

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ultrasonography (US) is a standard tool used to evaluate thyroid nodules at follow-up assessments. These nodules may remain stable or may show changes in size at follow-up (12). Thyroid nodules that have decreased in size are usually benign and have various names, such as degenerating nodules (DNs) (34), collapsing benign cystic nodules (5), mummified thyroid syndrome (67), and vanishing tumors (89). Among these, DNs have been mainly described as benign thyroid nodules (34567101112); however, they are also related to malignant thyroid cancer (913), which can be induced spontaneously or after fine-needle aspiration (FNA) or core-needle biopsy (CNB) (345678910111213).
DNs may sometimes show suspicious US features, which may cause confusion to many doctors despite a reduction in their size. DNs that show a size reduction on follow-up US are identified as benign rather than malignant; however, these nodules may occasionally appear without any previous US findings. Furthermore, DNs frequently show suspicious US features and even FNA may reveal variable cytological results, such as benign findings, atypia of undetermined significance (14), or nondiagnostic results (1516). In such cases with US-cytology discordance (i.e., cytologically benign nodules with suspicious US features), the false-negative rate of FNA is nonnegligible (1718). The incidence of US-cytology discordant nodules is 2.8–19.7% (19), and guidelines recommend repeated US-guided FNA in such cases (202122). One of the main causes of US-cytology discordant nodules is DNs.
The histological findings for DNs show a decrease in or absence of follicular cells and secondary reactive or degenerative changes such as hemorrhage, degeneration, infarction, fibrosis, vascular thrombosis/proliferation, stromal cell proliferation, and squamous metaplasia (10). These changes include worrisome histological features such as cytologic atypia, architectural atypia, and necrosis, which often lead to issues in the cytological interpretation of FNA specimens.
These US-cytology discordant nodules may lead to unnecessary repeated biopsies or diagnostic surgical procedures. Therefore, in this review, we will discuss the mechanism and US-pathology correlations of DNs to improve their differential diagnosis and management strategies.
Mechanism of Degeneration of Thyroid Nodules
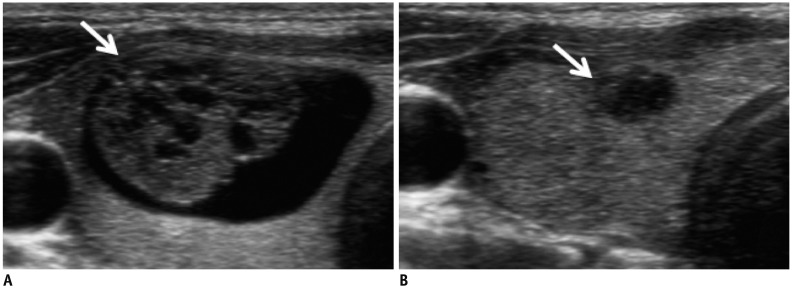
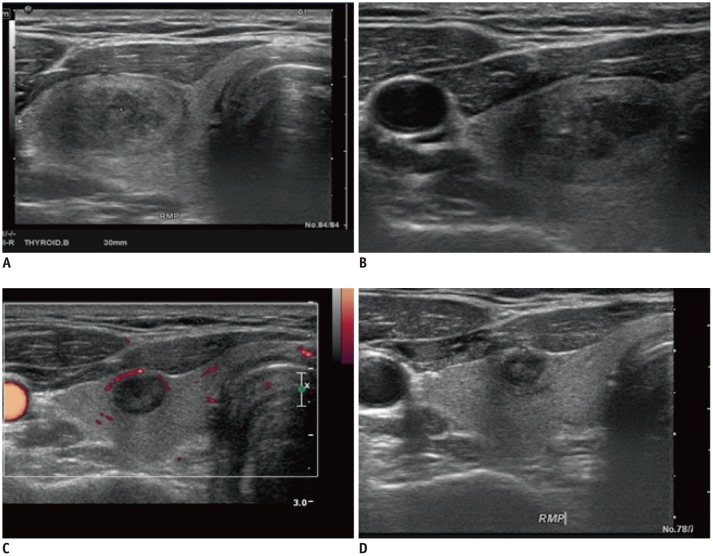
Studies on the natural history of benign thyroid nodules have shown that cystic or predominantly cystic nodules are more likely to decrease in size than solid nodules (123). In cystic or predominantly cystic thyroid nodules, the cystic portion can be spontaneously absorbed, desiccated, or crumpled over time. In solid nodules, iatrogenic injury by FNA/CNB can cause venous thrombosis and/or internal bleeding, which are mechanisms that potentially lead to nodule degeneration (7101124). Intranodular hemorrhage (spontaneous or FNA-induced hemorrhage) compressing peripheral nodule tissues is believed to be one of the initial mechanisms of DN development (Fig. 1). Hemorrhage usually occurs in thyroid nodules and may be associated with their rich blood supply. The prevalence of hemorrhage within thyroid nodules after biopsy is reportedly between 26.5% and 93.3% (102526), whereas even in patients who do not undergo FNA, the hemorrhage rate is still as high as 33.3% (10). An impaired blood supply due to venous thrombosis and hematoma regression may explain the further shrinkage and infarction that occurs later in the degradation process (7101124).
