

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatocellular carcinoma (HCC) is the sixth most common cancer and the second leading cause of cancer-related death worldwide (1). Prior to the application of organized screening and surveillance of high-risk patients for HCC, the mortality attributed to HCC was roughly comparable to its incidence (2). Since the introduction of systematic screening and surveillance for HCC in the mid-1990s, however, 5-year survival has markedly improved (3). Previous studies have since demonstrated that early detection of HCC definitely improved the prognosis of patients with HCC (456) and that screening/surveillance tests utilizing imaging examinations were better than any other screening/surveillance tests, including blood tests, for early diagnosis of HCC (7). Furthermore, the critical role that imaging has played in the screening, surveillance, diagnosis, staging, management, and monitoring of treatment response has further contributed to improvement in HCC mortality (8910). Unlike most other malignancies, HCC can be diagnosed noninvasively, and treatment may be initiated based on imaging alone, without confirmatory biopsy (111213). For this reason, in most current clinical practice guidelines, contrast-enhanced (CE) computed tomography (CT) and magnetic resonance imaging (MRI) have supplanted biopsy as the preferred method of diagnosing HCC with characteristic imaging features (8). This noninvasive diagnosis of HCC based on imaging tests alone is mainly possible due to the following reasons: 1) the pretest probability of HCC has been demonstrated to be sufficiently high in cirrhotic patients, and 2) the high specificity and positive predictive value of HCC imaging criteria in the selected screening cohort (11). The typical imaging hallmark of HCC is a combination of arterial phase hyperenhancement (APHE) and washout on the portal venous and/or delayed phases, which reflects the vascular derangement that occurs during hepatocarcinogenesis (14).
Over the past two decades, many major organizations have proposed HCC imaging systems, including the Association for the Study of Liver Disease (AASLD) (1115), European Association for the Study of the Liver (EASL) (16), Asian-Pacific Association for the Study of the Liver (APASL) (17), Liver Imaging Reporting and Data System (LI-RADS) (1819), the Organ Procurement and Transplantation Network system (20), Japan Society of Hepatology (JSH) (21), and the Korean Liver Cancer Study Group and the National Cancer Center (KLCSG-NCC) (22). The designs of these HCC imaging systems have varied across geographic areas so as to address different target populations, resources, and treatment practices (10). Despite these regional variations, imaging-based HCC guidelines have continued to improve the consistency and standardization of the acquisition, interpretation, and reporting of liver examinations (1023). These guidelines have also been continually updated to reflect the most recent radiological and technological advances, as well as our constantly improving understanding of HCC pathophysiology. In 2018, AASLD (1115) and EASL (16) published updated versions of their guidelines. LI-RADS, which is endorsed by the American College of Radiology (ACR), has been updated 2 years in a row, in 2017 (18) and 2018 (19). The Korean Liver Cancer Association (KLCA)-NCC (previously KLCSG-NCC) has also release new 2018 version of the KLCA-NCC guideline and it is expected to be published soon (in press) (24). The key change this year in both AASLD and EASL guidelines is the addition of hepatobiliary contrast media (HBCM)-enhanced MRI as the first-line diagnostic test to dynamic CT and MRI using extracellular contrast media (ECCM), while the KLCA-NCC and EASL guidelines also include CE ultrasound (CEUS) as the second-line diagnostic test. Therefore, it can be expected that HBCM-enhanced MRI and CEUS will play increasingly important roles in the noninvasive diagnosis of HCC in the years to come.
In this review, we will address the emerging role of HBCM-enhanced MRI and CEUS in the diagnosis of HCC and discuss several unsolved issues when using these two diagnostic tests. In addition, we will briefly review the new HCC diagnostic criteria endorsed by the KLCA-NCC practice guidelines version 2018 and compare them with the other aforementioned guidelines. Finally, we would like to address some remaining issues in the noninvasive diagnosis of HCC.
Role of HBCM
HBCM consists of two gadolinium-based contrast agents (GBCA)-gadoxetate disodium (gadoxetic acid or gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid [Gd-EOB-DTPA]) and gadobenate dimeglumine-that show the dual properties of “conventional” GBCAs and hepatobiliary contrast agents. As these agents show hepatocellular uptake and biliary excretion, they enable the visualization of a key feature of hepatocarcinogenesis in vivo, which is the alteration of transporters on the cellular membranes of hepatocytes (14). Expression of the organic anion transporting polypeptide (OATP) 1B1/3 assessed by HBCM reduces with tumor progression (1425). As a result, a persistent and strong enhancement of the normal background liver via cellular uptake can be observed during the hepatobiliary phase (HBP), whereas premalignant or malignant hepatocellular tumors would have diminished or absent transporter function and therefore show hypoenhancement on the HBP, which appears earlier than the hemodynamic changes in hepatocarcinogenesis (2627). Furthermore, the improved lesion-to-liver contrast during the HBP leads to higher sensitivity for the detection of HCCs than with CT or MRI using ECCM (28). Considering the results of previous studies in which the early detection of HCCs followed by prompt treatment could significantly improve outcome (456), the higher sensitivity of HBCM would have great clinical value, potentially leading to improved survival (29). According to a recent retrospective cohort study, additional evaluation using Gd-EOB-DTPA MRI along with dynamic CT in patients with a single nodular HCC led to the detection of additional HCC nodules in 16.4% of patients, reduced recurrence in 28%, and decreased overall mortality in 35% (29). Therefore, recognizing the benefit of HBCM-enhanced MRI, both APASL v. 2017 and KLCSG-NCC v. 2014 guidelines include HBCM-enhanced MRI as the first-line diagnostic test (1722).
