

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Interbody fusion strategies continue to evolve, improving surgical success rates and reducing morbidity. Open approaches, such as anterior lumbar interbody fusion (ALIF), posterior lumbar interbody fusion (PLIF), and transforaminal lumbar interbody fusion (TLIF), reportedly show high rates of success,1,2,3 although intraoperative concerns and iatrogenic complications are known.4,5,6
The minimally invasive lateral transpsoas approach to the lumbar spine is also known as extreme lateral interbody fusion (XLIF) or direct lateral interbody fusion (DLIF). The method was first described in 2001.7,8 The advantages of XLIF or DLIF include minimally invasive access to the lumbar spine, less blood loss compared with open surgery, decreased operative times, shorter hospital stays, and less postoperative pain.7 XLIF or DLIF are novel in that they can be used to gain access to the lumbar spine via a lateral approach that passes through the retroperitoneal fat and psoas major muscle. However, several complications have been reported. The most common complication is nerve injury: it has been reported that 30% of patients show paresthesias in the leg and 27% of patients show thigh pain after DLIF surgery.9 Furthermore, high rates (62.7%) of transient anterior thigh symptoms are found despite real-time electromyography (EMG) monitoring.10
To avoid nerve injury, mini-open anterior retroperitoneal lumbar interbody fusion methods, such as oblique lateral interbody fusion (OLIF), have been applied, as reported in 2012.11 With this method, a 4-cm skin incision is made 6-10 cm anterior from the mid portion of an intervertebral disc; the retroperitoneal space is accessed by blunt dissection; and the peritoneal content is mobilized anteriorly. The psoas muscle is then identified and reclined posteriorly, revealing the intervertebral disc. A banana-shaped polyetheretherketone cage (Boomerang, Medtronic, Minneapolis, MN, USA) filled with a bone graft was used in the reported study.11 A total of 179 patients undergoing OLIF showed good results with minimal blood loss and short operation time, as well as a decreased risk of abdominal wall weakness or herniation.11 Subsequent to this report, Medtronic improved and developed their OLIF system (OLIF25) and cage (Clydesdale Spinal System, Medtronic, Minneapolis, MN, USA), and this procedure enables placement of a larger interbody graft into the disc space for anterior column support and segmental sagittal alignment, while minimizing the nerve, muscle, and bone obstacles associated with traditional direct lateral approaches. However, to our knowledge, results and complications of this OLIF surgery have not been reported.
In the current study, we aimed to examine the clinical efficacy of OLIF for lumbar spinal degeneration disorders and to ascertain any complications during surgery.
MATERIALS AND METHODS
Patients and surgery
We evaluated 35 patients at our university hospital between June 2012 and February 2012. Patients were diagnosed with lumbar degeneration spondylolisthesis and spinal stenosis, degenerated kyphoscoliosis, and discogenic low back pain on X-ray and magnetic resonance imaging (MRI), myelography, and computed tomography after myelography (CTM). Patients who had previously undergone spinal surgery were included. We excluded spinal tumor, infection, and acute vertebral fractures of the thoracic and lumbar spine. Diagnosis of spondylolisthesis and inclusion criteria for fusion surgery were 1) more than 10% slip of the vertebra in a neutral position or 2) more than 5 mm of translation between flexion and extension positions on radiographic evaluation. Diagnosis of discogenic low back pain was determined by pain provocation by discography and pain relief after discoblock using lidocaine. When pain was provoked during the discography and decreased after the discoblock, we confirmed a diagnosis of discogenic low back pain. For diagnosis of degenerated kyphoscoliosis and indication for surgery, both more than a 40° Cobb's angle on the coronal plane and less than 10° of lordosis on the sagittal plane of the lumbar spine were used as inclusion criteria. Informed consent was obtained from each of the participants. Bone mineral density (BMD) of the lumbar spine was examined before surgery. Details of the patients' backgrounds are shown in Table 1.
