

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Transrectal ultrasound-guided prostate biopsy (TRUS-Bx) is a standard test for the preoperative diagnosis of prostate cancer and is currently performed widely by radiologists and urologists. In a study of urologists in the United Kingdom, Lee et al. (1) reported numerous differences in the number of biopsy cores, protocols for prebiopsy antibiotic prophylaxis, prebiopsy enemas, and local anesthesia methods among institutions and physicians. In addition, 68% of doctors believe that their training for TRUS-Bx is insufficient (1). In Korea, 12-core biopsy is thought to be widespread at present, but there are variations among operators with respect to the local anesthesia method, prebiopsy antibiotic use, opioid use, and other aspects during TRUS-Bx. However, guidelines for the aforementioned subjects do not yet exist. In the meeting of the Korean Society of Urogenital Radiology (KSUR) in May 2018, the members of the KSUR discussed the actual situations and opinions of the members on topics such as patient preparation and the medicines and methods used for local anesthesia. In this brief article, a consensus report of the aforementioned discussion will be presented with a review of the related literature.
MATERIALS AND METHODS
Composition of the Clinical Guideline Development Group
The KSUR convened a subcommittee consisting of one committee chief and two secretaries for guideline development in 2017. All KSUR members were included as official members of the committee.
Topic Refinement and the KSUR Survey
The subcommittee created several preliminary questionnaires and surveyed the members who attended the regular KSUR monthly meeting in May 2018. Based on these results and feedback, the final questionnaire items were confirmed through discussion with the subcommittee chairman, secretaries, and KSUR president. The survey was conducted using the “Naver Form” survey platform (https://office.naver.com as “Naver form” official site, http://naver.me/50qC8iGw as our survey page [in Korean]) on January 7, 2019, through January 24, 2019, and responses were solicited from the 90 members registered on the KSUR mailing list as of 2018 (Supplementary Materials).
Database and Literature Search
A comprehensive database search was performed by the subcommittee using the Medline database (accessed at PubMed https://www.ncbi.nlm.nih.gov/pubmed) between January 1, 2008 and December 31, 2017. The keywords that were used for the database search were “prostate biopsy,” “anticoagulant,” “antiplatelet,” “enema,” “opioid,” “antimicrobial,” “antimicrobial prophylaxis,” “local anesthesia,” “pain control,” “periprostatic neurovascular bundle block,” “lidocaine gel,” “biopsy core,” “needle gauge,” and “needle throw” in combination with publication-type keywords such as “guideline[Publication Type],” “practice guideline[Publication Type],” and “meta-analysis[Publication Type]” or title keywords such as “recommendation*[Title],” “standard*[Title],” and “guideline*[Title].”
Evaluation of the Literature
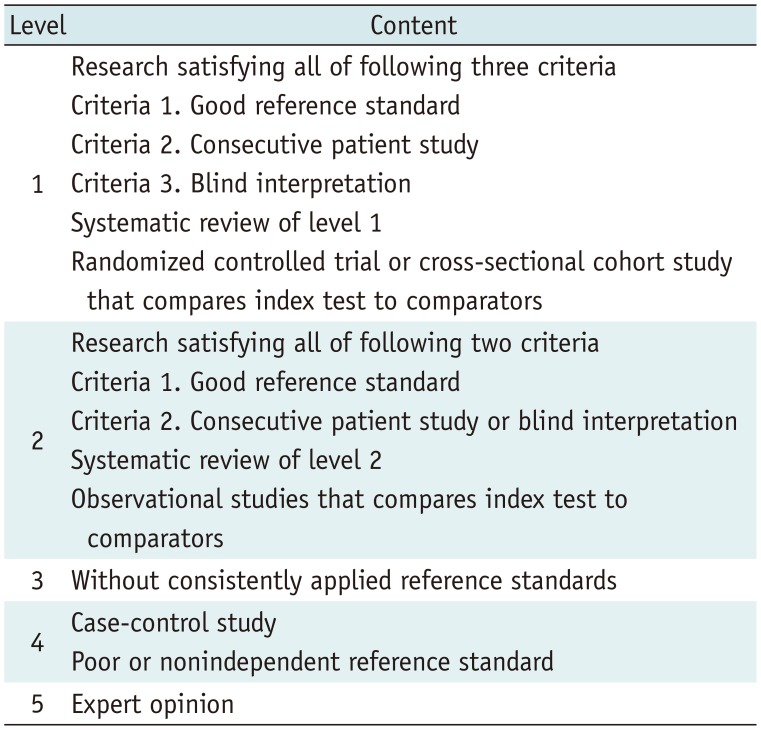
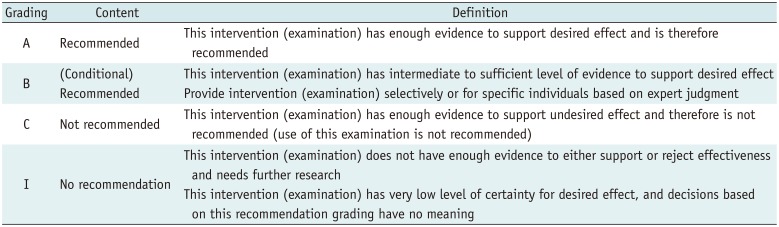
The subcommittee graded the evidence and classified the strength of the recommendation for each statement. The level of evidence grading and strength of recommendation grading were based on the 2016 Korean evidence-based clinical imaging guidelines by the Korean Society of Radiology and National Evidence-based Healthcare Collaborating Agency (2) (Tables 1, 2).
