

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since 1988, when gadolinium-based contrast agents (GBCAs) were approved by the Food and Drug Administration (FDA), GBCAs have been considered extremely safe (1). Life-threatening adverse reactions, which usually occur immediately or within 24 hours of GBCA administration, occur at a very low rate of 0.001–0.01% (234). Potentially lethal nephrogenic systemic fibrosis (NSF) due to GBCAs was first described in patients with renal failure in 2006 (56). Subsequent research has proved that certain linear GBCAs-gadodiamide (Omniscan; GE Healthcare AS, Oslo, Norway), gadoversetamide (OptiMARK; Guerbet, Raleigh, NC, USA), and gadopentetate dimeglumine (Magnevist; Bayer AG, Berlin, Germany), which have relatively unstable structures and easily release free gadolinium (Gd3+)-are associated with the occurrence of NSF in the presence of renal failure (789). Accordingly, it is recommended to use more stable GBCAs and limit repeated exposure to GBCAs in patients with renal failure, but there are no specific limitations to using GBCAs in subjects with normal kidney functions (10).
Almost 8 years after the first report of NSF, incidental GBCA deposition in the brain was first reported by Kanda et al. in 2014 (11). Subsequent reports have confirmed the association of the repeated administration of GBCAs and high T1 signal intensity in the dentate nucleus and globus pallidus (1112131415161718192021222324252627282930). Despite the increasing evidence of GBCA accumulation in the brain, there is no strong clinical evidence for the harmful effects of GBCAs on the brain. The underlying pathomechanisms of GBCA accumulation in the brain are not clearly known yet. Nevertheless, regulatory actions on GBCAs have been changed recently. The U.S. FDA decided not to restrict the use of any of the GBCAs-including certain GBCAs that are associated with a higher retention of gadolinium in the brain-based on a lack of evidence for the harmful effects of retained gadolinium on the brain (31). However, the European Medicines Agency's the Pharmacovigilance and Risk Assessment Committee has recommended the suspension of marketing authorizations for four linear gadolinium contrast agents-gadobenate dimeglumine (MultiHance; Bracco Imaging S.p.A., Milan, Italy), gadodiamide, gadopentetate dimeglumine, and gadoversetamide-based on the evidence of their accumulation in the brain (3233). The Japanese Pharmaceuticals and Medical Devices Agency has requested specific changes to the labeling regarding precautions about gadolinium retention in the brain in the packages of all GBCAs (34). In line with this, the Ministry of Food and Drug Safety in Korea has requested a mandatory revision of the precaution section in the package insert of GBCAs to state that more gadolinium remains in the brain with the use of linear GBCAs than with the use of macrocyclic GBCAs. Therefore, linear GBCAs should be administered when macrocyclic GBCAs are not appropriate, such as for patients with previous allergic reactions to macrocyclic GBCAs or when other alternatives for liver-specific agents (e.g., gadoxetic acid disodium: Primovist; Bayer AG) are not available (3536).
Despite this series of actions by healthcare policymakers, public concerns continue to increase, and a certain group of researchers has even proposed a new disease category linked to GBCA deposition in the brain (37). Thus, radiologists and clinicians are feeling pressured to understand the significance of GBCA accumulation in the brain as the recent evidence suggests. They also have to educate their potential patients without provoking groundless fears about GBCAs, as well as change their practice according to the evidence and recommendations to avoid certain types of GBCAs. In this review article, we summarize the current knowledge on GBCA deposition in the brain with respect to the types of GBCAs, deposition sites, deposition mechanisms, and clinical implications.
What Exactly are GBCAs? Types and Characteristics
Gadolinium is a rare earth heavy metal in the lanthanide series, with an atomic number of 64. The 7 unpaired electrons in its 4f subshell enable gadolinium to induce a strong paramagnetic effect, which accounts for its use for contrast enhancement in MRI. Free gadolinium, Gd3+, is toxic to humans; therefore, GBCAs are administered to humans in the chelated forms with various ligands to avoid the toxic effects of free gadolinium on the human body (38). The gadolinium in GBCAs must remain in the chelated form until their excretion by the kidneys. However, dechelation of free gadolinium from the GBCA complex appears to occur in vivo and is determined by various factors, such as the chemical stability of the GBCAs, pH, temperature, and competition between GBCAs and ions or ligands (39).
