

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pancreaticoduodenectomy (PD) is the main treatment for periampullary and pancreatic head cancers (123). Postoperative mortality after PD has decreased significantly over the past decade (45). However, the incidence of morbidity still remains high, ranging from 16% to 41% (6). Postoperative pancreatic fistula (PF) is a major complication as well as a major factor contributing to increased morbidity, with incidences ranging from 5% to 40% (678910). Pancreatic softness is the most frequently reported risk factor for PF. The presence of a fatty pancreas on microscopic pathological examination constitutes a risk factor for PF (9111213). Therefore, evaluating fatty infiltration of the pancreas on preoperative imaging may be useful for predicting PF and considering alternative treatment strategies (14).
Mean computed tomography attenuation in Hounsfield unit (CTHU) on nonenhanced images can reflect pancreatic fatty changes, and a low pancreatic attenuation index is strongly associated with PF (15). However, since the mean CTHU value represents an average value of all tissues, including fat, water, and pancreatic parenchyma, it is limited in terms of assessing the amount of fat in the pancreatic parenchyma. Recently, commercial three-dimensional (3D) imaging analysis software has made it possible to classify CTHU values in regions of interest (ROIs) within a specific range of HU values (16). We hypothesized that the negative CTHU fraction in the pancreatic parenchymal ROI represented the amount of fat in the pancreatic parenchyma. The purpose of this study was to evaluate the effectiveness of CTHU histogram analysis (HUHA) in predicting PF occurrence and pancreatic softness.
MATERIALS AND METHODS
Patients
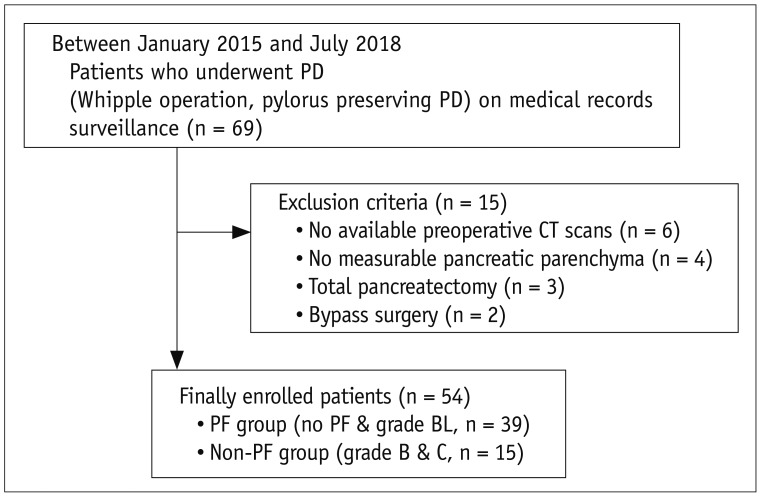
This retrospective study was approved by our Institutional Review Board of Hallym University Sacred Heart Hospital, and informed consent was waived. The study included 69 patients who underwent PD between January 2015 and July 2018 and were selected using “pancreaticoduodenectomy” as the search term in the hospital's electronic medical record system. Only patients with a preoperative CT scan available for review that was taken within 30 days before surgery were included in the study. Of these patients, 15 were excluded due to a lack of available preoperative CT scans (n = 6) or measurable pancreatic parenchyma (n = 4) or having underwent total pancreatectomy (n = 3) or bypass gastrojejunostomy (n = 2) instead of PD. In total, 54 patients (33 males and 21 females; mean age, 65.6 years; age range, 37–89 years) were included (Fig. 1). None of the patients received preoperative chemotherapy or radiation therapy. The clinical laboratory data for each patient were analyzed using previously described methods (1718).
PF Definition, Surgical Procedure, and Texture Analyses
PF was classified according to the 2016 update of the International Study Group on Pancreatic Fistula (ISGPF) as any measurable drainage output from an intraoperatively placed drain, or a postoperatively placed percutaneous drain, on or after postoperative day 3 with an amylase content greater than three times the upper limit of the normal serum amylase level (> 300 U/L). The severity of the fistula was graded as biochemical fistula (BL), B, or C as follows: 1) grade BL represents a transient, asymptomatic fistula with elevated drain amylase levels only, which does not require treatment or deviation from clinical management; 2) grade B represents a symptomatic, clinically apparent fistula requiring diagnostic elevation and therapeutic management, such as percutaneous or endoscopic drainage or an angiographic procedure for bleeding; and 3) grade C represents a severe, clinically significant fistula requiring a major deviation in clinical management, such as reoperation, organ failure, or death (810). Grades B and C are clinically important since they require altered postoperative management and interventions, whereas grade BL only requires observation (1819). Therefore, we combined grades B and C into the clinically significant PF group and grade BL and no PF into the non-PF group.
