

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The goal of anterior cruciate ligament (ACL) reconstruction is to return normal kinematics to injured knees. Advances in ACL reconstruction have emphasized the importance of positioning grafts within the existing anatomical insertion.1,2,3 The anteromedial portal technique for femoral bone tunnel drilling is more flexible and allows for more accurate anatomical positioning compared to the transtibial technique.4,5,6,7,8,9,10 However, anatomical ACL reconstruction is technically demanding and may require independent femoral and tibial bone tunnel drilling in order to avoid compromises to anatomical graft positioning.11,12 Unfortunately, the anteromedial portal technique can have complications because there is no accurate guiding system for femoral drilling. The large sized reamer via anteromedial portal bears a high risk for articular cartilage damage to the medial femoral condyle.4,7 It can also shorten the femoral tunnel length and compromise graft fixation at the femur.13,14 Many studies report the effects of graft length within the tunnel on graft healing and stability.15,16,17 Healing of the graft in connection with the tunnel plays an important role in fixation strength.18,19,20 Short femoral tunnels can lead to low fixation strength and rigidfix pin protrusion.14,21,22 Additionally, the anteromedial portal technique can lead to posterior wall blow-out.7
Many factors can affect femoral tunnel morphology after ACL reconstruction with the anteromedial portal technique such as knee flexion angle during creation of the femoral tunnel and obliquity of the femoral tunnel on the coronal and axial planes.13,23,24,25 The knee flexion angle is determined by surgeons during operation using a goniometer and the bending angle of the knee joint can be adjusted relatively accurately, however, in case of femoral tunnel creation, insertion angle of the femoral tunnel will be carried out with free handle technique, it is hard to set the correct insertion angle, and it is difficult to determine whether insertion angle is appropriate or not. However, no studies have documented results of three-dimensional tunnel orientation in accordance with tunnel entrance angles in anatomical ACL reconstruction. Therefore, we thought that investigate the three-dimensional study of femoral tunnel entrance angle and its outcomes. The purpose of this study was to evaluate entrance angle effects on femoral tunnel length and cartilage damage during anteromedial portal drilling using three-dimensional computer simulation in anatomical single bundle ACL reconstruction. The first hypothesis of this study is that angles lower than 30° in axial plane would produce longer and excessively vertical oriented tunnels and angles higher than 60° in axial plane would produce shorter and excessively horizontal oriented tunnels. The second hypothesis is that high angle in axial plane with shorter tunnel length represents higher possibility of medial femoral condyle damage.
MATERIALS AND METHODS
Three-dimensional modeling of cadaveric knees
Data was taken from an anatomic study performed using 16 cadaveric knees (12 males, 4 females). The mean subject age at the time of death was 65.4±6.2 years (range: 56-73 years). The specimens had no gross deformities. First, the ACL femoral insertion was dissected and the perimeter of the femoral ACL footprint was marked using a 1.5 mm drill bit and the knees were scanned by CT (Fig. 1). A three-dimensional model of each knee was reconstructed using MIMICS® software (Mimics 12.3, Materialise, Belgium) to verify the positions and to virtually remove the medial femoral condyle to better visualize the lateral femoral condyle and ACL footprint. The, three-dimensional measurements were calculated using Geomagic® software (Research triangle park, NC, USA). The center of the ellipse shaped anatomical ACL femoral footprint cross section area was automatically calculated by computer program (Geomagic® software), which is based on CT images of the perimeter femoral ACL foot print marked previously (Fig. 2). The femoral aperture centers were measured in anatomic posterior-to-anterior and proximal-to-distal directions using the Bernard's quadrant method relative to the femoral notch (Fig. 3).26 Distance 't' is defined the total sagittal diameter of the lateral femoral condyle measured along Blumensaat's line. It was limited by the intersections between this line and the ventral and dorsal borders of the femoral condyle. Also, distance 'h' is defined the height of the intercondylar space measured as the distance between Blumensaat's line and a tangent to the distal subchondral bone contour of the condyle parallel to Blumensaat's line. Distance 't' and 'h' defined the exact position of the center of the femoral ACL footprint within the coordinate system in the sagittal plane (Fig. 3).
