

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Deep neck infection is an infection in the potential spaces and fascial planes of the neck, either with abscess formation or cellulitis. Although infections were encountered more frequently in the pre-antibiotic era and were associated with poor oral hygiene, they can still cause significant morbidity and mortality, despite the present administration of antibiotics and the improvements of modern dental care. Life-threatening complications include: descending mediastinitis, septic shock, upper airway obstruction, jugular vein thrombosis, venous septic embolus, carotid artery pseudoaneurysm or rupture, pleural empyema, pericarditis, pericardial effusion, aortopulmonary fistula, adult respiratory distress syndrome, acute renal failure, epidural abscess, and disseminated intravascular coagulopathy.1-3 If any of these conditions occur, the results are ominous. The mortality rate can reach 40% to 50% in cases with mediastinitis.4,5
The clinical course and complications of deep neck infections have been well described in the previous literature, including a few recent large population studies.6-9 However, these studies were limited by the inclusion of peritonsillar abscesses, a small number of total and complicated cases, and small proportions of mediastinal complications. If the predisposing factors of complicated deep neck infections are identified with large population studies, appropriate treatment can be provided as soon as possible in order to reduce the mortality and morbidity rates of these cases. The purpose of this study is to identify the predisposing factors for longer hospitalizations and life-threatening complications in deep neck infections.
MATERIALS AND METHODS
The authors reviewed the medical records of 158 patients who were diagnosed with having deep neck infections, of which 23 patients had life-threatening complications. All patients were treated at the Department of Otolaryngology and Head and Neck Surgery in the Chonnam National University Hospital between the years of 1995 to 2004. Cases were excluded if they had peritonsillar abscesses, superficial infections, infections related to external neck wounds (traumatic or surgical), or head and neck tumors.
A computed tomography (CT) with contrast enhancement was performed on all of the patients in order to identify the extent of the infections and to differentiate cellulitis from abscesses. The authors performed surgery as the primary type of therapy in cases with abscesses over 2000 mm3 in size, and medical treatment in cases with cellulitis or small abscesses (≤ 2000 mm3).10 The volumes of the abscesses were estimated in mm3 (length × width × height). Empirical intravenous antibiotics (beta-lactamase-resistant beta-lactam antibiotics, aminoglycosides, and metronidazole) were administered before the culture results were available, and the antibiotics regimen was modified based on the culture and sensitivity results. The involved spaces were divided based on previously published descriptions.11,12 The authors classified Ludwig's angina with the group in the submental space. Unclassified abscesses were categorized according to the sites.
The authors used multiple linear regression with SPSS 12.0 as the statistical method to determine which variables contribute to longer hospitalizations. In addition to the variables of Wang et al's study, more candidate variables were added for analysis.6 The dependent variable was the duration of the hospital admission, and independent variables included age, sex, locations of involved spaces, numbers of involved spaces, a fever > 38℃, chills, neck swelling, neck pain, trismus, dysphagia, dyspnea, duration of symptoms, WBCs > 15,000cells/mm3, diabetes mellitus, causative bacteria (Klebsiella pneumoniae, Streptococcus viridans, and Methicillin-sensitive Staphylococcus aureus), etiologies (pharyngotonsillitis, odontogenic causes, congenital neck cysts, and foreign bodies), treatment methods (medical treatments, external drainage, and intraoral drainage and/or aspirations), and complications (mediastinitis, sepsis, and airway distress). The causes of infection were diagnosed based upon physical examination findings, patient history, and radiologic findings. Odontogenic causes were diagnosed through dental consultations.
In addition, logistic regression with SPSS 12.0 was used to determine the variables that contribute to complicated deep neck infections. In addition to the variables in the Wang et al's study,6 more candidate variables were added for analysis. The dependent variable was the specific complication; and the independent variables included age, sex, locations of involved spaces (submandibular, parapharyngeal, retropharyngeal, and submental), fever > 38℃, chills, neck swelling, neck pain, trismus, dysphagia, dyspnea, duration of symptoms, WBCs > 15,000 cells/mm3, number of involved spaces (one or two spaces vs. more than two), diabetes mellitus, causative bacteria (Klebsiella pneumoniae, Streptococcus viridans, and Methicillin-sensitive Staphylococcus aureus), and etiologies (pharyngotonsillitis, odontogenic causes, congenital neck cysts, and foreign bodies).
RESULTS
Demographics and clinical findings
There were 89 men and 69 women, with a male to female ratio of 1.29:1. Patient ages ranged from 1 to 89 years old, with a mean of 35.4 years. The most common symptom was neck swelling (74.7%), followed by neck pain (41.1%), fever (14.6%), chills (10.1%), dyspnea (10.1%), dysphagia (6.3%), and trismus (1.9%).