Consensus Achievement
The Delphi method was used for formal consensus in accordance with previously published guidelines (234). Twenty-six council members of the KSUR, including some of the subcommittee members, were asked to provide their level of agreement with each draft recommendation using a voting scale of 1–9 during the regular monthly meeting of the KSUR in March 2019 (where 1 denoted strong disagreement and 9 denoted strong agreement). Each voting score was allocated to one of three groups: 1–3 (disagreement), 4–6 (neutrality), and 7–9 (agreement). Consensus was defined as ≥ 75% of participants providing a score within the 7–9 range (agreement).
Summary of Literature Review with Consensus Statements
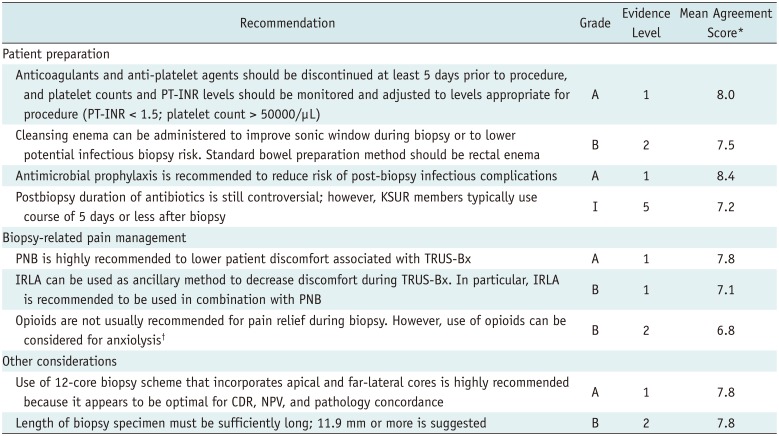
The following recommendations for patient preparation, standard technique, and biopsy-related pain management during TRUS-Bx are summarized in Table 3.
Patient Preparation
Anticoagulation: Stop or Continue before Biopsy?
Bleeding appears as hematuria, rectal bleeding, or hematospermia, and is a common complication of TRUS-Bx; bleeding has been reported in as many as 84% of patients who undergo TRUS-Bx (5). Thus, antiplatelet medications (aspirin, clopidogrel, nonsteroidal anti-inflammatory drugs [NSAIDS], and so on) and anticoagulation medications (heparin, warfarin, and so on) are generally required to be administered before TRUS-Bx to lower the risk of bleeding complications (6). The Canadian Urologic Association guideline on prostate biopsy methodology recommends that antiplatelet agents be stopped 1 to 2 weeks before TRUS-Bx and that anticoagulants be stopped 4 to 5 days prior (6). The Society of Interventional Radiology Consensus guideline for Periprocedural Management of Coagulation Status and Hemostasis Risk in Percutaneous Image-guided Interventions (SIR guidelines) (78) stratifies percutaneous interventional procedures into three categories according to the risk of bleeding, difficulty of detection, and control of bleeding: Category 1, procedures with a low risk of bleeding or where any bleeding is easily detected and controllable; Category 2, procedures with a moderate risk of bleeding; and Category 3, procedures with a significant risk of bleeding that is difficult to detect and control. Most intra- or retroperitoneal biopsies are classified as Category 2 according to SIR guidelines, and TRUS-Bx may also be classified in this category. The SIR guidelines suggest a 5-day course of regular-dose aspirin, clopidogrel, and warfarin before Category 2 procedures with confirmation that the PT-INR is under 1.5 and the platelet count is over 50000/µL (or correction to these values).