The texture of the pancreatic parenchyma was assessed as soft or hard by manual palpation by a single surgeon.
CT Acquisition Protocol
All CT images were obtained using one of three scanners, including a 64-slice multidetector CT (MDCT) scanner (Brilliance 64; Philips Healthcare, Cleveland, OH, USA) and two 128-slice MDCT scanners (SOMATOM Definition Edge or SOMATOM Definition Flash; Siemens Healthineers, Forchheim, Germany). Automatic tube voltage selection and current modulation were used for 128-slice MDCT scans, whereas automatic tube current modulation was used for 64-slice MDCT scans. The general scanning parameters were as follows: detector configuration, 64 × 0.6 mm for 64-slice MDCT scans and 128 × 0.6 mm for 128-slice MDCT scans; gantry rotation time of 0.5 seconds for all scanners; tube current, 140–200 mAs; tube voltage, 100 kVp or 120 kVp; slice thickness, 3 mm; reconstruction interval, 3 mm; and filtered back projection. The HUHA and mean CTHU values were measured on pre-contrast CT images to avoid contrast agent effects.
CT Image Analyses
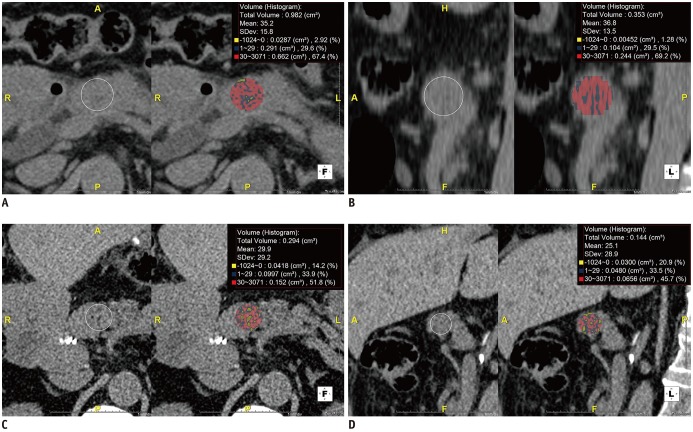
We evaluated the HUHA and mean CTHU values using commercial 3D analysis software (Aquarius iNtuition v4.4.12; TeraRecon, Foster city, CA, USA). The HUHA of the pancreas was evaluated on preoperative pre-contrast CT images. First, all pre-contrast CT images were saved in DICOM format and imported into the commercial 3D analysis software. The imported images were reconstructed as reformatted axial, sagittal, and coronal images. Referring to postoperative CT images, an observer selected one axial image containing the pancreatic parenchyma using the superior mesenteric vein (SMV) as the reference point, which corresponded to the pancreaticojejunostomy site. Following this, a large round ROI was drawn within the pancreatic parenchyma on the selected axial image. The retroperitoneal or peripancreatic fat was carefully excluded from this ROI. Using the 3D analysis software, a corresponding sagittal image was selected, and a round ROI was similarly drawn. The HUHA and mean CTHU values were automatically and simultaneously analyzed. The HUHA value was arbitrarily divided into three categories, comprising HUHA-A ≤ 0 HU, 0 HU < HUHA-B < 30 HU, and HUHA-C ≥ 30 HU. Categories HUHA-A, HUHA-B, and HUHA-C represent the fat, water, and pancreatic parenchyma content within the ROI, respectively. Each HUHA value was calculated as a percentage of the entire area. The axial and sagittal HUHA and mean CTHU values were expressed as average values (Fig. 2).
All data measurements were performed by two observers (i.e., observer 1 with 10 years of abdominal imaging experience and observer 2, a third-year radiology resident). Other risk factors related to PF occurrence were evaluated by one observer. The pancreatic thickness and main pancreatic duct (MPD) diameter were measured at the level of the confluence of the SMV and portal vein. The thickness of the subcutaneous fat adjacent to the umbilicus as well as the thickness of the perirenal fat at the level of the left renal vein were also measured on preoperative CT (611131820).
