

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The loading of clopidogrel before percutaneous coronary intervention (PCI) has become a standard procedure since several randomized trials demonstrated the efficacy of clopidogrel loading.1,2 Several studies have shown that the standard 300 mg loading dose of clopidogrel is inadequate to optimally inhibit platelet reactivity, and a 600 mg dose of clopidogrel has been reported to show superior outcomes in patients with stable angina3 or non ST-segment elevation acute coronary syndrome,4 undergoing PCI. Although recent studies reported that a 600 mg loading dose of clopidogrel reduced adverse ischemic events in patients undergoing primary PCI for ST-segment elevation myocardial infarction (STEMI),5,6 there are incomplete data on long-term clinical outcomes beyond 1 year and few studies have targeted Asian populations. Therefore, we evaluated the short- and long-term effects of 600 mg versus 300 mg clopidogrel loading doses on clinical outcomes in Asian STEMI patients undergoing primary PCI.
MATERIALS AND METHODS
Study population
We recruited 1107 consecutive patients who were admitted for STEMI and underwent primary PCI with drug-eluting stents (DES) at three major cardiology centers in Korea between August 2003 and January 2009. STEMI was defined as presence of typical chest pain for ≥30 minutes, and the presence of ST-segment elevation ≥1 mm in at least two contiguous leads, or presumably new left bundle branch block. Patients were excluded, if they presented with cardiogenic shock or did not undergo primary PCI within 12 hours after symptom onset. Since 416 patients did not fulfill the selection criteria, 691 STEMI patients were included in this study. Baseline clinical, peri-procedural characteristics, use of medications, and outcome data were recorded prospectively by research coordinators of the dedicated PCI registry of each hospital. The institutional review board of each hospital approved this study, and waived requirements for informed consent for this database analysis.
Percutaneous coronary intervention and medical treatment
All patients received loading of dual oral antiplatelet agents with 300 mg of aspirin along with 600 mg or 300 mg of clopidogrel as early as possible before PCI. The initial loading dose of clopidogrel was left to the physician's judgment. Coronary angiography and stent implantation were performed by standard interventional techniques. Use of glycoprotein IIb/IIIa receptor inhibitors, selection of stent type, pre-dilatation and post-stent adjunctive ballooning were also left to the operator's discretion. In patients with multi-vessel coronary artery disease, primary PCI was recommended only on the infarct related artery. The medical treatments such as β-blockers, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, calcium-channel blockers, or statins were started during in-hospital period. All patients were prescribed lifelong aspirin (100-200 mg/day) and clopidogrel (75 mg/day) for at least 6 months.
Endpoints and definition
The primary outcome was major adverse cardiac events (MACEs) during follow-up, defined as a composite of all-cause death, reinfarction, or target vessel revascularization (TVR). Clinical events were defined based on the recommendations of the Academic Research Consortium.7 All deaths were considered cardiac, unless a definite non-cardiac cause could be established. A reinfarction was defined as elevated cardiac enzymes (troponin or myocardial band fraction of creatine kinase) greater than the upper limit of the normal value with ischemic symptoms or electrocardiographic findings indicative of ischemia that were not related to the index procedure. TVR was defined as repeat revascularization of the target vessel by PCI or bypass graft surgery. Definite, probable, or possible stent thrombosis was defined according to the Academic Research Consortium recommendations.
Statistical analysis
Continuous variables were expressed as medians (interquartile range) or mean±standard deviations and were compared using Student's t-test if the data followed a normal distribution and Wilcoxon rank sum test if the data were skewed. Categorical variables were compared with the chi-square test or Fisher exact test. Adjusted hazard ratio and corresponding 95% confidence intervals were compared with multivariate Cox hazard models in order to adjust for differences between patients in the 600 mg and 300 mg clopidogrel groups. To reduce selection bias of treatment for clopidogrel loading doses and potential confoundings, we performed strict adjustment for baseline characteristics of patients in the 600 mg and the 300 mg clopidogrel groups using propensity score. The propensity scores were calculated using binary logistic-regression analysis. A full non-parsimonious model was developed and included all variables listed in Table 1. The discrimination and calibration abilities of the propensity-score model were reviewed through the c-statistic and the Hosmer-Lemeshow statistic. The c-statistic in our study was 0.629. We evaluated the balance in baseline covariates between the two groups in a propensity score-matched population. Covariates statistically significant on univariate analysis and/or those clinically relevant were regarded as candidate variables in multivariate models (sex, age, Body Mass Index, diabetes mellitus, initial left ventricular systolic ejection fraction by echocardiography, left anterior descending coronary artery as culprit vessel, multi-vessel coronary artery disease, types of DES, glycoprotein IIb/IIIa inhibitor, and clopidogrel 600 mg loading dose). All p-values were 2-tailed and p<0.05 was considered significant. Data management and analysis were performed using Statistical Package for the Social Sciences (SPSS) software, version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
Overall population
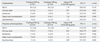
Of 691 patients, 381 patients received a 600 mg loading dose and 310 patients received a 300 mg loading dose of clopidogrel before PCI. Baseline clinical characteristics (Table 1) were not significantly different between the two groups, except for higher baseline hemoglobin levels in patients loaded with 600 mg compared with the 300 mg group. Procedural indexes (Table 1) were also mostly comparable, except for differences in the types of DES implanted. Patients in the 600 mg group were more likely to be treated with Zotarolimus-eluting stents and less likely to be treated with Sirolimus-eluting stents. The medications administered to the patients during in-hospital period are listed in Table 1. The 600 mg loading dose group patients received more glycoprotein IIb/IIIa receptor inhibitors during the procedure and more statins than the 300 mg loading dose group patients.