However, controversies remain regarding the ideal timing to determine “washout” on Gd-EOB-DTPA-enhanced MRI. Indeed, extending the phases of washout to the transient phase or including the hypointensity on the HBP in the diagnosis of HCC may increase sensitivity but inevitably lower specificity at the same time (3031). Using the washout in the portal or delayed phase of ECCM on MRI in contemporary guidelines, the overall sensitivity and specificity for noninvasive diagnosis of HCC according to several prospective studies have been reported to be 65–89% and 91–100%, respectively (3233). If Gd-EOB-DTPA MRI is used, the criteria using washout in the portal phase would show very high specificity but have low sensitivity, particularly for nodules < 2 cm in diameter (74.5%) (31). Thus, the criteria to determine “washout” on HBCM-enhanced MRI may depend on the diagnostic aim desired by radiologists and clinicians, whether it is high sensitivity or high specificity (34). In most Western countries, where the prevalence of HCC is not very high, a conservative approach may seem reasonable as over-diagnosis of HCCs may lead to an unnecessary increase in the priority for liver transplantation allocations. On the other hand, in Asian countries where the prevalence of HCC is quite high, diagnostic criteria providing higher sensitivity with reasonably high specificity may be more appropriate because early detection of HCCs may provide a chance for earlier application of potentially curative treatments such as radiofrequency ablation or surgical resection. In addition, as liver transplantations are frequently used as a salvage operation after several attempts, including interventional procedures or surgical resections, in Asian countries, a mild reduction in the specificity for HCC diagnosis may be acceptable if high sensitivity is achievable within certain diagnostic criteria. Considering the widespread use of Gd-EOB-DTPA MRI and clinicians' preference for the early diagnosis and treatment of HCCs in Korea (35), the KLCA-NCC Guidelines version 2018 adopt washout on the portal or transitional phase and hypointensity on HBP. Nevertheless, in order to preserve specificity, the 2018 KLCA-NCC guidelines also apply the exclusion criteria of a targetoid appearance or marked T2 hyperintensity to rule out the most common confounders that show the washout appearance on HBP, i.e., hemangiomas, cholangiocarcinomas (CCs), and combined hepatocellular-CCs (30). Therefore, the revised Korea guidelines can be expected to increase sensitivity while preserving specificity for the diagnosis of HCCs.
Another important merit of HBP is that hypointense nodules on HBP without APHE have a higher risk of progressing to typical hypervascular HCCs than iso- or hyperintense nodules (3637), and thus the signal intensity of HCCs on HBP has been reported to be a prognostic factor (38). Although most HCCs show hypointensity on HBP, the variable hyperintense signal characteristics of some HCCs (−10%) with increased expression rates of OATP transporters in HBP should be considered, especially when they are accompanied by a focal defect within the contrast uptake and a hypointense rim (39).
One major drawback of Gd-EOB-DTPA MRI in comparison with ECCM-enhanced dynamic MRI, however, is the suboptimal or non-diagnostic arterial phase images owing to transient dyspnea or the lower gadolinium concentration of gadoxetic acid compared to other ECCMs (40). Fortunately, however, a previous study has demonstrated that multiple arterial phase imaging with rapid imaging sequences or a modified injection protocol can minimize this problem (41).
Role of CEUS
CEUS is a valuable technique for the characterization of focal liver lesions and is based on the evaluation of hemodynamic alterations (42). The sensitivity for depiction of arterial hypervascularity on CEUS can potentially reduce the number of invasive biopsies otherwise required for such indeterminate nodules in the cirrhotic liver (43). Two major contributing factors of this advantage are the real-time imaging capability of ultrasound and the inherent superior sensitivity of CEUS to microbubbles in comparison with the sensitivity of CT or MRI to iodinated or GBCA (44). Two types of contrast agents are used for CEUS: intravascular contrast agents (also known as pure blood-pool contrast agents) and postvascular phase agents taken up by Kupffer and/or reticuloendothelial cells. Sulfur hexafluoride with a phospholipid shell (SonoVue: Bracco S.p.A., Milan, Italy) and octafluoropropane (perflutren) with a lipid shell (Definity/Luminity: Lantheus Medical, Billerica, MA, USA) are common intravascular agents while Sonazoid (GE Healthcare, Chalfont St. Giles, UK) is a postvascular phase agent. Unlike SonoVue or Definity, Sonazoid provides additional Kupffer phase images (usually 10–60 minutes after its injection) in which typical HCCs show low echogenicity, indicating a lack of contrast uptake due to the absence of Kupffer cells and/or reticuloendothelial cells (45).
