence of AF after catheter ablation.
MATERIALS AND METHODS
Study population
The study protocol adhered to the Declaration of Helsinki and was approved by the Institutional Review Board of Yonsei University Health System. All patients provided written informed consent. This study was a single-center retrospective comparison study, and patients were matched 1:1 by age, sex, and AF type. The study included patients with AF (76.5% males; 57.4±11.1 years old) who underwent RFCA between March 2011 and December 2012. The exclusion criteria were as follows: 1) permanent AF refractory to electrical cardioversion; 2) AF with valvular disease (>grade II); 3) associated structural heart disease other than left ventricular hypertrophy; and 4) prior AF ablation. IRAPB provocation tests were conducted in 100 consecutive patients, who were compared with 100 age-, sex-, and AF-type-matched patients who completed ablation without any induction or mapping test (No-Test group) (Fig. 1). Among them, 67.0% of patients had PAF, and 33.0% had PeAF. 3D spiral computerized tomography (CT) scans (64 Channel, Light Speed Volume CT, Philips, Brilliance 63, the Netherlands) were performed to visually define atrial and PV anatomy in all patients. The presence of a left atrial (LA) thrombus was excluded by trans-esophageal echocardiography. All antiarrhythmic drugs were discontinued for a period corresponding to at least five half-lives. In total, 58 patients (29.0%) were taking amiodarone, which was discontinued for at least 4 weeks prior to the procedure. Anticoagulation therapy was maintained before catheter ablation.
Electrophysiologic mapping and radiofrequency catheter ablation
Intracardiac electrograms were recorded using the Prucka Cardio Lab™ electrophysiology system (General Electric Health Care System Inc., Milwaukee, WI, USA), and catheter ablation was performed in all patients using 3D electroanatomical mapping (St. Jude Medical Inc., Minnetonka, MN, USA) merged with 3D spiral CT. We used an open irrigated-tip catheter (Celsius, Johnson & Johnson Inc., Diamond Bar, CA, USA; Coolflex, St. Jude Medical Inc., Minnetonka, MN, USA; 30-35 W; 47℃) to deliver RF energy for ablation (Stockert generator, Biosense Webster Inc.; Diamond Bar, CA, USA). All patients initially underwent circumferential PV isolation and bi-directional block of the cavo-tricuspid isthmus. For patients with PeAF, we added the roof line, posterior inferior line, and anterior line10 as a standard lesion set. All procedures were conducted by two operators with over 10 years of experience.
Post-procedural protocol for IRAPB provocation
Fig. 1 summarizes the study protocol. After a standard procedure, AF or AT was induced by 10-second high-current burst pacing (10 mA, pulse width 5 ms, Bloom Associates, Denver, CO, USA) from the high right atrial (RA) electrodes. This commenced at a pacing cycle length of 250 ms and was gradually reduced to 120 ms as previously described (Fig. 2A).11 We initiated isoproterenol (5 µg/min) infusion for at least 3 minutes before induction and maintained this for 3 minutes after the induction of AF or AT. Then, internal cardioversion was performed by utilizing biphasic shock (2-15 J) with R wave synchronization (Lifepak12, Physiocontrol Ltd., Redmond, WA, USA) using an anodal decapolar catheter (WOVEN diagnostic catheter, Bard Electrophysiology, Lowell, MA, USA) in the RA and a cathodal duo-decapolar catheter (St. Jude Medical Inc., Minnetonka, MN, USA) in the coronary sinus (CS) (Fig. 2B). After successful electrical cardioversion, we stopped isoproterenol infusion and waited for 10 minutes to map IRAPBs or immediate recurrence of AF originating from the non-PV foci (Fig. 2C). All mappable IRAPBs (≥6/min) or APBs triggering AF were mapped and ablated during the waiting period in the IRAPB provocation group. If AF recurred immediately (8 of 100) or during the mapping of IRAPBs (5 of 100) after cardioversion, we repeated internal cardioversion and attempted to ablate all mappable frequent IRAPBs.
Post-ablation follow-up
Patients were discharged without any anti-arrhythmic drugs and asked to visit the outpatient clinic at 1, 3, 6, and 12 months after RFCA and every 6 months thereafter for follow-up. Electrocardiography (ECG) was performed at each visit or anytime the patient reported palpitations. A Holter ECG (24-hour or 48-hour) and/or event recorder was evaluated at 3, 6, and 12 months after RFCA and every 6 months thereafter for at least 2 years, according to the 2012 HRS/EHRA/ECAS Expert Consensus Statement guidelines.12 We defined recurrence of AF as any episode of AF or AT with a duration of at least 30 sec.13 If any ECG documented an AF episode within the 3-month blanking period during follow-up, the patient was diagnosed with an early recurrence. Any AF recurrence thereafter was diagnosed as clinical recurrence,13 and antiarrhythmic medications were prescribed.