Propensity-matched population
A total of 548 matched cases, 274 in each of the clopidogrel groups, were found. There were no significant differences in baseline clinical, peri-procedural characteristics and in-hospital medications (Table 1), including glycoprotein IIb/IIIa receptor inhibitors during the procedure.
Clinical outcomes
Overall population
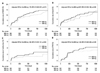
There were no differences in 1 month MACEs (3.2% versus 2.3%, p=0.481), all-cause death (2.1% versus 1.3%, p=0.429), reinfarction (1.3% versus 1.3%, p=0.984), TVR (0.8% versus 1.0%, p=0.799), and definite and/or probable stent thrombosis (0.8% versus 1.0%, p=0.799) between the two clopidogrel groups. Long-term clinical follow-up was successfully completed in 96% of the subjects. After a median follow-up of 921 (interquartile range 542-1223) days, clinical outcomes were similar between the two groups (Fig. 1). Clopidogrel loading dose was not an independent predictor of MACEs, all-cause death, reinfarction, TVR, and definite and/or probable stent thrombosis (Table 2).
Propensity-matched population
The results of propensity score-matched analysis were comparable to those of the main analysis in the overall population. There were no differences in 1 month clinical outcomes (for MACE 1.5% versus 1.8%, p=0.751, for all-cause death 0.4% versus 0.7%, p>0.99, for reinfarction 1.5% versus 1.5%, p>0.99, for TVR 0.7% versus 1.1%, p>0.99, and for definite and/or probable stent thrombosis 0.7% versus 1.1%, p>0.99, respectively) between the clopidogrel two groups among propensity score-matched patients. There were 24 MACEs with a median follow-up of 928 (interquartile range 542-1237) days in the matched patients. Also, there were no differences in long-term clinical outcomes between 600 mg and 300 mg loading dose of clopidogrel groups (Fig. 2). Loading dose of clopidogrel was not an independent predictor of MACEs, all-cause death, reinfarction, TVR, and definite and/or probable stent thrombosis even after propensity score matching, as well (Table 2).
Analysis according to tertiles of propensity score
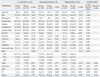
We compared and analyzed baseline characteristics and clinical outcomes for clopidogrel loading doses within the tertiles of propensity score (Table 3). Patients in the highest tertile of propensity score were more likely to have hypertension, higher initial left ventricular ejection fraction by 2D-echocardiography, and to use glycoprotein IIb/IIIa receptor inhibitors. The frequency of diabetes mellitus and prior myocardial infarction were higher in the lowest tertile compared with other tertiles. Patients in the intermediate tertile of propensity score were more likely to have dyslipidemia. There was a significant difference in stent types implanted between the tertiles. However, no significant differences in baseline characteristics were observed between 600 mg and 300 mg groups within each tertile. Regarding clinical outcomes, patients in the highest tertile of propensity score demonstrated a tendency to have a higher rate of death. However, there were no significant differences in death rate between 600 mg and 300 mg groups within the highest tertile. And also, no significant differences in reinfarction, TVR, stent thrombosis, and MACEs were observed, according to the tertiles of propensity score. There were no significant interactions between the loading doses of clopidogrel and tertiles of propensity score for each endpoint.
Subgroup analysis
To determine whether similar outcomes between the two groups were consistent in the various subgroups, we performed subgroup analyses (Fig. 3). The rates of MACEs were not different between the two groups in various subgroups, and there were no significant interactions between the loading doses of clopidogrel and MACEs among the nine subgroups.