The Pathologic Spectrum of DNs
The considerable variation in the histological changes in DNs makes diagnosis difficult. Surgical specimens of DNs are divided into an acute stage and a chronic stage based on the interval between FNA and surgical excision of the lesion (11). LiVolsi and Merino (11) stressed the importance of histological changes in surgical specimens by proposing the “Worrisome Histologic Alterations Following Fine-Needle Aspiration of the Thyroid” (WHAFFT) syndrome. Symptoms of WHAFFT syndrome include acute changes such as hemorrhage, granulation tissue, mitosis, granulomas, capsular distortion (pseudoinvasion), and infarction and chronic changes such as fibrosis, metaplasia, infarction, cyst formation, papillary degeneration, papillary endothelial proliferation, and calcification (11). Hemorrhage and granulated tissues are the main histological changes observed within 3 weeks after FNA, which is the so-called acute stage. The chronic stage typically begins one month after FNA, during which fibrosis and capsule distortion are the dominant changes (1011).
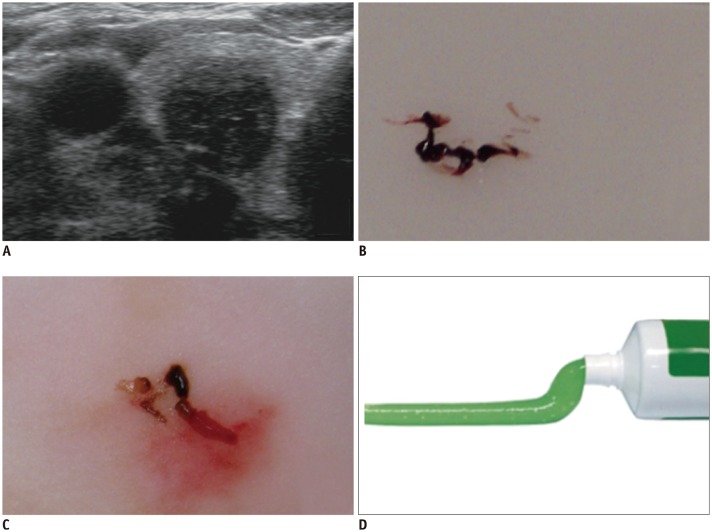
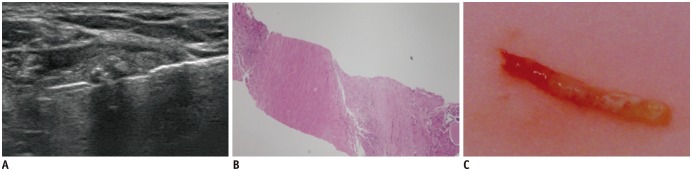
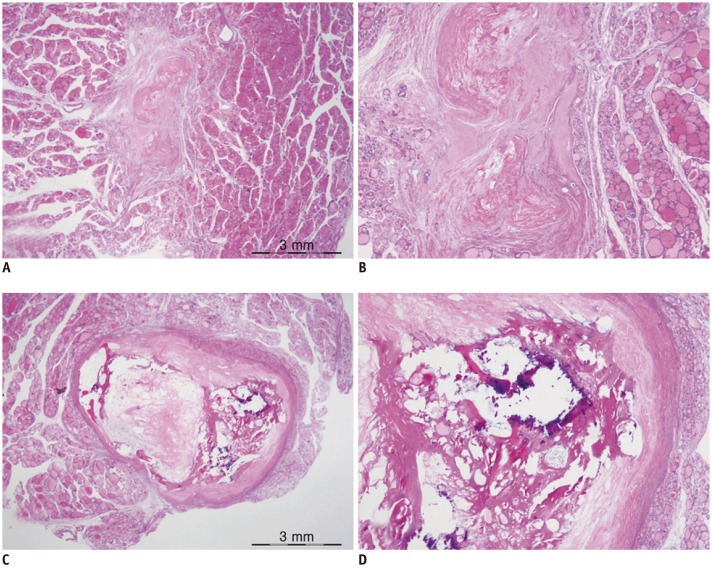
Biopsy specimens show different gross features in FNA and CNB according to the degeneration stage. In the early stage, hemorrhage appears as a reddish toothpaste-like muddy material on FNA and CNB (Fig. 2). Cytopathological characteristics include numerous degenerated red blood cells, few hemosiderin-laden macrophages, and a few equivocal microcalcifications. In the second stage of hemorrhage regression, CNB specimens show a brown bread-like material containing diffuse stromal fibrosis with chronic inflammation and histiocyte deposition (Fig. 3). Whitish hard material can be seen on the CNB specimen until the chronic stage, at which dense stromal fibrosis with/without calcifications can be observed (Fig. 4). These cases usually show no histological evidence of malignancy, which is key to diagnosing DNs as benign lesions; however, atypical cells occasionally develop, resulting in atypia of undetermined significance on cytopathological assessments. Importantly, in the chronic stage, nondiagnostic results with FNA specimens are common because these specimens contain few follicular cells, and the consistency of DNs becomes harder due to fibrosis.