The chemical stability related to the dechelation of free gadolinium from the GBCA complex is determined by both kinetic stability (which is also called kinetic inertness) and thermodynamic stability (40). Kinetic stability refers to how slow the rates of formation and dissociation of the GBCA complex are. The kinetic stability of GBCA is considered much more important than its thermodynamic stability in maintaining the in vivo stability (40). If the kinetic stability is low, free gadolinium is rapidly released from the GBCA complex. The thermodynamic stability determines the concentration of free gadolinium, free chelate, and the GBCA complex at equilibrium. The thermodynamic stability at the physiologic pH of 7.4 is termed conditional stability (39). In addition, the dechelation of free gadolinium from the GBCA complex is also influenced by the potent acceptors of gadolinium, such as inorganic ions (phosphate, carbonate, hydroxide), and the potential alternatives for free gadolinium, such as endogenous metals (Fe3+, Mg2+, Cu2+, Zn2+, and Ca2+) (394142).
Gadolinium-based contrast agents can be classified according to their chemical structures, electrical charges, stability, and biodistribution in the body, which depend on the type of chelating ligands (4043). Based on the structures of the chelating ligands, GBCAs can be divided into two categories: linear and macrocyclic. In macrocyclic molecules, free gadolinium is completely isolated within the preformed cage of the ligands, whereas in linear molecules, free gadolinium is wrapped around with elongated ligands. According to their charges, GBCAs can be subclassified into ionic or non-ionic agents. It is generally accepted that macrocyclic agents are more stable than linear agents due to the former's cage-like structures; furthermore, ionic agents are more stable than non-ionic agents because the electrostatic interactions between the acidic gadolinium and the basic donor groups of the chelates are stronger in ionic agents (4344).
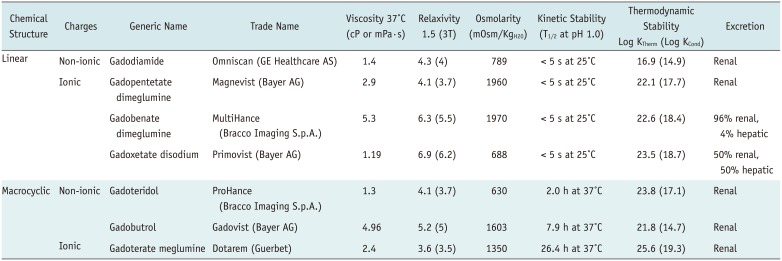
Most GBCAs are nonspecific extracellular contrast agents. When injected via a vein, a GBCA will rapidly disperse into the extracellular space without crossing the intact cell membranes or biological barriers, such as the blood-brain barrier (BBB); finally, the GBCA is excreted through the kidneys. Gadobenate dimeglumine (MultiHance) and gadoxetic acid disodium (Primovist) are well-known combined extracellular-intracellular agents. These agents are in part transported into the hepatocytes by specific mechanisms and excreted into the bile, thus exhibiting dual elimination (bile and urine). Gadoforsteset trisodium (Vasovist; Lantheus Medical Imaging, North Billerica, MA, USA) is an intravascular blood pool agent only. After an intravenous injection, it binds reversibly to serum albumin, making large molecular complexes that restrict passive distribution into the interstitial space. Seven GBCAs are commercially available and widely used in Korea and throughout the world. Their brand names and general chemical characteristics are listed in Table 1.