Data analyses
We compared clinical and electroanatomical markers in patients who experienced recurrence of AF with those in patients who remained in sinus rhythm. Data are expressed as mean±standard deviation. Statistical significance of the comparisons was assessed using Student's t-test, Fisher's exact test, and Kaplan-Meier analysis. A p-value of <0.05 was considered statistically significant.
RESULTS
Mapping and ablation of post-procedural IRAPBs
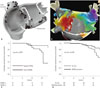
Fig. 1 summarizes the study protocol. Among the 100 patients in the IRAPB provocation group (70 PAF, 30 PeAF), we mapped and ablated IRAPBs in 33 patients, and 67 did not show post-procedural IRAPB after stopping the isoproterenol infusion (Table 1). The patients who tested positive for IRAPB had a higher CHADS2 score (p=0.003), higher prevalence of previous stroke/transient ischemic attack (p=0.002), higher frequency of sinus node dysfunction (p=0.025), and a larger left atrial volume index (LAVI; p<0.001) than those who did not. Fig. 3A shows the 44 sites for IRAPBs and additional ablation in 33 patients with positive IRAPB, with locations as follows: superior vena cava (n=12), interatrial septum (n=11), CS ostium (n=10), ligament of Marshall (n=6), crista terminalis (n=3), and LA posterior wall (n=2, one PAF and one PeAF). The RA volume index of the patients with RA-origin IRAPB (21.1±5.6 mL/m2) tended to be greater than those with LA origin IRAPB (19.5±4.6 mL/m2) without statistical significance (p=0.462). In patients with frequent and uni-focal IRAPBs, 3D-electroanatomical mapping was utilized for accurate mapping of non-PV foci or recovered conduction at linear ablation sites (Fig. 3B). The patients who underwent IRAPB ablation required a significantly longer procedure time (p=0.001) and ablation time (p=0.038) than those without IRAPB (Table 1). However, additional ablation for IRAPBs did not increase the procedure-related complication rate (p=0.732).
Presence of post-procedural IRAPBs is associated with higher clinical recurrence rate
During 18.0±6.6 months of follow-up, the early recurrence rate and clinical recurrence rate were 19% and 15%, respectively, for the IRAPB-provocation group. Among 51 patients with positive post-procedural inducibility before isoproterenol infusion, there was no significant difference in recurrence rates with respect to the type of induced atrial tachyarrhythmias (AF vs. AT; p=0.694) (Table 2). However, the patients with positive IRAPB showed a significantly higher early recurrence rate (36.4% vs. 10.4%; p=0.002) and clinical recurrence rate (27.3% vs. 9.0%; p=0.016) than those with negative IRAPBs, despite additional ablation and a longer procedure time (p=0.001) (Table 1). On multivariate logistic regression analysis, IRAPB (β=1.398; odds ratio=4.046; 95% confidence interval 1.14-14.39; p=0.031) was independently associated with clinical recurrence after RFCA of AF (Table 3). Table 3 also shows that the type of induced atrial tachyarrhythmias, AT (p=0.308) or AF (p=0.422), was not associated with clinical recurrence. Kaplan-Meier analysis showed consistently worse clinical outcome in patients with positive IRAPBs after the procedure (log rank, p=0.007) (Fig. 3C).
IRAPB provocation and ablation results in better clinical outcome of AF ablation
We compared patient characteristics, procedure time, procedure-related complication rate, and clinical outcome between the patients with IRAPB provocation and age-, sex-, and AF-type-matched patients who completed the procedure without an induction test (No-Test group) (Table 4). The baseline characteristics, LA diameter (p=0.187), LAVI (p=0.105), procedure times (p=0.540), ablation times (p=0.848), and procedure-related complication rates (p=0.702), were not significantly different between the two groups. However, the clinical recurrence rate (15.0% vs. 28.0%; p=0.025) was significantly lower in the IRAPB provocation and ablation group than in the No-Test group. Ka-plan-Meier AF-free survival analysis indicated a consistently better clinical outcome in the IRAPB provocation group than in the No-Test group (log rank, p=0.038) (Fig. 3D).