Statistical Analyses
Inter-observer agreement for the HUHA and mean CTHU measurements was assessed using Bland-Altman plots, and mean differences and 95% limits of agreement (mean difference ± 1.96 × standard deviation) were determined. Independent-samples t tests with or without Welch's test were used to compare quantitative parameters with respect to normal or unequal distributions. Chi-square tests and McNemar's test were used to assess categorical data. A correlation coefficient was calculated to evaluate the relationship between the HUHA values and PF occurrence or pancreatic softness. Predictions of PF occurrence and pancreatic softness were analyzed with receiver operating characteristic (ROC) curves using each HUHA and mean CTHU value. ROC curves were compared using the method of Delong et al. (21), which calculated the exact binomial confidence intervals (CIs) for the areas under the curve (AUCs) (22). Statistical analyses were performed using commercial software (MedCalc Software bvba, Ostend, Belgium). P < 0.05 indicated statistical significance.
RESULTS
Patient Demographics and CT Imaging Features
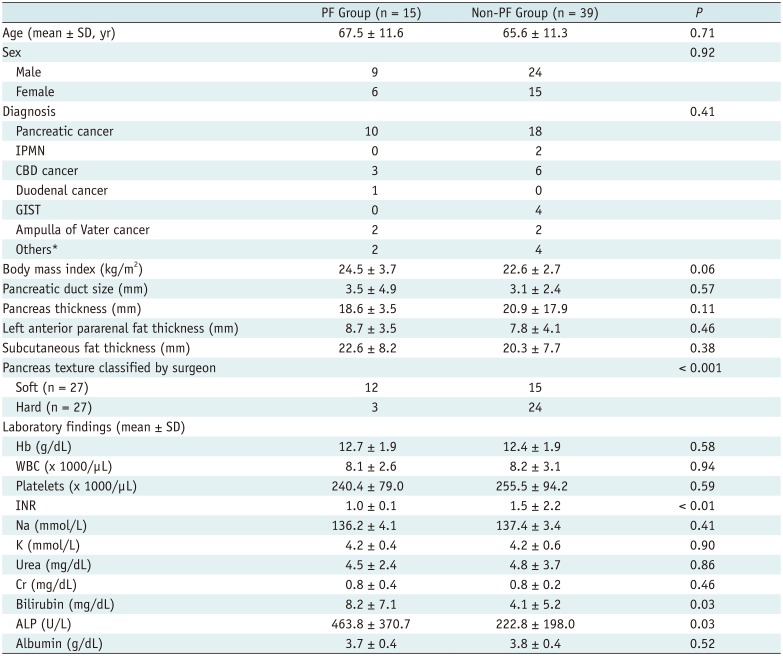
Patient demographics and clinical laboratory results are summarized in Table 1. Twenty-nine patients had no PFs and 10 patients had PFs that were classified as grade BL. Fifteen patients (27.8%) had clinically relevant PFs. All 15 patients with PF had grade B PFs, and no patients had grade C PFs. There were no significant differences between the PF and non-PF groups with respect to age, sex, diagnosis, or body mass index. Lower international normalized ratio (p < 0.01) and higher bilirubin (p = 0.03) and alkaline phosphatase (p = 0.03) levels were associated with PF occurrence. However, no additional blood test results were related to PF occurrence. The other imaging features examined were insignificant. Palpation by a surgeon showed a significant effect for predicting PF (Table 1).