How did We Realize It? A Short History on Gadolinium Deposition in the Brain
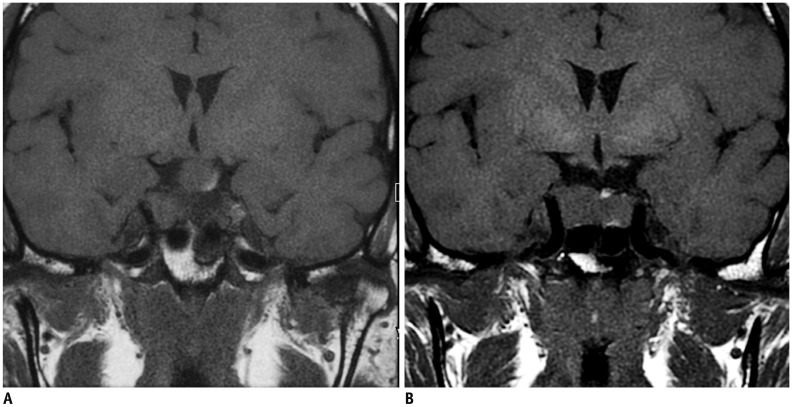
High signal intensities in the globus pallidus and dentate nucleus on non-enhanced T1-weighted images (T1WI) can be observed in many clinical conditions. T1 hyperintensities have been observed in the dentate nucleus in patients with calcification, history of brain irradiation, Langerhans cell histiocytosis, and multiple sclerosis (454647). T1 hyperintensities in the globus pallidus have been associated with hepatic dysfunction, Wilson disease, total parental nutrition, neurofibromatosis type 1, manganese toxicity, Rendu-Osler-Weber disease, hemodialysis, and other medical conditions that can cause calcification in the globus pallidus (484950). In 2014, Kanda et al. (11) reported for the first time T1 hyperintensities in the globus pallidus and dentate nucleus on non-enhanced T1WI in patients with multiple exposures to GBCAs (Fig. 1). Currently, based on numerous published articles (Table 2), gadolinium deposition is one of differential diagnoses of T1 hyperintensities in the globus pallidus and dentate nucleus.
Early reports on gadolinium deposition in the brain mainly focused on signal changes in the dentate nucleus and globus pallidus on MRI (11121314151617181920222324515253). However, the T1 hyperintensities are not limited to these two structures but appear to involve other areas of the brain, including the pulvinar of the thalamus, the precentral and postcentral cortex, the calcarine cortex (54), and the whole cerebral cortex (28). In a study of 13 patients with > 35 administrations of linear GBCAs, T1 hyperintensities were observed not only in the dentate nucleus (100%) and globus pallidus (100%) but also in the substantia nigra (100%), posterior thalamus (92%), red nucleus (77%), colliculi (77%), superior cerebellar peduncle (54%), caudate nucleus (31%), whole thalamus (23%), and putamen (15%) (30).
McDonald et al. (55) confirmed the causal relationship between T1 hyperintensities and gadolinium exposure by demonstrating that T1 hyperintensity is positively correlated with the concentration of gadolinium in the brain tissue, measured by inductively coupled plasma mass spectrometry (ICP-MS) in a cadaveric study. Gadolinium deposition was observed in the pons and thalamus in addition to the observations in the globus pallidus and dentate nucleus (5556). Kanda et al. (57) also found gadolinium deposition in the cerebellar white matter, frontal lobe cortex, and frontal white matter in an autopsy study involving subjects without severe renal dysfunction. These autopsy studies have demonstrated that gadolinium deposition can occur anywhere in the brain tissue, not only in the dentate nucleus and globus pallidus, and that MRI has a limited sensitivity to detect low levels of gadolinium deposition in the brain.
How does GBCA Deposit in the Brain? Histologic Evidence and Suggested Mechanisms
Although imaging evidence of GBCA in the brain is clear, histological and electromicroscopic observations are not straightforward. According to preclinical studies and the few available human autopsy studies, no histological changes have been detected in hematoxylin and eosin-stained sections of the dentate nucleus and globus pallidus from rats and patients administered gadodiamide (linear GBCA) (555859). In a few studies, electromicroscopic examination showed gadolinium deposition in the neuronal tissue, but these studies did not specify the affected cells (5560). A recent electromicroscopic observation of the rodent brain revealed that gadolinium-positive, highly electron-dense structures could be detected only in the endothelial walls of several microvessels in the brain, but not in neurons, neutrophils, or other glial cells (58). Although further studies may be needed to explore the target cells for gadolinium deposition in the brain, these findings raise the possibility that gadolinium itself may not pass through an intact BBB.