Tunnel creation and measurement
Solidworks® software (Solidwork Corp., Waltham, MA, USA) was used to create femoral tunnel at the anatomical center of the ACL in different entrance angle on a three-dimensional plane. The tunnel was created in a 120° knee flexion state. The knee flexion angle and tunnel were created using a computer simulation set with the femur shaft flexed at 30° from the plane (Fig. 4). The authors have selected 0 degree relative to an imaginary line connecting the distal end of the femoral condyle. In addition, we selected angle of insertion in the coronal plane of the tunnel of this baseline as coronal angle. We also set virtual line connecting posterior end of lateral and medial femoral condyle as standardized 0 degree, axial angle was determined to be the angle of insertion in the axial plane of the tunnel on the base line. And we set plane perpendicular to the other two planes as sagittal plane, axis of femoral shaft as 0 degree, and insertion angle of tunnel of this baseline as sagittal angle. The virtual cylinder of 8 mm diameter was created by computer simulation. The three-dimensional entrance angle was set randomly to five different angles using 16 cadaveric knees. The angles at each plane were averaged by computer simulation. The standard angle was defined as drilled at a coronal angle of 45°, a sagittal angle of 45°, and an axial angle of 45° (Fig. 5) and the reason why the authors set a coronal angle of 45°, a sagittal angle of 45°, and an axial angle of 45° standard angle as standard angle is that average of measured femoral tunnel angle was similar to our determined standard angle on the analysis of CT images of patients who underwent anatomical single bundle ACL reconstruction prior to this study. The cylinders rested upon the anatomical center of the ACL footprint and were placed at five different positions, 30°, 40°, 45°, 50°, and 60° in the coronal plane and axial plane, and at 45° in the sagittal plane. With a femoral tunnel through the center of the ACL femoral insertion, the effect of different entrance angles on femoral tunnel length was determined. To evaluate the impact of entrance angle on damage to the medial femoral condyle cartilage, virtual cylinders of the reamer direction were created. We measured the distance between the medial femoral condyle and virtual cylinders. We concluded that the distance was closer to or in contact with the medial femoral condyle and risk for cartilage damage is higher.
Statistical analysis
One way ANOVA test was used was to compare the femoral tunnel length and distance from the medial femoral condyle to the virtual cylinder of the femoral tunnel by different angle entrances, and p-values of <0.05 were defined as statistically significant. Analyses were performed using SPSS software (SPSS Inc., Chicago, IL, USA) version 16.0.
RESULTS
Center of the ACL footprint
According to Bernard's quadrant method, the anatomical center of the ACL footprint was positioned at 33.9±4.7% along the t line (line parallel to Blumensaat's line) and 35.8±8.1% along the h line (line perpendicular to Blumensaat's line).
Femoral tunnel length
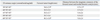
The mean length of the tunnel in the 30° coronal, 60° axial, and 45° sagittal group (34.0±2.9 mm) was significantly shorter than that of the standard angle group (39.5±3.7 mm; p<0.001). The 60° coronal, 30° axial, and 45° sagital group (46.3±3.8 mm) was significantly longer than the standard angle group (p=0.000) (Table 1). The length of the tunnel shorter than 30 mm occurred on three subjects
Distance between the virtual cylinder of the femoral tunnel and the medial femoral condyle
In tunnels drilled at a coronal angle of 45°, an axial angle of 45°, and a sagittal angle of 45°, the distance between the virtual cylinder of the femoral tunnel and the medial femoral condyle was 9.4±2.6 mm. In tunnels drilled at a coronal angle of 30°, an axial angle of 60°, and a sagittal angle of 45°, the mean distance between the virtual cylinder of the femoral tunnel and the medial femoral condyle was 0.7±1.3 mm, significantly shorter than that of the standard group (p<0.001). In this group, 12 cases showed zero distance, meaning the medial femoral condyle and the virtual cylinder of the femoral tunnel were in contact. There were no significant differences between the standard angle group and the other angle groups (Table 1).