DISCUSSION
In the current study, we reported the potential usefulness of post-procedural IRAPB provocation and additional ablation during AF catheter ablation. The patients who showed post-procedural IRAPB under isoproterenol had a clearly higher clinical recurrence rate of AF than those without IRAPB. However, clinical outcome was better in patients with routine post-procedural IRAPB provocation and additional ablation than in those who completed the procedure without an induction test. This study revealed the importance of remaining non-PV foci as a mechanism of recurrence after AF catheter ablation. Therefore, a further prospective study with a larger number of patients is warranted to prove whether routine IRAPB provocation facilitates an improved clinical outcome of AF catheter ablation.
Role of post-procedural detection of AF triggers or substrate
AF is generally a progressive disease, and the mechanism for generation of AF is not yet fully understood.114 Coumel1516 suggested that trigger factors or trigger foci initiate AF, and arrhythmic substrate leads to its persistence. In this study, we explored the clinical significance of post-procedural tests for AF triggers or IRAPB. It is known that 70-90% of AF triggers exist around PVs in patients with PAF; however, non-PV foci are more common in those with PeAF.456 Generally, PV isolation at the level of the PV antrum is a cornerstone of catheter ablation for AF.171819 In this study, by isolating PVs during the procedure, all post-procedural IRAPBs arose from non-PV foci. Although the presence of IRAPBs from these non-PV foci clearly worsened the clinical outcome of AF ablation, additional ablation targeting IRAPB might result in a lower recurrence rate than that of the No-Test group. Therefore, remaining non-PV-origin IRAPB may play an important role in the recurrence mechanism of AF in the No-Test group.
Clinical significance of non-PV foci
APBs that trigger AF frequently arise from PVs,20 and cardiac autonomic nerves mainly connect to the heart along the PV antral area.42122 Therefore, bi-antral PV isolation is effective for the elimination of PV triggers,2324 cardiac autonomic denervation,25 and substrate modification. However, PV isolation may not be sufficient to control AF due to the presence of non-PV foci or atrial substrate remodeling, particularly in patients with PeAF.2627 Clinically, complex fractionated atrial electrograms (CFAEs) are known to play a role in maintaining AF2829 and act as a target for AF catheter ablation.2930 Verma, et al.31 considered CFAE ablation to be a non-PV substrate and a trigger of ablation, and Lemery, et al.32 co-localized the area of CFAE and cardiac autonomic ganglionated plexi by nerve stimulation. However, CFAE includes both the active driver of AF and passive wave breakers, and CFAE-guided AF ablation carries the risk of unnecessary cardiac tissue damage. In this study, we ablated non-PV foci targeting post-cardioversion IRAPBs and demonstrated a better clinical outcome.
Mapping and ablation technique for non-PV foci
We previously reported that an excessively long ablation dura-tion for substrate modification results in a poor clinical outcome.3334 Therefore, limited and sophisticated ablation for non-PV foci based on post-procedural IRAPB might be beneficial for a better clinical outcome. However, detection and ablation of non-PV foci are not simple. We targeted non-PV foci immediately after cardioversion under isoproterenol (5 µg/min) infusion. As we adhered to the linear ablation strategy, including the anterior line10 in patients with PeAF, re-initiation of AF was uncommon (8%) after cardioversion and cessation of isoproterenol infusion, and most non-PV foci remained as frequent APBs. We were able to map those non-PV IRAPBs based on the areas defined by linear ablation lines.11 Quick and limited 3D activation mapping utilizing a multi-electrode catheter was useful for accurate mapping and limited ablation of frequent non-PV-origin APBs in certain patients. We mapped and ablated IRAPBs during the isoproterenol cooling-down period until no APBs appeared.
Limitations
The patients included in this study were a highly selective group referred for RFCA, and the number of patients was limited. As this was a retrospective single-center study, there might have been a selection bias, despite comparing two groups matched for age, sex, and AF type. Considering that most IRAPBs were mapped and ablated within 10 minutes after stopping isoproterenol infusion, infrequent IRAPBs, multi-focal APBs, and catecholamine-insensitive APBs may not have been eliminated in this study protocol. In addition, we did not challenge isoproterenol again after IRAPB ablation.
Conclusion
The patients who showed post-procedural IRAPB under isoproterenol had a clearly higher clinical recurrence rate of AF. However, careful mapping and ablation for post-procedural IRAPB safely resulted in a better clinical outcome without requiring a longer procedure time compared to those who completed the procedure without an induction test. Therefore, a future prospective study with a larger number of patients is warranted to determine whether routine IRAPB provocation facilitates an improved clinical outcome of AF catheter ablation.






 XML Download
XML Download