The chemical form of deposited gadolinium in brain tissue was discovered in rodent brain studies by Gianolio et al. (61) and Frenzel et al. (62). Gianolio et al. (61) quantified the total amount of gadolinium in the rat brain, as well as the amount of intact GBCA and the insoluble gadolinium-containing form, after repeated injections of macrocyclic and linear GBCAs. The authors found that, three days after the final GBCA administration, macrocyclic GBCA administration resulted in the exclusive presence of intact GBCA in the brain. With regard to linear GBCAs, the retained gadolinium was 10 times higher than macrocyclic GBCAs and was found mostly commonly in the insoluble form, followed by soluble macromolecules and soluble intact linear GBCAs (3.6–18%). In the Frenzel et al.'s study (62), soluble intact GBCAs (either macrocyclic or linear) were slowly excreted between 3 and 24 days. Frenzel et al. (62) suggested that the soluble gadolinium-containing macromolecules (and to some extent, the insoluble fraction that can freely access water) exhibits slow tumbling rates and high relaxivity, which results in T1 hyperintensity on MRI.
Given the findings above, dechelation of free gadolinium from the intact GBCA is considered to be an initial step in the mechanism of gadolinium deposition. In this respect, transmetallation has been suggested to play a major role in gadolinium deposition. Endogenous metals (e.g., Fe3+, Mg2+, Cu2+, Zn2+, and Ca2+) attract ligands to release Gd3+ ions, which in turn are deposited in the tissue as gadolinium phosphate (406364). According to Frenzel et al. (43), the amount of free gadolinium released from linear GBCA (gadodiamide) reached around 25–29% after a 15-day incubation period at 37℃ in human serum. The authors speculated that the presence of other metal ions that compete with gadolinium for chelation could result in the transmetallation (65), which results in the dechelation of gadolinium. Compared with the administration of macrocyclic GBCAs, the administration of linear GBCAs results in a 15-times higher concentration of gadolinium in the brain (5866676869). These results suggest that GBCA with lower thermodynamic stability will facilitate easier transmetallation with endogenous metals, such as iron and zinc (647071). The gadolinium deposition area is intrinsically the iron-rich area and is specifically the area affected by neurodegenerative disorders associated with iron and manganese accumulation in the brain (357071). Gadolinium could target the ferroportin-rich areas that are involved in the active regulation of iron and manganese metabolism, resulting in metal accumulation and toxicity (64).
Another possible mechanism for gadolinium accumulation is a metal-transporter-mediated accumulation of GBCA. A high concentration of gadolinium has been reported in the dentate nucleus, globus pallidus interna, and pulvinar of the thalamus (6572), with iron or calcium also showing relatively higher concentrations in these regions (73). These findings suggest that gadolinium is not transported passively but rather by some biological mechanisms, such as metal transporters (6574). Specific metal transporters mediate the transport and the intracellular distribution of metals. Less is known about the exact mechanism. Many types of metal transporters are present at different concentrations, and each mediates and maintains the concentration gradient of the metal. Transporters are not always specific for a single metal, and they can transport chemically similar metals, such as lead and cadmium (6574).
Finally, the cerebrospinal fluid (CSF) pathway has been suggested to have a role in the mechanism of brain accumulation of gadolinium. A possible route of brain exposure to all GBCAs via the CSF has been observed in rats (75) and some humans (76), thereby bypassing the BBB.