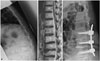
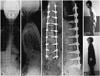
All patients initially underwent OLIF (Medtronic OLIF25) surgery. A cage (Clydesdale Spinal System, Medtronic, Minneapolis, MN, USA) filled with bone graft from the iliac bone was used in this study. Subsequently, posterior fixation was utilized in all patients. Open pedicle screws, percutaneous pedicle screws, or cortical bone trajectory screws (Medtronic) were used in all patients. Some patients underwent posterior decompression, while others did not. OLIF fusion from 1 to 4 levels and posterior fusion from 1 to 8 levels was performed (Figs. 1 and 2).
Assessment for posterior decompression
We performed myelography immediately after OLIF (before posterior fixation). If the lateral view showed a canal stenosis of more than 50% of a normal adjacent level, we performed posterior decompression. If the canal stenosis was less than 50% of a normal adjacent level, we did not perform posterior decompression. Open laminotomy at the level of the OLIF was used for decompression.
Radiographic and clinical evaluation
Radiography was used for evaluation before and after surgery. Anterior-posterior and profile views of X-ray images before and after surgery (immediate after surgery, one month after surgery, and at final follow-up) were evaluated.
We evaluated changes in low back and leg pain before and after surgery using a visual analogue scale (VAS) score (0, no pain; 10, worst pain). The Oswestry Disability Index (ODI) for low back pain was recorded before, 1 month, and 6 months after surgery.
RESULTS
Table 1 lists the demographic characteristics of the patients before surgery. Diagnoses included spondylolisthesis (20 patients), kyphoscoliosis (11 patients), and discogenic pain (4 patients). Diabetes mellitus in 6 patients, Parkinson disease in 3 patients, revision surgery in 6 patients (prior posterior surgery), and hemodialysis in 1 patient were recorded. The OLIF procedure was performed from 1 to 4 levels for a total of 45 levels in 35 patients. Open pedicle screws (8 patients), percutaneous pedicle screws (22 patients), or cortical bone trajectory screws (5 patients) were used for posterior fixation. Posterior decompression was performed in 18 of the 35 patients.
Adverse events
There was no infection, major vessel injury, peritoneal injury, or urinary injury. Segmental artery injury occurred in 1 patient and the surgery was converted to open surgery. Hardware failure did not occur; however, cage subsidence at one level was observed in one osteoporotic kyphoscoliosis patient. Spinal nerve injury did not occur. Quadriceps weakness in 1 patient, thigh pain in 1 patient, and thigh numbness in 3 patients were observed. Quadriceps weakness, thigh pain, and numbness diminished within 2 weeks of surgery (Table 3).
DISCUSSION
In the current study, we evaluated OLIF for lumbar spine degeneration. There were few complications during surgery. In particular, psoas muscle and spinal nerve injury were avoided. Low back and leg pain significantly decreased after surgery.
In the current study, we used anterior OLIF without decompression in about half of the patients. Indirect decompression using ALIF has been reported.4,12 We previously reported the cases of 39 patients who underwent noninstrumented stand-alone ALIF for degenerative spondylolisthesis with an average follow-up period of 12 years.4 The following results were obtained: long-term clinical results were satisfactory for the patients; 76% of the patients had satisfactory results after 10 years, 60% after 20 years, and 52% after 30 years.4 We have also compared stand-alone ALIF and PLF for patients with single level spondylolisthesis. Forty-six patients diagnosed with L4 degenerated spondylolisthesis were treated using either ALIF or PLF, and both anterior and posterior methods reduced the patients' low back and leg pain; however, improvement of low back pain was significantly greater after ALIF.
In the current study, we applied ALIF plus transpedicular or cortical bone trajectory instrumentation without PLF (270° fusion). Some trials have compared various combinations of anterior, posterior, or combined fusion. Prospective randomized comparison of ALIF plus PLF (360° fusion) to ALIF plus transpedicular instrumentation without PLF (270° fusion) for degenerated spondylolisthesis showed that both 360° and 270° fusion significantly reduces pain, with no significant clinical differences between them.13 In cases of degenerative spondylolisthesis, no difference was observed in outcomes with the addition of PLIF to PLF instrumented fusion.14 A total of 148 patients, including those with spondylolisthesis, were randomly selected for either instrumented PLF or circumferential lumbar fusion.15 The circumferential group showed significantly better improvement of fusion rate and pain in comparison with the PLF.14 These conflicting results do not permit any conclusions regarding the relative effectiveness of anterior, posterior, or circumferential fusion.