There are several distinctive features of CEUS in comparison to CT/MRI that reflect the dissimilarities in their underlying methods of image acquisition and types of contrast agent used. First, CEUS allows real-time evaluation of the enhancement of a nodule, resulting in more sensitive detection of APHE than CT or MRI which may fail to demonstrate transient APHE in the early arterial phase (464748). Therefore, CEUS can be considered to be an alternative imaging option for nodules categorized in CT or MRI as LR-3 or LR-4 due to the absence of APHE, because some of these nodules potentially could be upgraded to LR-5 if APHE is shown on CEUS (44). Second, there are no vascular pseudolesions on CEUS. Arterioportal shunts are the most common vascular pseudolesions in cirrhotic livers on CT and MRI (464950). Although most arterioportal shunts are promptly defined due to their typical wedge shape and location on CT or MRI, some may be mistaken for true lesions and may obscure true HCCs, lowering the sensitivity for HCC detection. On the other hand, since CEUS rarely depicts any arterioportal shunt, APHE on CEUS is highly likely to indicate HCCs in high-risk patients, even in the absence of washout (51).
The usage of CEUS for the diagnosis of HCCs has been variably endorsed by international and national scientific societies (5253). The Japanese, Canadian, Italian, and Asia Pacific hepatology or liver cancer societies were the first to endorse the use of CEUS to establish a diagnosis of HCC, (17215455), most commonly as a second-line technique when CT or MRI proved inconclusive or when they are contraindicated. Recently, the EASL guideline also adopted CEUS with intravascular contrast agents as a secondary diagnostic test (16), whereas the AASLD guideline (15) has not yet accepted CEUS for the diagnosis of HCC. As of now, most guidelines except LI-RADS recommend CEUS as a secondary imaging modality, most likely due to its several potential weaknesses, i.e., the lower detection rate for washout of HCCs than with CT or MRI (515657), limited capability of staging (5156), poor performance in some patients with a poor sonic window or advanced cirrhosis, and lack of availability except in expert centers (15). In addition, most guidelines that have adopted CEUS as a diagnostic tool accept the use of intravascular contrast agents, whereas JSH and APASL guidelines (1721) only accept the use of Sonazoid.
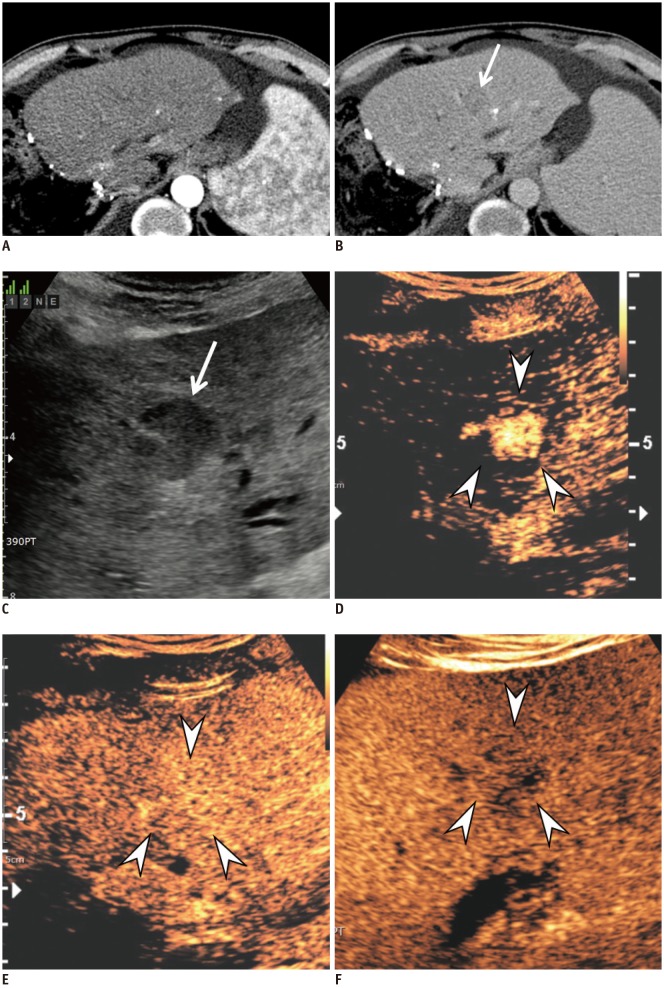
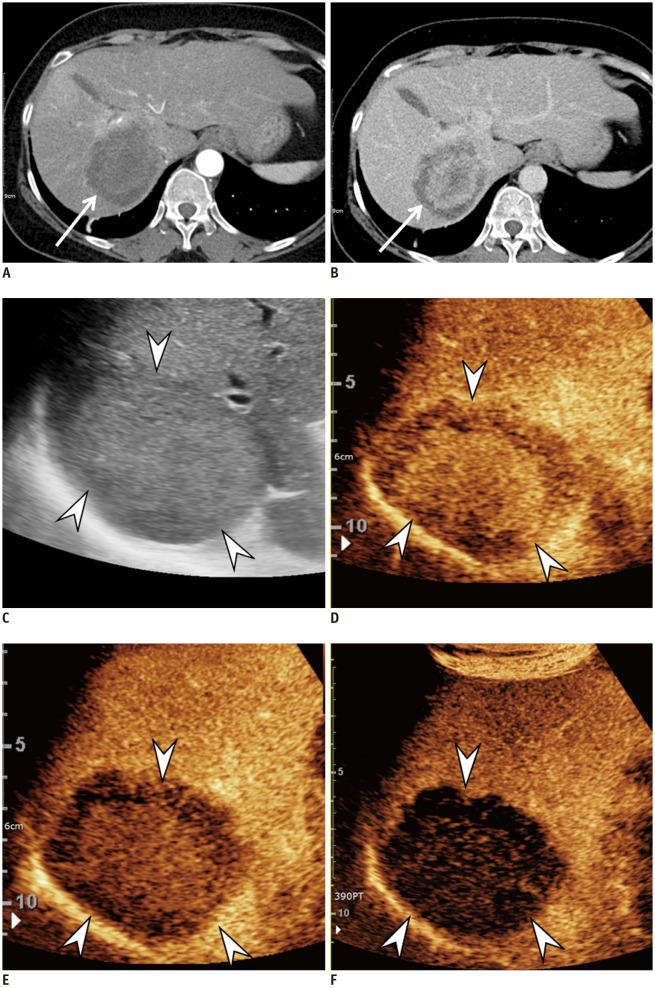
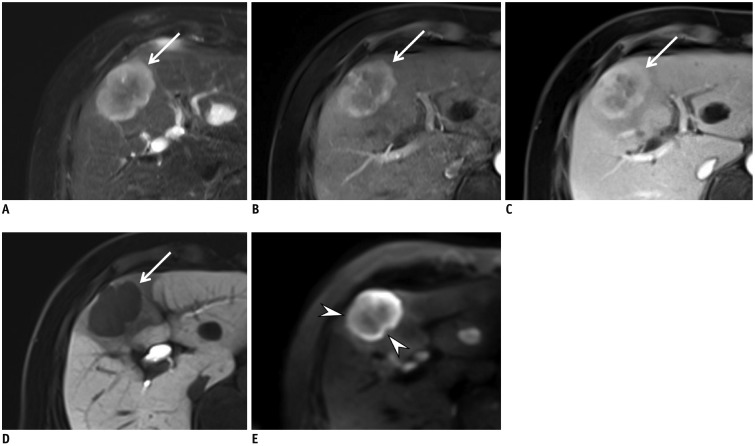
