

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is characterized by progressive and partially reversible airflow limitations associated with an abnormal inflammatory response of the lungs to noxious particles or gases.1 COPD restricts daily activities as a result of reduced pulmonary function, dyspnea, or limitations in exercise tolerance. Pulmonary function tests remain the standard method for grading COPD severity in international treatment guidelines. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommended that both pulmonary function and disease-specific quality of life be monitored regularly to guide any changes in treatment.1
Dyspnea is one of the major symptoms of COPD and it impairs quality of life in such patients. Moreover, dyspnea is known to be correlated with objective and subjective measurements of COPD.2 Several instruments are available to assess dyspnea: The Medical Research Council (MRC) dyspnea scale has been in use for many years to assess the effect of breathlessness on daily activities.3 Other dyspnea scales include the Visual Analogue Scale, Oxygen Cost Diagram, Borg dyspnea scale, and baseline or transitional dyspnea index for use in clinical practice. The MRC scale measures activity limitation or disability due to dyspnea rather than the severity of dyspnea itself, and thus, measures the chronic effect of disease.
Disease-specific quality of life is being recognized as an important outcome when evaluating patients with COPD.4,5 COPD-specific quality of life measurements, including the St. George's Respiratory Questionnaire (SGRQ)6 and Chronic Respiratory Questionnaire,7 have been validated and used extensively in clinical studies. However, these questionnaires are complex and time-consuming to complete and may require specialist software or licenses to use, which limits their applicability in routine practice.
The COPD assessment test (CAT) was recently developed as a short, simple instrument for qualifying the symptom burden of COPD in routine practice, and enables better communication between patients and healthcare professionals about the consequences of the disease. The CAT was derived from 21 candidate items identified through qualitative research of patients with COPD from COPD prospective international studies.8-11
In the present study, dyspnea severity was evaluated by the MRC scale. Patient COPD-specific quality of life was assessed with CAT score as a disease specific measure. The purpose of this study was to evaluate the effect of the dyspnea on disease-specific quality of life detected by CAT score in patients with COPD.
MATERIALS AND METHODS
Subjects
Patients with stable COPD, as defined by GOLD, were recruited from our outpatient clinic from October 2010 to May 2011. All patients had undergone at least 6 months of outpatient management. The entry criteria for the study were as follows: 1) a known post-bronchodilator forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) ratio of <70% and an FEV1 <80% (except GOLD I patients) of the predicted value for all measurements made over the prior six months; 2) a smoking history of >10 packet-years; 3) no history suggestive of bronchial asthma; 4) no exacerbations of the airflow limitation over the preceding six weeks; and 5) no changes in treatment regimen over the preceding four weeks. Exclusion criteria were any current pulmonary disorder other than COPD and serious, unstable cardiovascular or neurological disease.
All eligible patients finished the following examinations on the same day: pulmonary function tests, assessment of their dyspnea, and assessment of their disease-specific quality of life by CAT. All tests and questionnaires were administered by investigators in a face-to-face interview. The ethics committee of our institute approved the research protocol and written informed consent was obtained from all participants.
Demographic information, medical history, blood chemistry, previous and current COPD medications were recorded. The history of exacerbations in the previous one year was also recorded. An exacerbation was defined as a worsening of the symptoms that required oral corticosteroids and/or antibiotics and/or hospitalizations. All patients were treated according to GOLD guidelines.
Pulmonary function tests
The diagnostic classification was performed by pulmonary physicians according to GOLD guidelines. Post-bronchodilator FEV1 was assessed at 20 min after the inhalation of salbutamol 200 mcg plus ipratropium 40 mcg using a metered dose inhaler. Spirometry was performed using a Flowscreen Pro spirometer (JAEGER Inc., Hoechberg, Germany) according to established guidelines.12
Assessment of the CAT
The disease-specific quality of life was assessed with the Turkish version of the CAT.14 The CAT comprised eight items assessing cough, phlegm, chest tightness, breathlessness going up hill/stairs, activity limitations at home, confidence leaving home, sleep and energy. Each item was scored from 0 to 5 giving a total score from 0 to 40, corresponding to the best and worst health status in patients with COPD, respectively.9 Scores of 0-10, 11-20, 21-30 and 31-40 represented mild, moderate, severe or very severe clinical impact, respectively.15
Statistical analysis
Data were analyzed using SPSS-PC (Version 15.0, SPSS Inc., Chicago, IL, USA). All indices are expressed as mean±SD. The relationship between variables of patients was calculated by Pearson's correlation coefficient(r). Proportions of patients with different MRC grades across the GOLD stages and CAT scores were analyzed by chi-square test. Multiple group comparisons of quantitative variables were made using analysis variance. Inter-group comparisons were carried out using multivariate analysis and the Bonferroni's test to identify significantly different groups. p-values less than 0.05 were considered significantly.
RESULTS
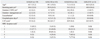
Ninety patients with COPD were evaluated. The average age of the patients was 68.5±10.9 (range: 41-97) years; duration of COPD, 8.1±8.4 (range: 1-50) years; and duration of management, 6.1±7.1 (range: 1-40) years. Nineteen patients were GOLD stage I, 43 patients were GOLD II, 26 patients were GOLD III, and 2 patients were GOLD IV. Table 1 shows the demographic and clinical characteristics according to GOLD stage.