Recent preclinical studies have also reported that the gadolinium concentration was highest in the olfactory bulb after both the linear and macrocyclic agent exposures (5868). Interestingly, the gadolinium concentration was decreased in the posterior direction in animals that were administered gadopentetate dimeglumine, whereas the gadolinium concentrations were similar in all 7 investigated regions of animals that were administered gadodiamide (58). These findings suggest that an ongoing drainage of CSF occurs from the subarachnoid space through the olfactory nerves into the nasal lymphatic system (58). Iliff et al. (77) revealed that GBCAs distribute along the glymphatic system (a so-called waste clearance system) after intracisternal injection, from the basal artery to the olfactory artery (paravascular pathway), suggesting that GBCAs enter the brain through the exchange between CSF and interstitial fluid (58). A recent study involving patients administered GBCA in the subarachnoid space showed increased signal intensity of the cortex and white matter 4 hours after GBCA administration (78). Naganawa et al. (79) demonstrated signal enhancement in the subarachnoid space and perivascular space on enhanced fluid-attenuated inversion recovery (FLAIR) 4 hours after GBCA administration. This result suggests that even in normal renal function, intravenous GBCA can be transported through the glymphatic system and reach the brain (65).
What Type of Contrast Agent Is Responsible for Gadolinium Deposition in the Brain?
Many studies have investigated the association between T1 hyperintensities in the globus pallidus and dentate nucleus and multiple administrations of linear GBCAs (1112131415161718192021222324252627282930). In retrospective human studies that included patients with multiple linear GBCAs, T1 signal changes in the dentate nucleus and/or globus pallidus were consistently associated with multiple administrations of nonspecific extracellular linear GBCAs, such as gadodiamide (11121722) and gadopentetate (1113192326). On the other hand, some studies focusing on the signal changes in patients who were repeatedly administered macrocyclic GBCAs (gadobutrol [Gadovist; Bayer AG], gadoterate meglumine [Dotarem; Guerbet, Rovi, France], and gadoteridol [ProHance; Bracco Imaging S.p.A.]), which are more stable, have found that macrocyclic GBCAs were not associated with significant signal intensity changes in the globus pallidus and dentate nucleus in the brain (5280818283). Studies comparing linear (gadopentetate) and macrocyclic (gadoteridol or gadoterate meglumine) agents have reconfirmed that the signal intensity change is significantly and exclusively related to the use of linear agents (141516208485).
All of the above-mentioned studies were retrospective human studies using MRI; therefore, the study results cannot be compared. The patient populations, the number and frequency of GBCA administrations, the cumulative amounts of GBCAs, and the methods for measuring signal changes on MRI could not be completely controlled and standardized; therefore, the results contradict other studies using gadobenate (171822), gadoxetic acid (278687), gadobutrol (5388), and gadoterate meglumine (89). Moreover, several autopsy studies measuring the deposited concentrations in brain tissue using ICP-MS revealed that gadolinium could be detected regardless of the GBCA class (5556576090).
Prospective animal studies with standardized protocols were developed to overcome the potential pitfalls of retrospective human studies. These animal studies have also demonstrated an association between exposure to linear GBCAs and gadolinium accumulation in the brain (586266676975919293). According to Robert et al. (66), all linear GBCAs (gadodiamide, gadopentetate, and gadobenate) resulted in T1 hyperintensities in the deep cerebellar nuclei of rats, whereas macrocyclic GBCAs (gadoterate meglumine) did not. Several studies using MRI demonstrated signal intensity changes in the deep cerebellar nuclei of rats that were associated with the administration of linear GBCAs (gadodiamide, gadopentetate, and gadobenate) but not macrocyclic GBCAs (gadoterate meglumine) (66677591). The animal studies using ICP-MS demonstrated that gadolinium concentrations in brain tissue were significantly higher in animals exposed to linear GBCAs (gadodiamide, gadopentetate) than in those exposed to macrocyclic GBCAs (gadobutrol, gadoteridol) (589193). However, more recent studies reported that gadolinium was detected in rats repeatedly injected with macrocyclic agents, albeit at very low levels (9194).