Patients who continue taking low-dose aspirin without interruption do not show a significant increase in hemorrhage or hematuria after TRUS-Bx (910). For warfarin, no statistically significant difference has been reported in the severity of postbiopsy bleeding between patients who were continuously administered before and after biopsy and those who discontinued the drug (11). However, this study had limitations, including its nonrandomized design; variability in biopsy type (patients undergoing either 6- or 4-core biopsies); the possibility of life-threatening hemorrhagic complications that may have been missed due to the small sample size; the potential for recall bias, as complications were entered retrospectively 10 days after the biopsy; and the inclusion of patients on warfarin, which may have led to an underestimation of the severity of the hemorrhagic complications (6). A randomized prospective trial revealed that continuing low-dose aspirin in men undergoing TRUS-Bx did not increase the incidence of mild bleeding complications, although it prolonged the duration of self-limiting hematuria and rectal bleeding; thus, its effect on severe bleeding must be evaluated further (12). Therefore, there is a risk to not stopping the anticoagulant or antiplatelet based on the above studies.
All KSUR members who responded to the questionnaire stopped anticoagulants before TRUS-Bx. Approximately 76% (22 of 29) of the responding members ceased anticoagulants 1 week before the procedure. Similarly, almost all respondents except one doctor stopped antiplatelet drugs before TRUS-Bx. Most respondents (86%, 25 of 29) paused the antiplatelet drugs 1 week before the procedure.
Recommendation
Before TRUS-Bx, anticoagulants and anti-platelet agents should be discontinued at least 5 days prior to the procedure, and platelet counts and PT-INR levels should be monitored and adjusted to levels appropriate for the procedure (PT-INR < 1.5; platelet count > 50000/µL).
Cleansing Enema
The main effect of the prebiopsy glycerin enema is emptying the stool from the rectum to improve the sonic window and prevent unnecessary shadowing (6). There is still controversy regarding the effectiveness of enema in preventing infection after biopsy. The incidence of postbiopsy bacteremia is lower in patients given an enema than in those who received no enema, independent of antibiotic administration; however, the bacteremia is asymptomatic (13). Carey and Korman (14) reported that the prebiopsy enema was not of significant benefit and only increased the cost and inconvenience to the patient. However, several published studies subsequently reported that prebiopsy enema could reduce infectious side effects (151617). Mechanical bowel preparation, such as with polyethylene glycol (PEG) solution intake, has an effect of lowering infectious side effects similar to that of a glycerin enema; however, patients considered the PEG preparation to be less comfortable (18).
All members of the KSUR who responded to the questionnaire administered an enema just before TRUS-Bx.
Recommendation
There is no strong evidence to recommend for or against the use of an enema before TRUS-Bx; however, an enema can be administered to improve the sonic window during the biopsy or to lower the potential infectious biopsy risk. The standard bowel preparation method should be rectal enema.
Antimicrobial Prophylaxis
Antimicrobial prophylaxis reduces the risk of bacteriuria, bacteremia, and clinical infections after TRUS-Bx (1920). Prophylactic antibiotic therapy for 1 day or even single-dose prophylactic antibiotic therapy is known to lower the risk of infectious complications to 1% or less (2122). Fluoroquinolone and first-, second-, and third-generation cephalosporins are recommended for TRUS-Bx, and prophylactic antibiotics should be given 1–2 hours before the procedure (192023). The administration route (oral, intramuscular, or intravenous) does not influence the effect of the antibiotics. The postbiopsy duration of antibiotics is still controversial (6). A retrospective multicenter study (24) reported that a combination of single-dose gentamicin intramuscular injection before biopsy and three-day levofloxacin oral administration after biopsy reduced the infectious complication rate by up to 90% compared to the administration of postbiopsy antibiotics only.