Reliability of HUHA and Mean CTHU Measurements
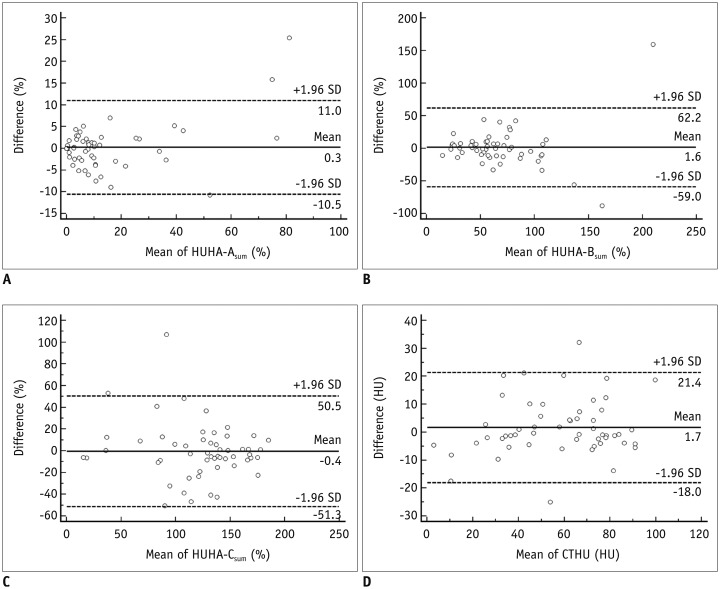
Bland-Altman plots of HUHA and mean CTHU measurements are shown in Figure 3. The mean differences (95% limits of agreement) were 0.3% (−10.5–11.0%) for HUHA-A (Fig. 3A), 1.6% (−59.0–62.2%) for HUHA-B (Fig. 3B), −0.4% (−51.3–50.5%) for HUHA-C (Fig. 3C), and 1.7 HU (−18.0–21.4 HU) for mean CTHU (p > 0.05) (Fig. 3D).
HUHA and Mean CTHU Performance in Predicting PF Occurrence and Pancreatic Softness
The HUHA and mean CTHU values of the PF and non-PF groups are summarized in Tables 2 and 3. PF occurrence correlation analysis showed a strong positive correlation of HUHA-A with PF (r = 0.60; 95% CI, 0.47 to 0.71; p < 0.01). HUHA-B (r = 0.32; 95% CI, 0.18 to 0.51; p < 0.01), HUHA-C (r = −0.39; 95% CI, −0.60 to −0.30; p < 0.01), and mean CTHU (r = −0.27; 95% CI, −0.44 to −0.08; p < 0.01) showed either weak positive or negative correlations with PF. Pancreatic softness correlation analysis showed that HUHA-A (r = 0.51; 95% CI, 0.36 to 0.64; p < 0.01) and HUHA-C (r = −0.47; 95% CI, −0.60 to −0.30; p < 0.01) had moderate correlations with pancreatic softness. HUHA-B (r = 0.36; 95% CI, 0.18 to 0.51; p < 0.01) and mean CTHU (r = −0.27; 95% CI, −0.44 to −0.08; p < 0.01) showed only weak correlations.
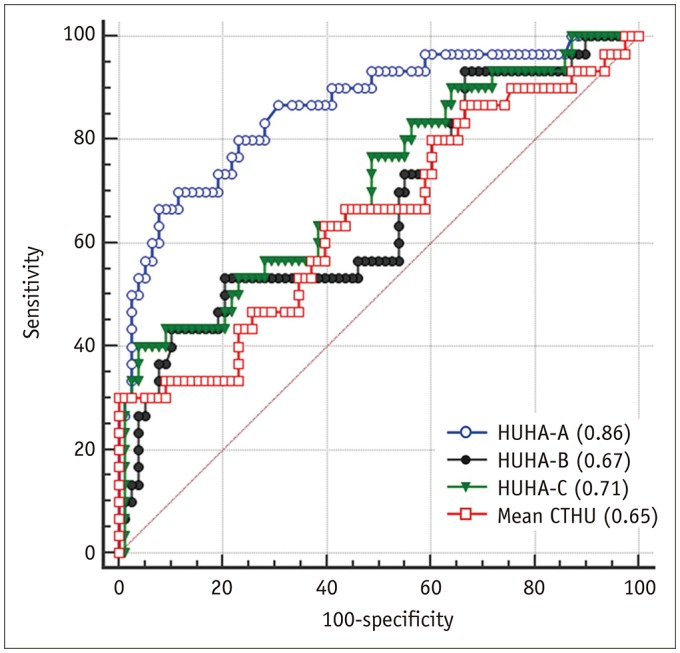
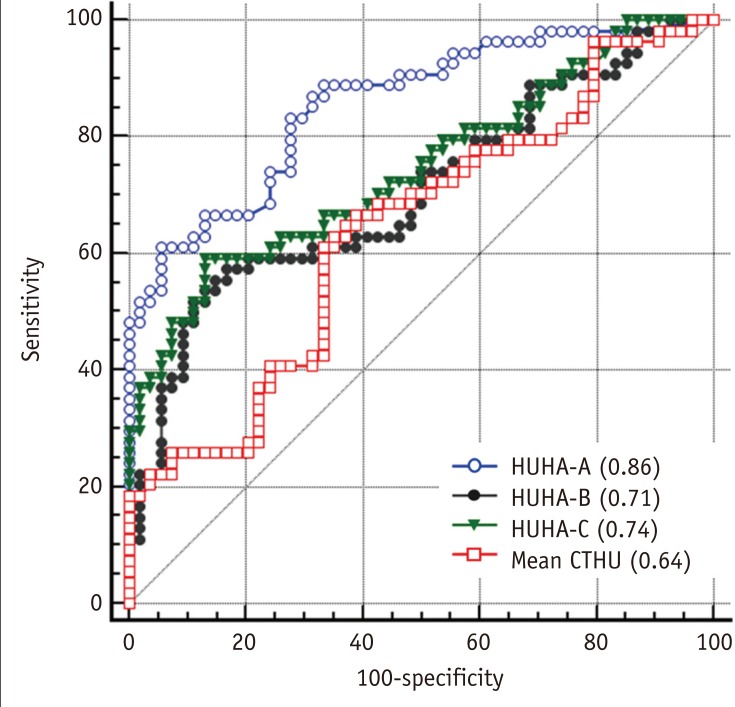
The ROC analysis to predict PF occurrence resulted in AUC values for HUHA-A, HUHA-B, HUHA-C, and mean CTHU of 0.86 (95% CI: 0.78 to 0.92), 0.67 (95% CI: 0.57 to 0.76), 0.71 (95% CI: 0.61 to 0.79), and 0.65 (95% CI: 0.55 to 0.74), respectively. HUHA-A had significantly better PF predictive capabilities compared to the other values (p < 0.01) (Fig. 4). When the 27.8% PF prevalence rate of our study population and a > 7.9% HUHA-A cutoff were applied, the sensitivity and specificity of the HUHA-A value for predicting PF were 66.7% and 92.3%, respectively.
The ROC analysis to predict pancreatic softness resulted in AUC values for HUHA-A, HUHA-B, HUHA-C, and mean CTHU of 0.86 (95% CI: 0.78 to 0.92), 0.71 (95% CI: 0.61 to 0.79), 0.74 (95% CI: 0.65 to 0.82), and 0.64 (95% CI: 0.54 to 0.73), respectively (Fig. 5).
DISCUSSION