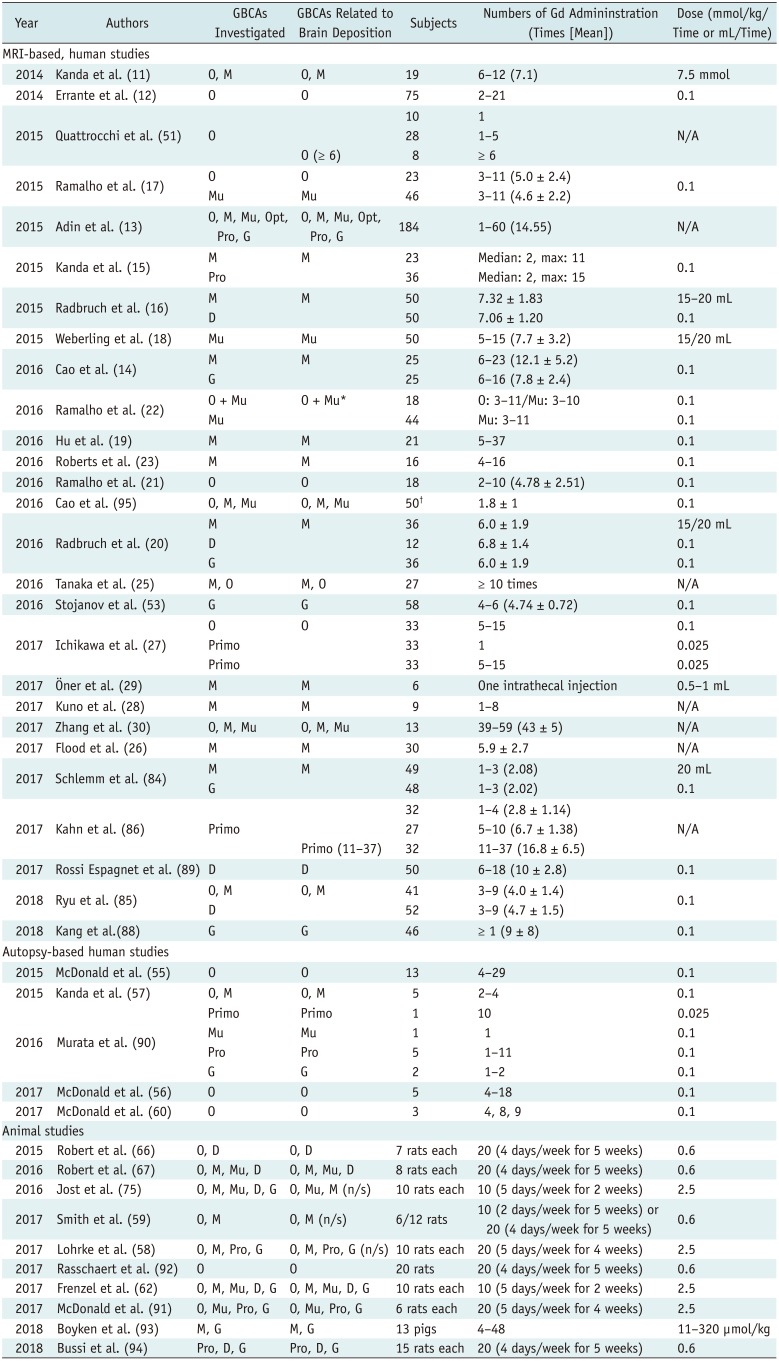
Table 2 summarizes the studies that demonstrate a relationship between GBCAs and signal intensity changes in the dentate nucleus and globus pallidus in human and animals.
Who Is Susceptible to Gadolinium Deposition in the Brain?
Current evidence suggests that a certain threshold needs to be reached in order to change the magnetic resonance (MR) signal after repeated injections of linear GBCAs. In a study with gadodiamide, at least 6 enhanced MRI scans were required to reveal the T1 hyperintensity in the dentate nucleus (51). Studies by Weberling et al. (18) and Adin et al. (13) have also supported the findings that at least 4–6 injections of linear GBCAs are required to cause a visually detectable T1 signal change in the dentate nucleus. Two autopsy studies on subjects exposed to gadodiamide have confirmed that gadolinium deposition in the brain showed a dose-dependent relationship with the injection doses of the GBCAs (5556).
Because most of GBCAs used for the diagnosis of brain diseases are exclusively excreted by the kidneys, longer retention times of the GBCAs in the body can be expected in patients with impaired renal function. A longer retention time in the body is associated with a higher chance of dechelation of the free Gd3+ from GBCAs, according to their stability and patients' conditions. Patients undergoing hemodialysis who have repeated injections of linear GBCAs have a greater T1 signal increase in the dentate nucleus compared to patients with near-normal renal function (95), which was corroborated by an animal study (92). All this evidence suggests that renal function affects the rate of gadolinium accumulation in the brain after linear GBCA injection.