It has previously been questioned whether CEUS can be utilized to derive a specific diagnosis of HCC due to the potential risk of a misdiagnosis in cases of CC, which occurs at a rate of 2–5% among all new nodules in liver cirrhosis (5859). Furthermore, approximately 50% of all mass-forming CCs in cirrhosis show global APHE followed by washout in CEUS, leading to misdiagnosis as HCC (6061). These similarities in the enhancement features of HCC and CC on CEUS, which are different from those on CT or MRI, can be attributed to the different pharmacokinetic features of contrast agents in CEUS from ECCMs used for CT or MRI. Contrast agents for CT or MRI tend to diffuse through the vascular endothelium and accumulate in the interstitial tissue, whereas most contrast agents for CEUS, except Sonazoid, are purely intravascular microbubbles (44). However, subsequent studies (626364) have demonstrated that CEUS can show different APHE characteristics and timing and degree of washout between HCCs and CCs. Specifically, many HCCs showed APHE followed by late (> 60 seconds) and mild washout (6566) (Fig. 1) on CEUS, whereas many CCs showed APHE followed by early (< 60 seconds) and marked washout (6263) (Fig. 2). These refined criteria for HCC on CEUS preserve its extremely high positive predictive value for the diagnosis of HCC while improving its capacity to differentiate other malignant lesions such as CC (58). Indeed, a recent large retrospective study (58) including more than 1000 lesions in cirrhosis proved that these new criteria for HCC on CEUS had a positive predictive value of almost 99% for HCCs and a positive likelihood ratio of 15.5, with no false-positive diagnoses owing to CCs. In another recent prospective multicenter study (67) involving 10–20 mm nodules, CEUS showed a higher specificity of 92.9% compared to CT (76.8%) and MRI (83.2%). Furthermore, after the first inconclusive diagnosis with CT or MRI, CEUS as the second imaging technique showed the highest specificity with only a slight drop in sensitivity for nodules of 10–20 mm and the highest sensitivity and specificity for nodules of 20–30 mm. On the basis of these recent promising results obtained with these refined CEUS criteria for HCC, these criteria have now been adopted in Italy (Italian Association for the Study of the Liver) (54), the ACR in the USA (68), as well as in the updated guidelines in 2018 endorsed by EASL and KLCA-NCC (1624). However, it is critical for clinicians to know that these stringent criteria for HCC on CEUS may provide such high specificity for HCC, unavoidably lowering sensitivity.
The ACR recently updated their CEUS LI-RADS version 2017 similar to LI-RADS for CT and MRI (68). CEUS LI-RADS provides a diagnostic algorithm that categorizes nodules from LR-1 (definitely benign) to LR-5 (definitely HCC), reflecting the readers' certainty in the diagnosis of HCC, according to the lesion size and enhancement patterns. LR-5 nodules can be categorized by the presence of cirrhotic nodules showing APHE followed by late (> 60 seconds) and mild washout, and can be treated as HCCs without biopsy or further imaging. Because LR-5 criteria are very stringent to achieve a high specificity for HCCs, HCCs may occur in other categories, most commonly in categories LR-3 and LR-4 for well-differentiated HCC and in LR-M for poorly differentiated HCC, for which final diagnoses are usually achieved with histology.