Etiology
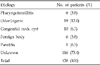
The most common cause of deep neck infections was odontogenic (19 cases, 12.0%), followed by pre-existing congenital neck cysts (10 cases, 6.3%) (Table 1).
Bacteriology and underlying diseases
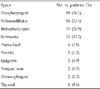
The results of bacterial cultures were positive in 73 (46.2%) patients. Klebsiella pneumoniae (10 cases of 73 culture positive cases, 13.7%) was the most common pathogen among the positive cultures, followed by Streptococcus viridans (9 cases, 12.3%), Methicillin-sensitive Streptococcus aureus (MSSA) (8 cases, 11.0%), and α-hemolytic Streptococcus (6 cases, 8.2%). Mixed infection reached 9.6% (7 cases). There were 9 species of anaerobes cultured: Bacteroides fragilis (1 case), Peptostreptococcus anaerobius (2 cases), Pasteurella haemolytica (1 case), Prevotella intermedia (1 case), Gemella morbillorum (3 cases), Enterobacter cloacae (1 case), Actinomyces meyeri (1 case), Clostridium tetani (1 case), and Corynebacterium species (2 cases).
There were 27 patients with diabetes mellitus (DM), 5 patients with chronic liver disease, and 9 patients with malignancies. Of the 10 patients who had Klebsiella pneumonia as a pathogen, 7 of the patients (70%) had DM.
Involved spaces of deep neck infections
The involved spaces overlapped, and the most common site was the parapharyngeal space (89 cases, 56.3%), followed by the submandibular space (56 cases, 35.4%), the retropharyngeal space (33 cases, 20.9%), and the submental space (24 cases, 15.2%) (Table 2). Of the 158 patients, 110 (69.6%) had one involved space, 37 (23.4%) patients had two, and 11 (7.0%) patients had more than two (7 patients had three involved spaces, 3 patients had four, and 1 patient had five).
Treatment
Surgery was performed in 121 (76.6%) cases, including catheter drainage in 11 cases, intraoral drainage in 17 cases, transcervical drainage in 90 cases, and combined transcervical and thoracotomy drainage in 3 cases.
Complications and durations of hospital stays: statistical analysis
There were 23 patients who developed life-threatening complications: descending mediastinitis (14 cases), sepsis (6 cases), and airway distress (9 cases) (Table 3). The crude mortality rate was 1.9% (3 cases) and septic shock was the cause of death in all cases. The duration of admission ranged from 3 to 70 days with an average of 14.1 days.
In multiple linear regression, patients with a large number of involved spaces (p = 0.027), DM (p = 0.048), and complications (p = 0.001) required longer hospitalizations. The remaining variables were not statistically significant (Table 4). In logistic regression, patients with more than two involved spaces (p = 0.010), were more likely to have complicated deep neck infections. Patients with odontogenic causes (p = 0.037) were less likely to have complicated deep neck infections. The remaining variables were not statistically significant (Table 5).
DISCUSSION
Deep neck infections can arise from various head and neck regions, including the teeth, salivary glands, nasal cavity, paranasal sinuses, pharynx, and adenotonsillar tissues. In the pre-antibiotic era, studies demonstrated that most (70-80%) deep neck infections resulted from complicated pharyngeal infections.13 A decreased incidence (9-16%) of pharyngotonsillar sites of origin has been recently described.7-8,13 In this study, only 3.8% of the patients presented with pharyngotonsillar sites of origin. Some reports indicated a significant prevalence (22.7-43%) of deep neck infections that were caused by dental infections.7-9 Similarly, the current study found the most common cause to be dental infections (12%). This may be due to the delay of treatment caused by the relatively high cost of dental care and public indifference to dental health compared with pharyngotonsillitis. There were some reports that indicated complicated or serious deep neck infections, such as descending necrotizing mediastinitis or cervical necrotizing fasciitis, secondary to odontogenic infections.14-20 However, in this study, logistic regression revealed that odontogenic causes were negatively correlated with complicated deep neck infections (p = 0.037). The 19 patients in our study that had relatively mild odontogenic infections responded well to treatment. Thirteen of the 19 (68.4%) had only one involved space. The submandibular space was most commonly involved (10 cases, 52.6%) and was easily managed. There were only two patients with complicated infections with odontogenic causes. Both completely recovered with properly managed treatment.