DISCUSSION
The most important findings in this study are that insertion at low angle in coronal plane and high angle in axial plane tended to produce a shorter tunnel length compared to other tunnel lengths at different angles and higher incidence of medial femoral cartilage damage. In contrast, angles such as insertion at high angle in coronal plane and low angle in axial plane produced excessively vertical oriented tunnel. Recently, despite the many studies, the optimal method of creating femoral tunnels for ACL reconstruction is still controversial.5 In the present study, we defined an accurate anatomical single bundle ACL footprint center, and we evaluated tunnel lengths and incidence of medial femoral condyle cartilage damage in accordance with different entrance angles.
Restoring anatomy is a basic principle of orthopaedic surgery. Precise knowledge of tunnel location is critical for ACL surgery, which is based on applying anatomical reconstruction concepts. Many studies have shown that, according to anatomical concepts, positioning of the femoral tunnel within the footprint causes favorable clinical outcomes.4,22 Methods for measuring the center of the ACL footprint are variable and depend on radiographic descriptions, arthroscopic descriptions, and cadaveric gross descriptions.2,27,28,29 Piefer, et al.18 recommend anatomic descriptions that are fixed, independent of femoral positioning, anterior, posterior, proximal, and distal. Their results show that from proximal to distal, the anatomic center of the ACL femoral footprint is 43% of the distance from the proximal articular margin, which is arthroscopically visualized at the osteochondral junction to the distal articular margin on the lateral wall of the intercondylar notch. In another study, Luites, et al.30 reported the center of the ACL as being 7.9±1.4 mm distal along the notch roof and 4.0±1.3 mm posterior to the notch roof. However, the precise measurement of the center of the ACL footprint is difficult to obtain. In order to address this limitation, we created the femoral tunnel at the center of the ACL footprint by drawing accurate values using a software program and a three-dimensional computer simulated modeling system to virtually replicate the surgical condition. Our method for establishing real anatomical ACL footprint centers will contribute to greater accuracy of three-dimensional simulation studies.
The first hypothesis of the study is that as the angle in the axial plane grows smaller, the possibility of excessively vertical oriented angle tunnels forming grow larger as well, and vice versa. Five experiments at different settings were performed in order to affirm the first hypothesis. Tunnel lengths from a setting of coronal plane angle at 60° and axial plane angle at 30°, and a setting of coronal plane angle at 30° and axial plane angle at 60° showed statistically significant differences compared to other tunnel lengths in different settings from ours. Inappropriate femoral tunnel length has been cited as one of the causes of failure after ACL reconstruction.11,21 Many studies address the effects of tunnel length on graft healing and stability.23,24,31 Healing of the graft to the tunnel plays an important role in fixation strength. In this study, we observed excessively vertical oriented femoral tunnels resulting from entrance angels set at 60° coronal and 30° axial in the 3-dimensional model. Such femoral tunnel angle might induce extremely longer tunnel length that could alternate the graft function and graft stability.23,24 Drilling the femoral tunnel in an anatomic ACL reconstruction through anteromedial portal results in a more oblique and horizontal tunnel than traditional approaches.32,33,34 However, increasing femoral tunnel obliquity results in short femoral tunnels and possibly compromised femoral fixation due to posterior wall blowout and rigidfix pin protrusion.1,14,35 Additionally, short femoral tunnels result in less graft within the femoral tunnel, which may cause decreased graft healing and subsequent graft failure. Yasuda, et al.22 also advocate that 15-mm of graft inside the tunnel is sufficient for biological healing. Therefore, we assume that 30-mm of graft is the minimum adequate length for biological healing.21 Three-dimensional simulation in this study also suggests that angles lower than 30° in the coronal plane and 60° in the axial plane cause shorter femoral tunnel length. When considering the situations of notchplasty such as patients who have small intercondylar notch size or unexpected bone loss at the entrance area of the femoral ACL footprint, a length of at least several mm longer than 30-mm is recommended. These findings are in concordance with the results reported by Golish, et al.16 supporting concerns regarding graft-tunnel mismatch, insufficient graft-tunnel interface for healing, and limited options for fixation with such short tunnels.