New Changes in the KLCA-NCC Practice Guidelines Version 2018
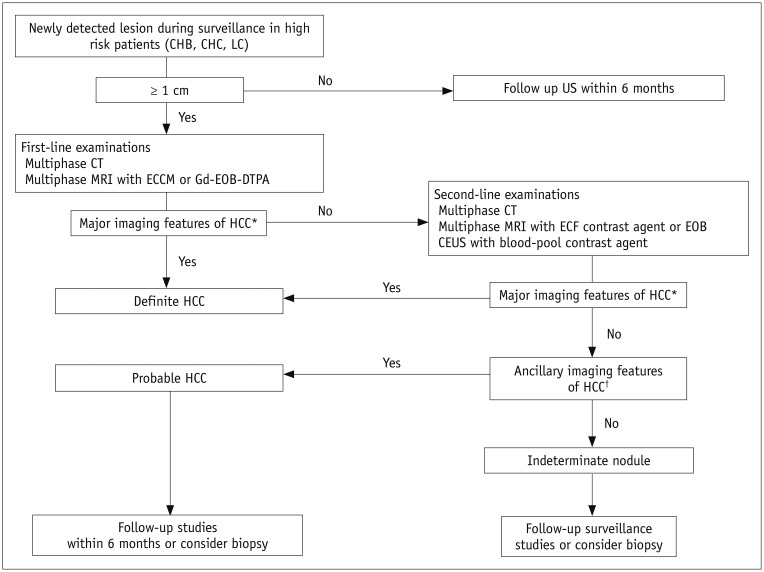
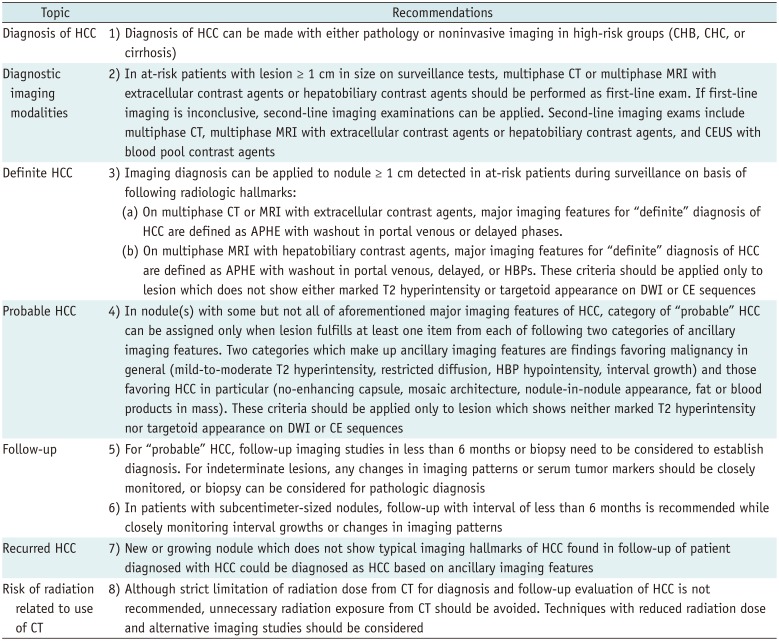
The diagnostic algorithm of the KLCA-NCC practice guidelines is provided in Figure 3. The 2018 KLCA-NCC practice guidelines provide several statements regarding the diagnosis of HCC (Table 1). The major changes in the KLCA-NCC 2018 guidelines compared to the previous version can be summarized as follows:
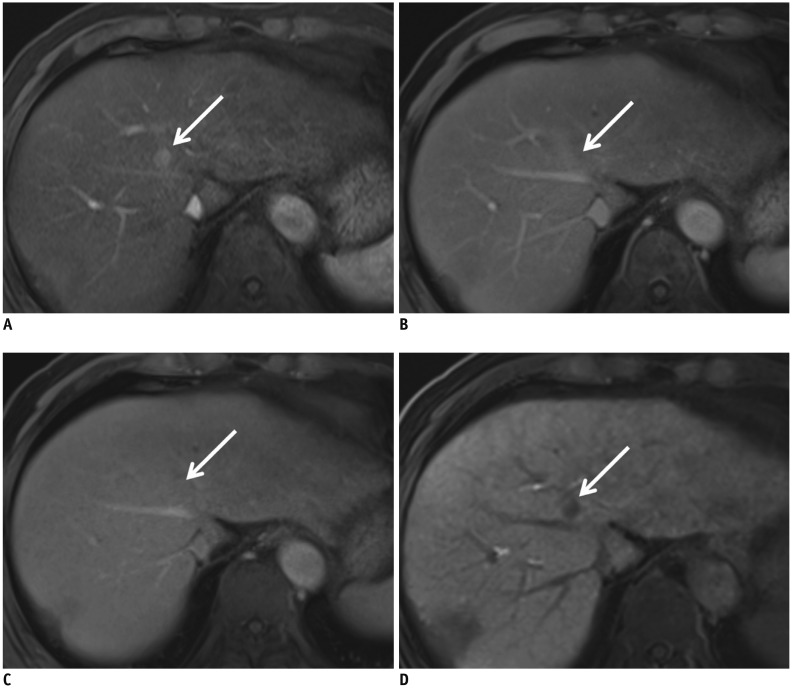
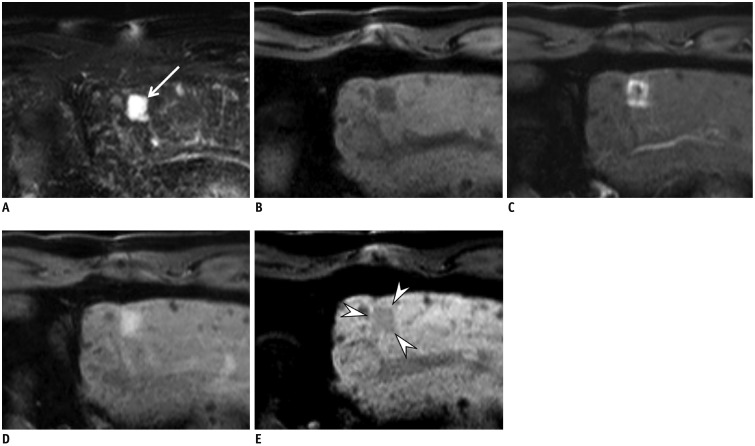
First, the guidelines have adopted new non-binary decisions, e.g., definite, probable, and indeterminate nodules. Second, the guidelines now allow multi-parametric assessment of CT and MRI and therefore, several ancillary features can be used to make a “probable HCC diagnosis.” Third, the guidelines now include “washout” not only in the portal or transitional phase, but also hypointensity on the HBP after applying the exclusion criteria of a targetoid appearance or marked T2 hyperintensity on gadoxetic acid-enhanced MRI. In fact, the additional inclusion of the hypointensity on the HBP when there is no washout on portal venous or transient phase may increase its sensitivity for the diagnosis of HCC (Fig. 4) but at the cost of reduced specificity, mainly due to the pseudo-washout phenomenon (3031). However, since most false-positive diagnoses are caused by hemangiomas, CCs, and combined hepatocellular-CCs from the use of the HBP for determining the washout appearance, applying the exclusion criteria for a targetoid appearance or marked T2 hyperintensity is expected to prevent a significant loss in specificity (30). In keeping with this prediction, Joo et al. (69) recently reported sensitivity of 92.5% and the specificity of 87.4% for the new diagnostic criteria after additionally encompassing hypointensity on HBP as an alternative washout after applying the exclusion criteria. In the study (69), the application of the exclusion criteria significantly improved the specificity (87.4% vs. 48.4%) compared to the criteria without the exclusion criteria. Representative cases are presented in Figures 5 and 6. Furthermore, considering the widespread use of gadoxetic acid-enhanced MRI as well as most clinicians' preference for early diagnosis and treatment for HCCs in Korea, the KLCA-NCC Guidelines version 2018 adopt washout in the portal, transitional, or HBPs after applying these exclusion criteria.