In this study, 10 cases (6.3%) had deep neck abscesses that resulted from acute suppurative infections of pre-existing congenital neck cysts. Prompt surgical treatment is recommended for congenital neck cysts after the control of the infection is established. In over half of the cases, the causes of infection remain unknown. The reason may be that an inciting infection can precede the deep neck infection by weeks, and it is often difficult to discern the primary source of infection, as indicated in previous reports.6,9,13,21,22
The present study demonstrated that Klebsiella pneumoniae (10 cases, 13.7%) accounted for the most common pathogen among the positive cultures, followed by Streptococcus viridans (9 cases, 12.3%). This differed from other reports in which Streptococcus viridans was the most common pathogen.7,23,24 Wang et al recently reported that Klebsiella pneumoniae was the most common pathogen.6 MSSA was found in only 8 (11.0%) positive cultures. This result was lower than those of other reports.10,23 These findings reflected the declining incidence of pharyngotonsillitis, and the increasing incidence of dental infections and immunocompromise as causes of deep neck infections.6
The most common associated systemic disease was diabetes mellitus (DM). Of the 10 patients who had Klebsiella pneumoniae as a pathogen, 7 (70%) patients also had DM. This was most likely because the virulence of Klebsiella was determined by the hosts' macrophage function,25 and the macrophage function was impaired in the hyperglycemic state.26 For those patients with DM, control of blood sugar plays an important role in the treatment strategy. In the present study, patients with DM stayed significantly longer in the hospital than non-diabetic patients (p = 0.020, student t-test). Although DM was not a significant predisposing factor of complicated deep neck infections (p = 0.054), diabetic patients should be considered high-risk patients when treating these types of infections.
One hundred ten (69.6%) cases of the 158 patients had one involved space, 37 (23.4%) patients had two involved spaces, and 11 (7.0%) patients had more than two involved spaces. In this study, having more than two involved spaces was found to be a significant predictor of complicated deep neck infections (p = 0.010).
No clinical symptoms and signs correlated with longer hospitalizations or complicated deep neck infections. However, Wang et al reported that in female patients, neck swelling and respiratory difficulty were high risk factors of deep neck infections.6 This discrepancy might have occurred because peritonsillar abscesses were excluded from our study, in contrast to Wang's study that included 61 peritonsillar abscesses in 196 patients.6 Chen et al reported that patients with an underlying disease, neck swelling, and delayed time had a positive correlation with complicated deep neck infections, in which 18 cases resulted in lethal complications among the 214 deep neck infection patients.27
In this study, the longest duration of hospitalization was 70 days. A 1-year old female patient was brought to the hospital with dyspnea from acute suppurative infection of the pre-existing 3rd or 4th branchial cleft cyst. An emergency tracheotomy and an incision and drainage were performed. There was a recurrence of the infection three times throughout the hospitalization. However, the patient was discharged after the infection was controlled. In the present study, the duration of hospitalization appeared to be longer than is usually the case. This was most likely because, in general, the authors only discharged patients after the infections were completely controlled.
The most dangerous complications included descending mediastinitis, airway obstruction, and vascular rupture. In this study, 14 cases had descending mediastinitis. Most of these patients were older and had mixed space infections. Four cases with mediastinitis also had sepsis. Three of them died of multi-organ failure related to septic shock and had concurrent DM as a systemic disease. The remaining 11 patients with mediastinitis recovered with close observation and effective intravenous antibiotics after surgical drainage. The causative organism of the mediastinitis varied depending on the origin, but in the majority cases, the flora were a mix of both aerobic and anaerobic bacteria.14 β-Hemolytic Streptococcus was the most commonly found pathogen because of the high incidence of odontogenic infections.28 In this study, α-hemolytic Streptococcus was the most commonly found bacteria in patients with mediastinitis (33.3%, 3 of 9 positive cultures). Upper airway obstruction was noted in 9 cases, and an emergent tracheotomy was performed in 6 (66.7%) of them. Endotracheal intubation is not recommended because it may further jeopardize the already compromised airway. There were 6 patients with sepsis. Three of them recovered following a high-dose of intravenous antibiotics and surgical drainage, and the remaining 3 patients died of septic shock (all of them had DM as was mentioned previously). The mortality rate in our study was 1.9%, which was similar to that of some previous reports.6,8,9,29 This suggests that most patients will have a good prognosis if they are managed properly.
Complications of deep neck infections are still potentially fatal, and that is why we recommend that high-risk groups, such as diabetic patients and/or patients with more than two involved spaces, should be more closely monitored throughout their hospitalization.



 XML Download
XML Download