Differential Diagnosis on US
Serial US Changes
Despite the gradual size reduction of DNs, their worrisome histological alterations usually lead to US features mimicking malignancy (2728293031), upgrading their thyroid imaging reporting and data system (Korean-TIRADS) category (61032).
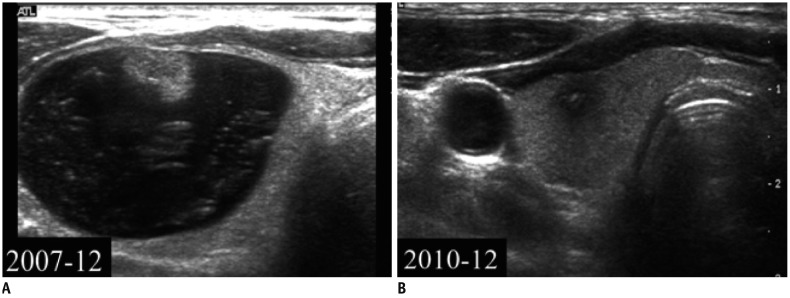
Lee et al. (4) reported that all cystic portions in nodules (8/8) disappeared and were replaced with solid content (Fig. 5). The degree of malignant US features (i.e., spiculated margin and marked hypoechogenicity) increased during the follow-up period (6% vs. 13% and 19% vs. 38%, respectively) (Fig. 6). Micro- and macrocalcifications also became more prevalent in the final US findings than in the initial images (19% vs. 32%) (4).
Fibrosis is closely related to hypoechogenicity on US (3272833). The relatively high incidence of intranodular fibrosis in DNs (66.0–100%) may explain the suspicious US findings (410). Calcification, which is another malignant US feature, usually develops in 17.9–25.0% of DNs within 2 months after FNA (3410). However, colloid material can mimic calcifications after degeneration. More importantly, considering the similar incidences of the appearance of microcalcifications (p = 0.734) and macrocalcifications (p = 0.538) in DN and papillary thyroid carcinoma (PTC) (5), the presence of calcifications is problematic. Collapse (428) and capsular distortion (pseudoinvasion) may contribute to ill-defined margins (10). Capsular distortion was found in 7.6–14% of nodules after FNA (10). Similarly, the taller-than-wide shape of DNs correlates with asymmetric fibrous traction, especially transverse shrinking (7).
Differentiation of DNs from Thyroid Cancer on US
Several studies have tried to differentiate DNs from thyroid carcinoma on US. Significant differences were found between DNs and PTC in shape (ovoid-to-round vs. taller-than-wide), margins (ill-defined vs. spiculated), low-echoic halo, and inner isoechoic rim (5343536373839); however, these findings overlap in both diseases.
Among these US features, inner isoechoic rim and low-echoic halo showed the highest diagnostic accuracies with acceptable negative predictive values (5). An inner isoechoic rim was defined as a thin continuous isoechoic rim along more than half of the inner margin of a nodule, which may correspond with the intact solid wall of preexisting cystic nodules (5). Interestingly, a tumor capsule or a fibrotic pseudocapsule that is compressed in normal thyroid tissue or chronic inflammatory infiltrates can manifest as a low-echoic halo (3040), which is defined as a hypoechoic rim surrounding the outer margin of a nodule.
Posterior US shadowing was also reported as a useful US feature for a correct final diagnosis; this shadowing is associated with an uneven interface due to shrinkage encapsulation or peripheral fibrosis (3041). However, the lack of vasculature does not definitively distinguish DNs from PTC because a strong stromal desmoid reaction can suppress angiogenesis (42).
Management of DNs
Serial US Images
Serial US images and findings, including thyroid nodule volume, echotexture, and echogenicity obtained from a comparison with previous US results, may warrant US follow-up instead of an unnecessary repeated biopsy or diagnostic surgery (671043).