Fourth, CEUS is now adopted as a secondary diagnostic test when a proper diagnosis of HCC is not made by initial diagnostic tests. Lastly, the updeted guidelines suggest separate diagnostic criteria for recurrent HCCs in order to increase sensitivity, considering the higher possibility of HCC development in patients with a history of HCC than those without HCC. For newly developed hepatic nodules or those with an interval size increase during follow-up in patients with a previous history of HCC, HCC can be diagnosed if they show compatible ancillary imaging features, even without typical imaging features.
Comparison between KLCA-NCC Practice Guidelines Version 2018 and Other Guidelines
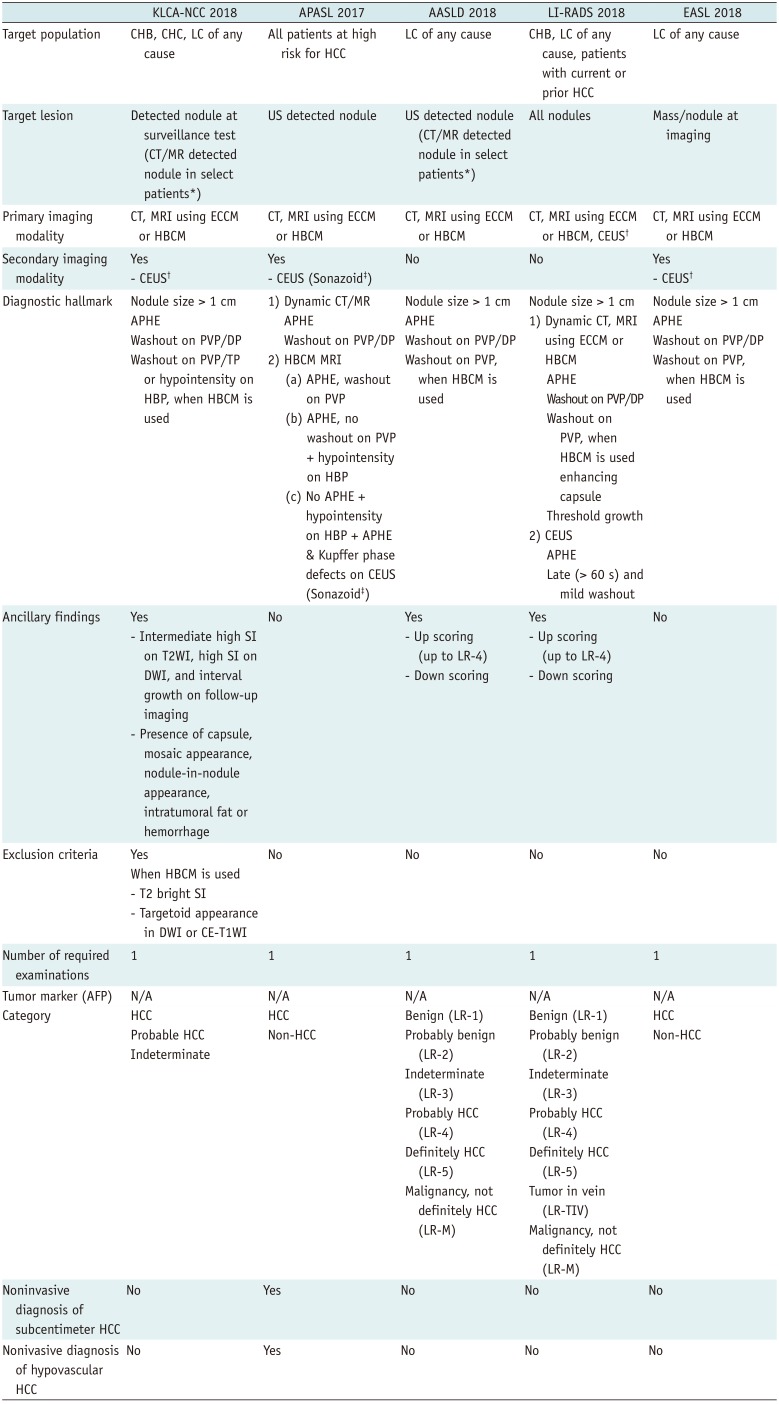
Comparisons of the KLCA-NCC practice guidelines version 2018 with the 2018 AASLD and EASL guidelines, as well as with 2018 LI-RADS and with 2017 APASL, are summarized in Table 2. Compared to the previous guidelines, there have been changes in the diagnostic tests and in the decision algorithm. For example, the 2018 updated guidelines from EASL and AASLD now include gadoxetic acid-enhanced MRI as a diagnostic test, while the new EASL and KLCA guidelines now include CEUS as a second-line diagnostic test.
The KLCA-NCC guidelines share several similarities with other guidelines including AASLD, EASL, LI-RADS, and APASL, i.e., the usage of gadoxetic acid-enhanced MRI as a diagnostic examination with only one diagnostic test required. The KLCA-NCC guidelines also use ancillary findings as exclusion criteria to preserve specificity, similar to AASLD or LI-RADS. As for the target population for surveillance, they are generally similar but they do have a slight difference: the KLCA-NCC guidelines include liver cirrhosis of any cause and chronic hepatitis B or C virus infections whereas AASLD and EASL include only patients with liver cirrhosis and chronic hepatitis B. Furthermore, regarding washout timing, the KLCA-NCC and APASL guidelines include the HBP whereas AASLD, EASL, and LI-RADS use only the portal venous phase. Finally, a definite diagnosis for subcentimeter HCCs or hypovascular HCCs, at present, is only possible with the APASL guideline.