The pediatric population has also shown similar findings in terms of gadolinium deposition in the brain. In studies by Hu et al. (19) and Roberts et al. (23), administration of at least 5 doses of gadopentetate was linked to an increased signal intensity of the dentate nucleus and/or globus pallidus. The dentate nucleus signal intensity was significantly correlated with the cumulative dose of GBCAs (26). However, macrocyclic GBCAs were not associated with T1 signal change of the dentate nucleus and globus pallidus in a pediatric population (96). In a study involving both linear GBCA-exposure and macrocyclic GBCA-exposure groups in a pediatric population, only linear GBCAs were found to be responsible for significant signal intensity increase in the dentate nucleus and globus pallidus between the first and last examination (85). Only one pediatric study of a macrocyclic GBCA (gadoterate meglumine) reported no visible T1 hyperintensities but an increase in the dentate nucleus-to-pons ratio and globus pallidus-to-thalamus ratio in subjects with multiple GBCA exposures (89). There is no clear evidence that pediatric subjects are more susceptible to gadolinium accumulation in the brain. Compared with adults, pediatric patients are more likely to be injected with GBCAs repeatedly throughout their lifetimes; furthermore, pediatric patients may have longer retention times after gadolinium deposition for the rest of their lives. Hence, because the developing brains of infants and children are more vulnerable to certain toxic agents, it is wise to consider pediatric patients as a high-risk group for gadolinium deposition in the brain.
How Can GBCA Deposition Be Visualized Using MRI?
In most of the human reports (Table 2), the T1 hyperintensity due to gadolinium deposition was observed using the spin-echo (SE) or turbo SE techniques (11121415171922232527282953858689). However, T1-weighted gradient-echo sequences, such as the fast low angle shot and magnetization-prepared rapid gradient echo (MPRAGE), can also be used to visualize the T1 hyperintensity due to GBCAs (131416182021263084). T1 FLAIR also depicts the T1 hyperintensity due to GBCAs (13).
Ramalho et al. (21) investigated the feasibility of T1 sequences for the visualization of gadolinium deposition. The authors found that the signal intensity ratio difference before and after GBCA exposures was significantly observed on both SE and MPRAGE sequences (21).
Kuno et al. (28) used T1 and T2 relaxation maps produced using the mixed fast spin echo pulse sequence to assess the effect of gadolinium accumulation in the global and regional brains of patients with prior exposure to linear GBCAs. In this study, the T1 values in the gray matter were significantly shorter in patients with prior GBCA exposure than in those without the prior exposure (p = 0.022). In addition, the authors also found the T1 value of the whole brain, globus pallidus, dentate nucleus, and thalamus and the T2 value of the whole brain, dentate nucleus, and thalamus to correlate significantly with the cumulative doses of GBCAs.
In another studies using T1 and T2* relaxometry, the T1 relaxation time in the dentate was significantly correlated with the number of GBCA administrations (8897). In contrast, the T2* signal intensity was age-dependent and independent of previous GBCA administrations (97).
Recently, it has been suggested that quantitative susceptibility mapping (QSM) enables us to calculate the susceptibility value change induced by GBCA accurately. Hinoda et al. (98) reported increased susceptibility of the brain areas in the multiple GBCA-exposure group as compared with the normal control group.
These quantitative study results using either T1/T2 mapping or QSM are completely in line with reports of T1 hyperintensities in the brains of patients with multiple exposures to GBCAs.
What Is the Clinical Significance of GBCA Deposition in the Brain?
Despite accumulating evidence of gadolinium deposition in the brain, little is known about the clinical importance of gadolinium accumulation in the brain. Considering the location of gadolinium deposition in the globus pallidus, one can infer that the gadolinium deposition might be associated with extrapyramidal system dysfunction and might be related to parkinsonism in later life.