Most KSUR members who responded to the questionnaire (86%, 25 of 29) used antibiotic prophylaxis before TRUS-Bx. The most frequently used antibiotics were third-generation cephalosporins, followed by quinolones and second-generation cephalosporins. Postbiopsy antibiotic use was also surveyed, and almost all members who responded (90%, 26 of 29) administered antibiotics up to 1 week after the procedure. One member who did not use prophylactic antibiotics administered postbiopsy antibiotics (3rd generation cephalosporins) 1 week after the biopsy.
Recommendation
Antimicrobial prophylaxis is recommended to reduce the risk of postbiopsy infectious complications.
The postbiopsy duration of antibiotics is still controversial; however, KSUR members typically use a course of 5 days or less after biopsy.
Biopsy-Related Pain Management
Periprostatic Neurovascular Bundle Block
The factors affecting pain in TRUS-Bx patients vary, and the intensity of the pain is known to be influenced by the size of the ultrasound probe and the number of biopsies.
The pain that occurs when an ultrasonic transducer is inserted is known as somatic pain when the anal canal under the dentate line, which has a rich sensory nerve distribution, is expanded by the transducer. The rectal mucosa is insensitive to pain, but the prostate capsule and prostate parenchyma are very sensitive to pain, which is known to spread through the periprostatic neurovascular bundle.
Periprostatic neurovascular bundle block (PNB) was usually performed using a Chiba needle or a long spinal needle (7-inch, 22-gauge), with direct injection of 5 mL of 1–2% lidocaine in the region of the prostatic vascular pedicle at the base of the prostate just lateral to the junction between the prostate and seminal vesicle (24). To date, PNB has been the best proven method for reducing pain in TRUS-Bx and has been shown to reduce pain (with statistical significance) in a series of meta-analyses comparing non-anesthetic control and placebo (2526). PNB has also been shown to provide similar pain control compared to sedoanalgesia (intravenous midazolam and fentanyl) or intravenous tramadol. However, PNB is a preferable method in TRUS-Bx since it is much more practical in outpatient clinics and relatively free from the side effects of midazolam, fentanyl, or tramadol.
Most KSUR members who responded to the questionnaire adopted PNB for pain management during TRUS-Bx (79%, 23 of 29).
Recommendation
PNB is highly recommended to lower patient discomfort associated with TRUS-Bx.
Intrarectal Lidocaine Gel Application
The main function of the gel applied to the anal canal during TRUS-Bx is to reduce the pain caused by the expansion of the anal canal by enhancing anal compliance and lowering the friction between the probe and anal canal. Lidocaine-containing gels are expected to reduce somatic pain more effectively by dampening the sensation of the anal canal and by adding local anesthetic effects to the surrounding prostate capsule and parenchyma via absorption through the rectal mucosa (26). However, the effects of intrarectal lidocaine gel application (IRLA) have been reported to be widely variable; of 17 randomized controlled trials, 12 reported no difference in pain relief between conventional ultrasound gel and lidocaine gel, and 5 described IRLA as reducing the pain in TRUS-Bx, relative to the effect of conventional gel (27). In comparison with IRLA, PNB is known to have the same effect (24) and shows more effective pain relief (2526272829). In particular, the use of both PNB and IRLA simultaneously is described as being more effective than single treatment (25).
Four of 29 (14%) KSUR members who responded to the questionnaire used IRLA only, and 6 doctors among the respondents used a combination of PNB and IRLA for pain management during TRUS-Bx (21%, 6 of 29).
Recommendation
IRLA can be used as an ancillary method to decrease discomfort during TRUS-Bx. In particular, IRLA is recommended to be used in combination with PNB.
Opioid Analogues
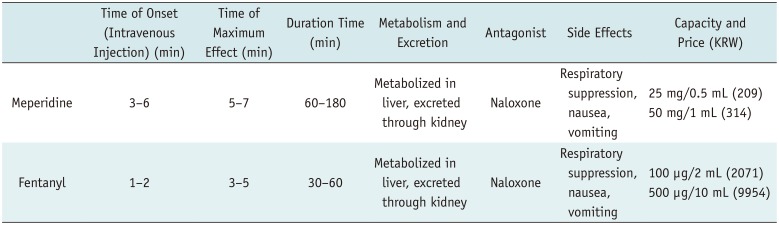
Among opioid analogues, meperidine (pethidine) and fentanyl are commonly used in Korea. Generally, fentanyl is more effective and faster-acting than meperidine, but its effective duration is shorter, and it is more expensive. Among side effects, respiratory depression, nausea, and vomiting show similar frequencies between the two drugs, but the rate of cardiovascular side effects is slightly higher for meperidine. Simple comparisons are listed in Table 4.