Major discrepancies between the guidelines of Western societies such as AASLD, EASL, LI-RADS and those from Eastern societies such as KLCA-NCC and APASL, are mainly attributed to different priorities in treatment practices between the two geographic areas with different diagnostic scopes (1070). For instance, the new diagnostic criterion for additionally encompassing hypointensity on HBP as an alternative washout after applying the exclusion criteria in KLCA-NCC guidelines version 2018 results in a relatively higher sensitivity of 92.5% but comparable or slightly lower specificity of 87.4% (69), compared to those in previous studies (sensitivity, 60.5–83.5%; specificity, 81.2–100%) (31717273) which evaluated the criterion of APHE plus hypointensity only on the portal venous phase in gadoxetic-acid-enhanced MRI (equivalent to the hypervascular HCC diagnostic criterion used in EASL and LI-RADS). In Europe and USA, the diagnostic criteria are intentionally designed to achieve high specificity rather than high sensitivity for the diagnosis of a definite HCC while diagnostic criteria favor high sensitivity for the detection of early HCCs in Asia. This differences in practice patterns are related to the preference between liver transplantation versus locoregional ablative therapies for the management of patients with early-stage HCCs (1037).
Regardless of the region, another difference among the guidelines could be the preference toward binary versus non-binary decisions with different diagnostic scopes. At present, LI-RADS, AASLD, and KLCA-NCC use a non-binary decision algorithm covering the whole spectrum of observations seen in the liver whereas other systems including EASL and APASL use binary decisions mainly focusing on the distinction between HCCs and non-HCCs. Furthermore, EASL, AASLD, LI-RADS, and KLCA-NCC guidelines allow a definite HCC diagnosis only for HCCs with APHE while the APASL guideline provides criteria for both hypervascular and hypovascular HCCs. Finally, only the APASL guideline allows for a definite HCC diagnosis for subcentimeter nodules based on hallmark imaging features of HCC.