Our study demonstrated a strong positive correlation between the HUHA-A value and PF occurrence. Moreover, in the ROC analysis, the HUHA-A value showed good diagnostic performance in predicting PF occurrence. Since we hypothesized that the HUHA-A value represents the distribution of fat in the pancreatic parenchyma, our results suggest that the amount of fat in the pancreatic parenchyma is closely related to PF occurrence. Based on our results, the assessment of the fat content of pancreatic tissue with HUHA may be helpful in predicting PF occurrence and identifying patients with a high risk of developing PF. Additionally, in the ROC curve for pancreatic softness, the HUHA-A value showed a moderate correlation with pancreatic softness and had good predictive performance. As in other reports (141520), the mean CTHU, which is commonly used to analyze CT images, was significantly different between the PF and non-PF groups in our study. However, it showed a weak negative correlation with PF and poor diagnostic accuracy for PF prediction. Fatty changes in the pancreatic parenchyma are indicated by decreased HU values on CT. However, since the mean CTHU value is the average value of all tissues, it has limitations with respect to accurately evaluating fat. Moreover, to use the mean CTHU value to measure fat in the liver or pancreas, a calibration process using spleen or main portal vein attenuation values may be required (15232425). Recent advances in imaging analysis technology have made it possible to analyze the CTHU value for specific HU ranges and calculate the distribution of arbitrarily set HU ranges as a percentage. Specifically, this method can only measure the distribution of negative HU values representing fat content (16). In this study, we assumed that negative HU values represented fat tissue in the pancreas more accurately than the mean CTHU value. Our results suggest that the HUHA value represented the amount of fat within the ROI more accurately than the mean CTHU.
Fatty infiltration of the pancreas and pancreatic softness are considered important risk factors for PF (91113). Pathologically proven fatty changes in the pancreas have been highly correlated with CT and magnetic resonance imaging (MRI) features. Yardimci et al. (15) calculated the pancreatic attenuation index by dividing pancreas density by spleen density. Patients with a lower pancreatic attenuation index developed PF at a significantly higher rate. Lee et al. (12) and Yoon et al. (26) demonstrated the effectiveness of using MRI to quantify pancreatic fat and reported a correlation between fatty infiltration of the pancreas and PF occurrence. In this study, we measured mean CTHU and HUHA values to determine whether they were associated with PF occurrence and found that HUHA-A was highly correlated with PF occurrence as in other studies.