Opioid analogues are mainly used as an adjunct to PNB because narcotic analgesics reduce anxiety (anxiolytics) (28). There is no evidence that the analgesic effect of opioid analogues is superior to that of PNBs when injected intravenously, and the analgesic effects of opioids are inferior to those of PNBs when injected intramuscularly (272930). Although fentanyl offers no additional benefit over PNB monotherapy when used with PNB, it should be considered for reducing patient anxiety (28).
Only two KSUR members (6.8%) who responded to the questionnaire used opioid analgesics, and all used opioids as a complement to PNB and/or IRLA. No respondent used opioids as the sole method of pain management during TRUS-Bx.
Recommendation
Opioids such as meperidine or fentanyl are not usually recommended for pain relief during biopsy. However, the use of opioids can be considered for anxiolysis. This recommendation may be controversial since a consensus was not fully achieved (% of respondents with agreement score ≥ 7: 73.1%).
Other Considerations
Number of Biopsy Cores and Length and Diameter of the Biopsy Needle
According to the American Urologic Association white paper (31) and the Canadian Urological Association on Prostate Biopsy Methodology (5), a 12-core biopsy scheme including the prostate apex and bilateral far lateral peripheral zones is recommended as the standard TRUS-Bx protocol. In comparison with the standard sextant biopsy, the 12-core biopsy scheme increases the cancer detection rate (CDR), increases the negative predictive value (NPV) to lower the ratio of recurrent biopsy, and shows a similar rate for diagnosing cancer (i.e., the difference in rate is not clinically significant). These reports also indicated that there are no additional benefits in terms of CDR and NPV to performing biopsy with more than 12 cores.
The size of the biopsy needle is usually 18-gauge, and there are studies reporting that an increase in the size of the core to a 16-gauge does not cause any side effects or differences in CDR (32). The length of the core has a great effect on the CDR (3233), and one study recommended that the length of the core be greater than 11.9 mm (33). Therefore, there could be no significant difference in CDR between the 16-mm and 22-mm biopsy needles. However, the aforementioned studies compared the length of cores obtained by a fixed single-length biopsy needle, and there are no studies comparing CDR or complication rates among different biopsy needle gauges and lengths. Further studies are needed on this issue.
Most KSUR members who responded to the questionnaire (90%, 26 from 29) chose the 12-core method for TRUS-Bx. One respondent used the 10-core method. Two respondents chose ‘others’; one answered that he or she obtained 10 or 12 cores depending on the situation, and the other responded that he or she obtained an additional 2 cores from the transitional zone, making 14 cores in total.
The most commonly used gauge and throw combination for the biopsy gun was the 18G 22-mm (15 of 29, 51.7%) needle, followed by the 18G 16-mm needle and 16G 16-mm biopsy needle. Four respondents chose “others” and left a comment stating “mixed use of 18G 16-mm and 18G 22-mm according to prostate size.”
Recommendation
The use of a 12-core biopsy scheme that incorporates apical and far-lateral cores is highly recommended because it appears to be optimal for CDR, NPV, and pathology concordance.
Although the gauge and length of the biopsy needle seem irrelevant in CDR, the length of the biopsy specimen must be sufficiently long; 11.9 mm or more is suggested.
CONCLUSION
The KSUR guideline development subcommittee presented a consensus statement with a literature review for topics including patient preparation, pain management, and biopsy scheme planning for TRUS-Bx. We recommend the 12-core biopsy scheme with the PNB ± IRLA local anesthesia method as the standard protocol for TRUS-Bx. Anticoagulants and antiplatelet agents should be discontinued at least 5 days prior to the procedure, and antibiotic prophylaxis is highly recommended to limit infectious complications. Glycerin cleansing enemas and administration of opioid analogues before the procedure could be helpful in some situations. The choice of gauge and length of the biopsy needle is dependent on the practitioners' situation and preferences.
 XML Download
XML Download