However, genuine PTCs rarely exhibit volume stability and can even shrink over time (44). In addition to these rare cases, when the patient's history is unavailable, biopsy should be recommended.
Combination of US Features and Biopsy Characteristics
FNA is an effective and accurate technique for diagnosing thyroid nodules. However, DNs tend to present benign results, atypia of undetermined significance, or nondiagnostic results upon FNA because of the histological nature of scarce follicular cells and hard fibrosis. Moreover, US-cytology discordant nodules, defined by benign cytological findings but suspiciously malignant US findings, have a markedly increased risk of malignancy of 13.6–56.6% (102021314546). Given the above conditions, even if the FNA results are benign, repeat FNA or diagnostic surgery may still be necessary due to the malignant US features.
Recent studies seem to support the assumption that CNB is more useful than repeat FNA for avoiding inappropriate diagnostic surgery in patients with initial nondiagnostic results (1516) or atypia of undetermined significance (4748) and discordant US-cytology results (3). CNB of solid nodules yields a high level of diagnostic accuracy (97–98%) and has a lower rate of inconclusive or nondiagnostic results (3.2–7.2%) than FNA (349505152). Yeon et al. (15) revealed that diagnostic surgery can be prevented by CNB in 96% of patients with two series of nondiagnostic FNA results.
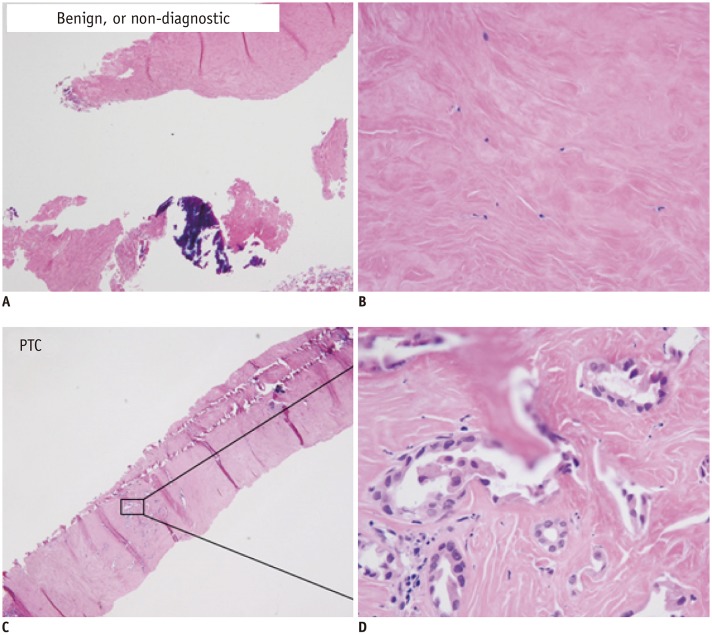
The correlation between pathologic characteristics and US findings for DNs may explain the utility of CNB for diagnosis (4). There are relatively few follicular cells in the center of a DN, whereas plenty of follicular cells are located adjacent to the peripheral area (Fig. 7) (4). Utilizing the central region as a target may increase the nondiagnostic risk of FNA. In contrast, CNB specimens containing both the center and peripheral regions may offer significantly enhanced diagnostic value (4). Therefore, when a CNB specimen shows fibrosis and hemorrhage with scarce follicular cells in the corresponding suspicious area within DNs, such a nodule can be more confidently considered to be a benign lesion (Fig. 8).
The risk of malignant discordant US-CNB nodules was lower (3.6–5.5%) than that of malignant discordant US-FNA nodules (13.6–56.6%) (29). This finding suggests that rebiopsy or diagnostic surgery for US-CNB discordant thyroid nodules should be carefully considered. Caution should be taken because CNB may mistarget the diagnostic portion if it is limited to one or two CNB sessions (29); malignant nodules may also spontaneously degenerate.
CONCLUSION
Most DNs are benign, but they frequently show suspicious US features. An understanding of the mechanism, US findings, pathological findings, and serial changes in DNs can minimize unnecessary procedures for patients. Some US features, including ovoid-to-round shape, ill-defined borders, low-echoic halo, inner isoechoic rim, and posterior shadowing, may help diagnose DNs. Follow-up US should be recommended first in cases showing nodule shrinkage and changes in echotexture and echogenicity on serial US images. For patients whose history is unavailable or whose nodules remain highly suspicious, biopsy should also be recommended. FNA may be the first choice, but DNs tend to present benign results, atypia of undetermined significance, or nondiagnostic results in FNA because of the histological nature of scarce follicular cells and hard fibrosis. Given the above conditions, it would be more useful to perform CNB instead of repeat FNA to avoid unnecessary diagnostic surgery.

 XML Download
XML Download