DISCUSSION
The present study reports a current evaluation of long-term clinical outcomes for Asian patients who received either a 600 mg or 300 mg loading dose of clopidogrel and underwent primary PCI for STEMI. The major finding was that a 600 mg loading dose of clopidogrel was not associated with better long-term clinical outcomes compared with the conservative 300 mg loading dose.
According to the 2009 Focused Updates, ACC/AHA STEMI and PCI Guidelines recommended that at least 300 to 600 mg of clopidogrel should be given as early as possible (Class I/level of evidence A), instead of describing a specific loading dose of clopidogrel.8 Consequently, the optimal loading dose of clopidogrel has not been established yet. Moreover, there was no long-term data comparing clinical outcomes of a 600 mg with 300 mg loading dose of clopidogrel beyond 1 year, and there are incomplete data on comparison of the effectiveness of loading doses of clopidogrel for primary PCI in Asian STEMI patients.
Our results are different from those of previously conducted large-scale clinical trials, the HORIZONS-AMI trial5 and the CURRENT-OASIS 7 trial.6 We considered that there are several reasons why our results were different from those of the two above trials. First, the benefits of high dose clopidogrel in the HORIZONS-AMI trial and double dose clopidogrel in the CURRENT-OASIS 7 trial were mainly attributable to a lower rate of myocardial infarction and stent thrombosis. However, the rates of reinfarction and stent thrombosis of both the 600 mg and 300 mg groups in our study were lower than that of the high dose group in the HORIZONS-AMI trial or double dose group in the CURRENT-OASIS 7 trial. Therefore, there might be little room to improve with 600 mg loading dose of clopidogrel. Second, the ethnic differences in platelet aggregation or in clopidogrel responsiveness may be thinkable. A recent study reported that clopidogrel low-responsiveness evaluated by the Verifynow™ P2Y12 assay is an independent predictor of stent thrombosis and composite end point of stent thrombosis or cardiac death in patients with acute coronary syndrome within 6 months after DES implantation.9 Previous studies have also showed that carriers of the reduced function CYP2C19 allele have significantly lower levels of the active metabolite of clopidogrel, reduced platelet inhibition, and an increased rate of cardiovascular events,10,11 even with higher doses of clopidogrel.12 This polymorphism has been observed in a higher rate of East Asians compared with Caucasions.13 So, the efficacy of high or double dose clopidogrel shown in Western people may not equal in Asian people. Instead, triple anti-platelet therapy including cilostazol may be superior to dual anti-platelet therapy, including higher doses of clopidogrel in Asian patients.14-16 Finally, it is not clear whether the beneficial effects were a result of the double loading, double maintenance dose or both in the CURRENT-OASIS 7 trial. Additionally, other acute coronary syndrome patients were enrolled as well as those with STEMI in the CURRENT-OASIS 7 trial. Therefore, these could be the reasons for the differing results of the present study.
On the other hand, results of the present study correspond with the results of a recently published trial, in which there were no differences in 1 and 12 month clinical outcomes between the two clopidogrel groups in STEMI patients undergoing primary PCI, from a large acute myocardial infarction registry.17 Similarly, the GRAVITA trial showed that among patients with high on-treatment reactivity after coronary intervention with drug-eluting stents, the use of high-dose clopidogrel compared with conventional-dose clopidogrel did not improve the clinical outcomes, such as death from cardiovascular causes, nonfatal myocardial infarction, or stent thrombosis.18
Study limitations
There are several limitations to our study. First, the sample size of the present study was relatively small, and therefore would not allow for drawing a definite conclusion. Second, this study was not a randomized study. The clopidogrel loading dosage was left to the discretion of the treating physician. Despite our effort to adjust for potential confounders by using multivariable models and propensity score match analysis, it is likely that unmeasured covariates could have contributed to the observed differences in clinical outcomes. Third, our evaluation of clinical outcomes was limited by the fact that bleeding events were not included in our analysis. Bleeding events have been known to play a role in the mortality of STEMI patients.19
In conclusion, in Asian patients undergoing primary PCI for STEMI, the use of a 600 mg loading dose compared with a 300 mg loading dose of clopidogrel did not reduce the incidence of MACEs, all-cause death, reinfarction, target vessel revascularization, or stent thrombosis. Further study for clopidogrel loading doses in this subset of patients is needed to improve clinical outcomes.



 XML Download
XML Download