Recently, a minimally invasive lateral transpsoas approach to the lumbar and thoracic spine, also known as XLIF or DLIF, has been used. This method has been used for degenerative lumbar disease, discogenic back pain, and kyphoscoliosis. Acosta, et al.16 analyzed changes in coronal and sagittal plane alignment following XLIF for degenerative scoliosis and noted excellent results for deformity correction in both planes. Recent studies of the surgical treatment of adult scoliotic deformity have found that XLIF results in less blood loss, shorter length of stay, and a lower incidence of infection, compared with traditional methods.17,18 Several authors have reported on indirect decompression using a standalone XLIF cage without posterior decompression or pedicle screws. A total of 84 stand-alone XLIF patients were evaluated and 68 patients showed evidence of solid arthrodesis and improvements in patient-reported pain and function scores.19 Twenty-one patients who underwent standalone XLIF were evaluated using X-ray imaging and MRI. In most patients, the XLIF procedure provides good surgical results and enlargement of the spinal canal after surgery.20 Nevertheless, 9.5% patients required a second procedure for additional posterior decompression and instrumentation. Further contrasting results were discovered in an investigation of stand-alone short-segment (1- or 2-level) XLIF in 98 patients. While significant gains in segmental lumbar lordosis and disc height were observed overall, some patients experienced less improvement because of a higher rate of interbody graft subsidence, which was correlated with transient clinical worsening.21 In the current study, we used posterior fixation to improve fusion rate and avoid revision surgery or cage subsidence. Our decisions for whether or not to perform posterior decompression were based on intraoperative myelography. However, there was a possibility that patients showing a narrow canal on intraoperative myelography may show improvements in pain after surgery without decompression. Further study is needed to clarify the criteria for posterior decompression.
Real-time EMG monitoring is required to avoid nerve injury during surgery; however, Cummock, et al.10 reported that of 59 patients who underwent XLIF surgery, 62.7% had thigh symptoms postoperatively. New thigh symptoms at first follow-up visit included burning, aching, stabbing, or other pain (39.0%), numbness (42.4%), paresthesias (11.9%), or weakness (23.7%). Davis, et al.22 reported the course of the lumbar plexus using eighteen cadaveric specimens: the femoral nerve is formed from the L2 to L4 nerve roots at the level of the L4-5 disc space and lies ventral to its posterior aspect. They concluded that during the transpsoas lateral surgical approach to the L4-5 disc space, the femoral nerve should be considered to be at risk intraoperatively because of the position and size of currently available retractors.22 Furthermore, Uribe, et al.23 discussed the potential of injury to the ilioinguinal, iliohypogastric, lateral femoral cutaneous, and genitofemoral nerves in the retroperitoneal space. Real-time EMG monitoring does not monitor sensory nerves. At the L4-5 level, the genitofemoral nerve runs anterior to the disc; the ilioinguinal and iliohypogastric nerves run across the mid-portion of the disc; and the lateral femoral cutaneous nerves run posterior to the disc.23 In the current study, we approached the disc between the aorta and psoas muscle. We did not conduct real-time EMG monitoring, and few patients showed any motor or sensory nerve injury or symptoms from the psoas muscle. In this regard, this OLIF method is useful for avoiding the complications reported for the XLIF procedure. Table 4 summarizes the merits and demerits of OLIF in comparison with other methods.
The current study has some limitations. First, it is a small-sized prospective study and the number of patients was restricted. Second, the duration of follow-up was short. Finally, we did not evaluate bone fusion or correction rates. Further study is required to clarify these points.
In conclusion, we evaluated OLIF plus posterior screws for patients with lumbar spinal degeneration disorders. Pain scores significantly improved after surgery, and there were no major complications during surgery or symptoms from nerve or psoas muscle injury. We concluded that OLIF provides reductions in pain without any major complications.







 XML Download
XML Download