The use of the anteromedial portal technique for femoral tunnel drilling provides more flexibility and accuracy in anatomic positioning compared to the transtibial techni-que.10,14,15,16,19,23,32 However, reaming through far anteromedial portal bears a high risk for articular cartilage damage to the medial femoral condyle.15,31 This finding is related to our second hypothesis that high angle in axial plane with shorter tunnel length represents higher possibility of medial femoral condyle damage. The exact incidence of surgical-associated articular cartilage damage in ACL reconstruction has not been reported. However, articular cartilage damage may be of highest clinical relevance for the patient. After recovery from the ACL injury, it may significantly influence postoperative symptoms, the degree of satisfaction with the surgery, function, activity levels, and the development of arthritis.31 Siebold, et al.36 recommends the "Guide Pin Maneuver" to avoid articular cartilage damage while traveling along the guide pin, and far anteromedial portal should be avoided. Although many studies report entrance angle influence on medial femoral condyle damage, most of these studies are two-dimensional plane based research which is founded on random anatomical center.4,7,36 Therefore, such angles do not represent condition in a three-dimensional plane, so the results from the studies are not reliable.4,7,36 However, our current simulation study shows that the distance between the virtual cylinder of the femoral tunnel and the medial femoral condyle was shortened by a lower angle in the coronal plane and by a higher angle in the axial plane. The 12 cases with tunnels drilled at a coronal angle of 30° and an axial angle of 60° showed contact with medial femoral condyle. This means that the virtual cylinder of the femoral tunnel and medial femoral condyle were in contact. A femoral tunnel with a lower angle in the coronal plane and a higher angle in the axial plane may injure the articular cartilage of the medial femoral condyle while traveling along the guide pin and reamer. We also found that a low angle in the coronal plane and a high angle in the axial plane may influence not only shorter femoral tunnel length, but also higher risk of cartilage damage on the medial femoral condyle. Consequently, based on our results, we suggest that the femoral tunnel entrance angle should be chosen within the standard angle and aside from extreme angles exceeding acceptable range in order to minimize cartilage damage on the medial femoral condyle.
The present study has several limitations that require consideration. First, the cadaveric specimens used in the present study might not represent the anatomical features and dimensions of the femur in patients undergoing ACL reconstruction. If patients have substantially larger femoral dimensions than our study subjects, different results would be encountered. Second, the small sample size is a weakness. Third, we used a virtual computer simulation to measure the length of the femoral tunnel using a relatively narrow range of compounded three-dimensional drilling angles. It is possible that the arranged angles do not represent all possible angles. Fourth, this is an in vitro computer simulation study. Thus, we did not consider the in vivo situation such as entry position of guide pin, position of anteromedial portal, and soft tissue structures that influence to the portal position. However, this is the first report to display a three-dimensional image using accurate ACL femoral footprint centers to aid femoral tunnel positioning at various entrance angles. Our goal was to characterize the center of the femoral footprint, the femoral tunnel length, and the distance between the imaginary extension of the femoral tunnel and the medial femoral condyle as they correlate to three-dimensional drilling angle. The computer model allowed us to accurately evaluate these parameters and directly visualize the length of the femoral tunnel and relation between the femoral tunnel and medial femoral condyle. We also analyzed the tunnel in three dimensions (coronal, axial, sagittal) rather than two. This allowed for emphasis to be placed on size factors, obtained by two-dimensional studies, and on direction factors, obtained by three-dimensional studies.
Extremely low and high entrance angles in both of axial plane and coronal plane produced inappropriate tunnel angles, lengths and higher incidence of cartilage damage. We recommend that angles in proximity to standard angles be chosen during femoral tunnel drilling through the anteromedial portal.




 XML Download
XML Download