Although the assessment of pancreatic softness via manual palpation by a surgeon is subjective, it has been reported to be a useful predictor of PF and, specifically, ISGPF grade C PF (17182728). Similarly, our study found that PF occurred at a significantly higher rate in soft compared to hard pancreatic tissues. Furthermore, higher HUHA-A values were associated with a greater likelihood of pancreatic softness. Therefore, pancreatic softness showed a moderately positive correlation with the HUHA-A value.
Obesity, perirenal fat and pancreatic thickness, and a MPD diameter < 3 mm are predictive factors of PF occurrence (611131718202729). However, in our study, none of these factors were associated with PF occurrence. Several studies have evaluated the association between a small MPD diameter and PF occurrence and had contradictory findings; however, studies enrolling more than 500 subjects found that a small MPD diameter was correlated with PF occurrence (1727). In our study, the MPD diameter was underestimated since there was no difference in the distribution of MPD diameter given the small number of patients enrolled. Pancreatic thickness is an imaging feature associated with PF occurrence. However, in previous studies, the pancreatic thickness cutoff has varied from 12 mm to 17.6 mm (293031). Although pancreatic thickness was greater in the non-PF group in our study, there was no significant difference between the two groups. The reason for this discrepancy is unclear; however, it may have been due to our small sample size, patient body morphology, measurement methods, or observers. In particular, surgical skill or technique may have impacted PF occurrence outcomes; however, this is unlikely since a single surgeon performed all of the assessments in our study. Thus, the relationship between pancreatic thickness and PF occurrence requires further investigation.
HU measurement is significantly affected by intravenous contrast material (32). To avoid contrast material effects, we drew ROIs on pre-contrast CT images. Fat measurement on pre-contrast CT images is less affected by the X-ray tube voltage. Bone and iodine with a high atomic number result in significant differences in mass attenuation coefficient values according to X-ray tube voltages; however, on pre-contrast imaging, there is less difference in tissues, such as fat, muscle, and water. Thus, HU values measured on pre-contrast images may be less affected by 100-kVp or 120-kVp tube voltage (33).
Measuring HUHA values has several advantages. First, it can be measured using CT, which is the most common and basic imaging modality used to evaluate cancer stages, operability, and comorbidities (34). Second, HUHA can be easily performed by drawing an ROI around the pancreatic parenchyma on preoperative CT images. During aging, the pancreas shows non-homogeneous fatty degeneration. To exclude this effect, we performed HUHA by measuring CT attenuation in the axial and corresponding sagittal planes around the pancreaticojejunostomy site with reference to postoperative images. This approach assumes that the 3D distribution of pancreatic fat along the pancreatic resection plane is better reflected by using both axial and sagittal images for measurements. The ROI location used for the HUHA was near the SMV with reference to postoperative images and generally corresponded to the pancreatic resection margin during PD. Third, by simply drawing ROIs on pre-contrast images, the HUHA provides a semi-quantitative measurement of fat content as a percentage value with high inter-observer agreement. We were very careful to exclude peripancreatic retroperitoneal fat tissue from the ROIs, which can affect the results. Furthermore, for convenience, we drew circular ROIs in the pancreatic parenchyma.
Despite the interesting results, this study has certain limitations. First, given the retrospective nature of this study, potential selection bias was inevitable. Second, the degree of fatty infiltration and pancreatic fibrosis was not evaluated histologically. However, several CT studies have demonstrated the effectiveness of fat quantification for determining pathological predictors of PF occurrence. Third, our study population was relatively small and patients had various pathological diagnoses, which could have been a confounding factor. Moreover, the study did not have any cases of ISGPF grade C. Fourth, HUHA values were categorized into 3 groups arbitrarily. Thus, a larger cohort study and external validation are required. Lastly, although CT scanners are regularly calibrated according to the manufacturer's guidelines, attenuation values may differ based on X-ray beam properties. Therefore, the HU value will differ depending on the CT scanners and protocols used.
In conclusion, the HUHA-A values on pre-operative precontrast CT images demonstrate a strong correlation with PF occurrence and is effective in predicting PF occurrence.


 XML Download
XML Download