Table 2 shows the inter-correlations among the CAT score and clinical characteristics of the patients. The CAT scores were correlated with duration of COPD, duration of management, hospitalization days, and exacerbation.
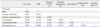
With respect to the CAT scores, 24 patients were CAT I (mild), 33 patients were CAT II (moderate), 27 patients were CAT III (severe), and 6 patients were CAT IV (very severe). Table 3 shows the study variables according to CAT score. The dyspnea scale, exacerbation, and disease duration were significantly different among the CAT score groups.
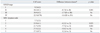
Table 4 shows the differences in CAT scores between classes of other COPD impairment measurements. There were significant differences between GOLD I and GOLD II stages (p=0.001), as well as between MRC scales 1 and MRC scales 2 and 3 (p=0.021, p=0.001, respectively). Other measurements were not significant.
DISCUSSION
In our study, CAT scores were shown to be associated with disease features, including duration of COPD, duration of management and exacerbation, while GOLD stages were not. While stage of the disease was evaluated with a spirometry test according to GOLD guidelines, CAT score measures clinical, symptomatic state and quality of life. This may be the reason for the close relationship between characteristics of the disease and CAT score.
Dyspnea is a major symptom in patients with COPD. Several studies have investigated the relationship between dyspnea severity and spirometric measurements of FEV1 or FVC to determine the relationship between dyspnea scales and pulmonary function. Some authors found that pulmonary function was significantly correlated with dyspnea scales.16-18 In contrast, other authors found that it was not correlated with dyspnea scales.19,20 Ozalevli and Ucan13 observed that dyspnea score obtained from MRC was correlated with spirometric measurement (FEV1). The MRC scale is the most commonly used scale because of its simplicity, easy of administration and established validation as a useful marker in COPD.21 Additionally, MRC scale was shown to predict the likelihood of survival in patients with COPD.22
The relationship between dyspnea and quality of life in COPD has previously been indicated in a few studies.23,24 Perceived dyspnea was shown to have a greater impact on health-related quality of life than spirometric or functional measurements in these patients.25 In an international study, the most frequently reported symptom was dyspnea (78%) and the most frequent complaint reported by patients with COPD was daily activity limitation.26 Hajiro, et al.24 showed that dyspnea is one of the main determinations of disease-specific health related quality of life, and has moderate-to-strong correlations with impairments in the health related quality of life in patients with COPD. On the other hand, quality of life measurements did not correlate well with the severity of airflow limitation.27 Furthermore, factors such as dyspnea, depression, anxiety and exercise tolerance were found to be more correlated with health status than the widely used spirometric values.28
The CAT was developed as a short validated COPD-specific questionnaire for assessing the impact of COPD on health status. It provides a reliable measure of overall COPD severity from the patient's perspective, independent of language.9 The CAT has been translated to 58 different languages, available on their web site.14 It is not a diagnostic tool; its role is to supplement information obtained from lung function measurement and assessment of exacerbation risk.8,9 The relative frequency of severe exacerbations within these patients was shown to be higher in patients with higher CAT scores. We observed that the increase of exacerbation frequency was parallel to the increase of CAT scores. Additionally, CAT scores were the same in males and females, and were not influenced by age.9 In our study, it was observed that the CAT scores were not influenced by sex, age or body mass index.
It has been suggested that CAT is likely to offer relevant alternatives to complex tools such as the SGRQ. Jones, et al.8 reported an extremely strong correlation between CAT and SGRQ. They observed that small differences in health status impairment between patients in GOLD stage I and II can be seen with the CAT. In present study, we discerned that no difference in health status impairment among GOLD II, III and IV stage patients can be seen with the CAT. In contrast, there was significant difference between patients of GOLD stages I and II according to CAT. Also, Jones, et al. reported a significant difference in all grades of MRC dyspnea scales according to CAT scores. We, however, observed a difference only in MRC 1, 2, and 3 grades.
In our study, CAT scores was classified as mild, moderate, severe and very severe. There was a significant relationship among these classifications of CAT and COPD patient features and dyspnea scale. We suggest that CAT classification is compatible with COPD severity levels.
As the CAT score was shown to be correlated with clinical characteristics and quality of life, it can also be expected to be associated with the prognosis of the disease. However, as this study is a cross-sectional study and has limitations to showing the prognostic value of CAT score, a follow-up study of patients may demonstrate relationships between CAT and prognosis.
We should mention some of the limitations of the present study. First, since we recruited only stable patients from an outpatient clinic, the study sample may not to be representative of patients with exacerbation. Additionally, the study sample was small, and the study was not a multicentre or an international study. Second, CAT and dyspnea scale are self-administered questionnaires, but we used an observer to complete the questionnaires.
In conclusion, dyspnea greatly impacts the health related quality of life of patients with COPD. We concluded that the CAT, a novel COPD-specific measurement, was associated with dyspnea scale, duration of COPD and exacerbation, but not co-morbidities. The CAT may be a simple short questionnaire for assessing disease severity levels in patients with COPD. At the moment, more studies from other countries around the world are needed to ascertain the value of the CAT.

 XML Download
XML Download