Unsolved Issues or Controversial Issues
There are some unsolved or controversial issues that must be addressed. First, although both EASL and KLCA-NCC practice guidelines start the diagnostic flow with nodules detected at the imaging or surveillance test, the diagnostic flow in AASLD and APASL guidelines mainly depend on US-detected nodules to be initiated (111617). In brief, since US can be regarded as the most appropriate test for surveillance in many regions, the detection sensitivity of US for cirrhotic nodules > 1 cm may significantly affect the sensitivity of the diagnostic algorithm. However, the reported diagnostic accuracy of US when used as a surveillance test ranges between 58% and 89% in sensitivity, although its specificity is greater than 90% (74). One meta-analysis including 19 studies also revealed that US was less effective in detecting early-stage HCCs, with a sensitivity of only 63% (75). Furthermore, the diagnostic performance of US could be limited in patients with truncal obesity or marked parenchymal heterogeneity owing to cirrhosis (75). According to AASLD, EASL, and KLCA-NCC practice guidelines, CT and MRI are not recommended as the primary modalities for the surveillance of HCC in every cirrhotic patient due to the paucity of data on its efficacy and cost-effectiveness. However, in select patients with a high likelihood of having an inadequate US or if ultrasound is attempted but inadequate, CT, MRI, or CEUS may be utilized as an alternative tool to the US examination. Indeed, according to a recent cohort study enrolling 407 cirrhotic patients in which US and HBCM-enhanced MRI were compared for the surveillance of HCC, MRI showed significantly higher sensitivity and a lower false-positive rate compared with US (75). More recently, abbreviated MRI examination protocols showed similar sensitivity to screening US but with a significantly lower false-positive rate (7677). In addition, a previous simulation study by Tanaka et al. (78) demonstrated that CEUS surveillance for HCC could be a cost-effective strategy for cirrhotic patients in the US surveillance group. However, even under these circumstances, the radiation risk due to repeated CT scans, high cost of MR, and the need for contrast injection make their use in long-term surveillance highly debatable. Further studies are warranted to define conditions in which either CT, MRI, or CEUS can be additionally used for the surveillance of HCC.
Second, it is not possible to make a definite diagnosis of HCC for small (< 1 cm) nodules according to most guidelines except APASL due to the low probability of HCC in lesions < 1 cm and the difficulty of making a reliable diagnosis for small nodules on CT or MRI (2870). Currently, only APASL allows a noninvasive diagnosis of HCC for small nodules < 1 cm when they show the hallmark imaging features of HCC on CT or MRI. In addition, according to LI-RADS, for subcentimeter nodules that show arterial hyperenhancement along with one of three major findings such as “washout,” “capsule,” or “threshold growth,” they can be considered to be LR-4 (probably HCC) (19). Furthermore, considering the high progression rate (89.9–100%) of subcentimeter hypervascular nodules showing typical HCC imaging findings on gadoxetic acid-enhanced MRI to typical HCCs in patients with a history of treatment for HCC (3679) and the improved prognosis of very early-stage HCCs compared to early-stage HCCs (7080), the diagnosis of subcentimeter HCCs in patients with a history of treatment for HCC is possible according to the KLCA-NCC version 2018 guidelines. Thus, with diverse opinions on acknowledging the diagnosis of subcentimeter HCCs among guidelines, further studies are warranted to better refine the diagnostic criteria and to better stratify the degree of risk in subcentimeter nodules.
Third, there is no concrete evidence as to which modality would be the most proper secondary imaging modality when imaging findings on the initial modality are inconclusive. Although there has been a trend toward the utilization of CEUS as the secondary modality, as endorsed by EASL, KLCA-NCC, and APASL guidelines, AASLD guidelines still doubt the feasibility of CEUS owing to its operator dependency, lack of generalizability with regional variations in Asian versus Western countries, as well as the absence of a large-scale study. Therefore, further prospective studies involving a larger number of patients are warranted to confirm the role of CEUS as the most effective secondary modality.
Lastly, different contrast agents such as Sonazoid and SonoVue are recommended for CEUS according to the guidelines; Sonazoid is only used in JSH and APASL guidelines. The Kupffer-phase CEUS that can be additionally provided with Sonazoid may provide better sensitivity in the detection of focal hepatic nodules, but may suffer from low specificity for the diagnosis of HCC as other entities such as hemangiomas or CCs also lack Kupffer cells. This limitation of CEUS with Sonazoid is similar to the obstacle faced with HBCM-enhanced MRI. Although defect reperfusion imaging with Sonazoid, which allow reinjection of Sonazoid into areas showing defects in Kupffer phase, may improve the specificity for the diagnosis of HCCs (4581), further studies are warranted to clarify the diagnostic power between the two CEUS agents.
CONCLUSION
In the last 2 years, several major guidelines of HCC have been updated. Key changes in those guidelines are the addition of HBCM-enhanced MRI as the first-line diagnostic test or inclusion of CEUS as the second-line diagnostic test. These changes will have a profound clinical impact on both diagnosis and characterization of hepatic nodules in patients at high risk, and it can also be expected that HBCM-enhanced MRI and CEUS will play an increasing role for the noninvasive diagnosis of HCC in the years to come. Although the noninvasive diagnostic criteria of dynamic CT and MRI with ECCM endorsed by the major guidelines are in good agreement, discrepancies still do exist in the diagnostic criteria of MRI using HBCM. Furthermore, several issues remain to be solved regarding the diagnostic accuracy of US surveillance, diagnosis of subcentimeter HCCs and hypovascular HCCs, the most appropriate secondary imaging modality, and the effect of different CEUS contrast agents (SonoVue and Sonazoid). We hope that these issues can be clearly resolved on the basis of large-scale data-driven evidence, in the near future.
 XML Download
XML Download