In a population-based study (n = 246557) of two groups that underwent initial MR imaging between 2003 and 2013 (one group with exposure to at least one dose of GBCA and the other without the exposure), the authors found no significant difference in the presence of incidental parkinsonism between the two groups (99). The authors concluded that their results contradicted the hypothesis that gadolinium deposits in the globus pallidus lead to neuronal damage that manifests as parkinsonism. However, a weakness of this study was the lack of details on MR.
Bauer et al. (100) evaluated 376 patients who underwent both contrast-enhanced MR and PET/CT imaging between 2004 and 2015. They found that the median SUVmax of the dentate nucleus and globus pallidus was significantly lower in the group with exposure to gadolinium than in the control group; the differences were 16% and 27%, respectively. Accordingly, the authors speculated that gadolinium deposition led to decreased FDG uptake due to decreased metabolism in the corresponding area. However, they did not correlate these findings to clinical findings.
Semelka et al. (101) proposed a new disease category-gadolinium deposition disease-based on the observational study of 42 patients who underwent gadolinium-enhanced MRI previously. In the acute stage of gadolinium exposure, patients complained of central and peripheral pain, headache, bone pain, and skin thickening. In the chronic stage, 29 of 42 patients had persistent clouded mentation and headache.
At the time of introduction of GBCA, dose-dependent neurotoxicity was reported in a preclinical study using dogs (102). According to Roman-Goldstein et al. (103), gadopentetate dimeglumine administration after osmotic BBB disruption increased the frequency of delayed seizures in a dose-dependent fashion. Although human studies have not proven these findings of central nervous system toxicity, it is reasonable to suspect there is still a possibility of neurotoxicity due to gadolinium deposition in the brain when GBCA is given repetitively to subjects. Thus, further evidence is needed to explore the clinical impact of gadolinium deposition in the brain.
Are There Alternatives?
As discussed above, the exact nature and clinical implication of GBCA accumulation in the brain are still unknown. Despite the convincing evidence of a link between exposure to linear GBCA and gadolinium accumulation in the brain, we cannot currently conclude that macrocyclic GBCAs do not accumulate in the brain. At present, it is advisable to minimize the number of repeated doses of GBCA as much as possible. There are several ways to reduce the number of repeated doses of GBCA. A recent study has suggested a possibility that a deep learning method can be used to enhance the image quality of low-dose post-contrast enhanced images up to a level comparable to full-dose post-contrast enhanced images (104). Some other possibilities have been suggested, such as iron-contrast agents that can be used for contrast-enhanced MRI (105). Several interesting ideas have been tried to enhance the image quality of MRI, such as the use of natural D-glucose as an infusible biodegradable MRI agent (106). Other approaches include the use of endogenous contrasts, such as arterial spin labeling (107).
However, given the lack of evidence of clinical harm due to GBCA deposition in the brain, we also have to be careful about the potential harm from overprotective measures against GBCA use in clinical practice. In addition, we have to be careful to weigh the potential harm of GBCA-enhanced MRI without radiation exposure and that of iodine contrast-enhanced CT imaging with radiation exposure. Given the rarity of GBCA-related toxicity and brain deposition, for which the exact clinical implications are unknown, the risk of GBCA use should not be judged on the basis of perception rather than facts.
CONCLUSION
In summary, linear GBCAs were found to be almost exclusively responsible for the brain accumulation of gadolinium after repeated injections, as evidenced by T1 hyperintensity. Furthermore, the most recent animal studies have also documented the brain accumulation of gadolinium from macrocyclic agents, albeit at very low levels. The dechelation of free gadolinium from unstable GBCAs, transmetallation, active metal transporters in cell membranes, and the glymphatic system as an alternative access route to the brain may have roles in the underlying mechanisms of gadolinium accumulation. Linear GBCAs are considered to be less stable than macrocyclic GBCAs; therefore, they have a greater chance of brain deposition. Despite a lack of clinical evidence on the neurologic effects of gadolinium deposition, a careful approach to the use of GBCAs in clinical practice is advisable until further evidence is discovered.
 XML Download
XML Download