

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Drug-eluting microspheres (DEMs), also called drug-eluting beads (DEBs), are a type of drug delivery system that was introduced in 2006 for the treatment of hepatocellular carcinoma (HCC) (1). Although conventional transcatheter arterial chemoembolization (c-TACE) is considered the first-line palliative treatment for patients with unresectable HCC (2), it has important technical and scheduling drawbacks that have not yet been standardized. Moreover, lipiodol oil used in c-TACE may cause severe pain in some patients. DEM-transcatheter arterial chemoembolization (DEM-TACE) was produced to overcome these drawbacks and ensure sustained and tumor-selective drug delivery while delivering permanent embolization (1). The microspheres can load a variety of drugs through mechanisms such as ion exchange or absorption (134), and when infused directly into target tumors through catheters or microcatheters, can release chemotherapeutic agents in a sustained manner over a prolonged period (13).
Chemotherapeutic agents delivered through this approach are not only cytotoxic to tumor cells but also cause ischemia and tumor necrosis. Moreover, DEM-TACE results in high concentrations of chemotherapeutic agents being delivered to tumors without elevating systemic concentrations. Therefore, the typical adverse effects associated with c-TACE may be reduced by using DEM-TACE. In this review, recent advances in the use of DEM-TACE for the treatment of HCC are summarized.
Types of Microspheres, Chemotherapeutic Drugs, and Pharmacokinetics
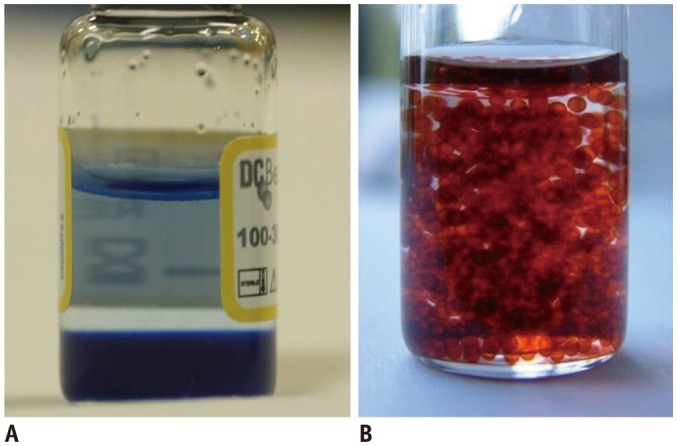
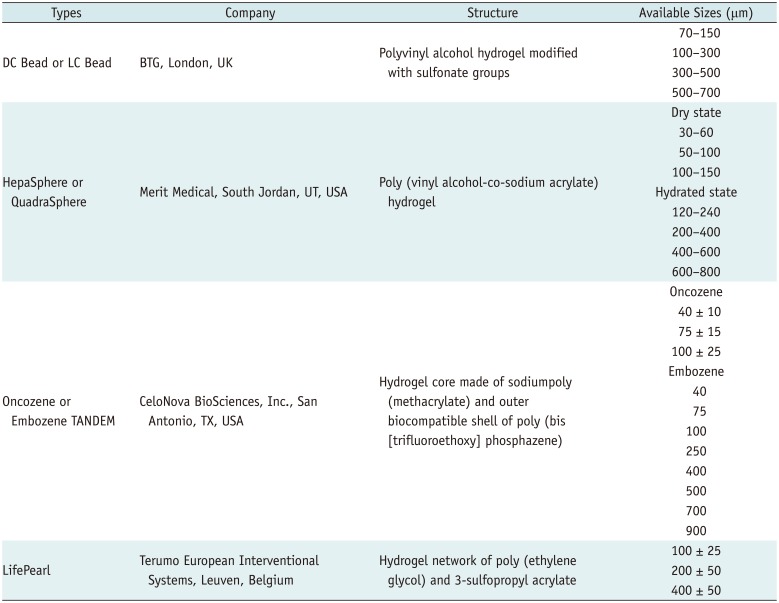
Many types of microspheres are commercially available (Table 1) (56). The microspheres most commonly used in clinical practice are DC Bead® (BTG, London, UK) and HepaSphere™ (Merit Medical, South Jordan, UT, USA). Other microspheres include Oncozene™ TANDEM® (CeloNova BioSciences, Inc., San Antonio, TX, USA) and LifePearl® (Terumo European Interventional Systems, Leuven, Belgium). All are negatively charged and allow the uploading of different types of chemotherapeutic agents. Doxorubicin is most frequently used in DEM-TACE, and in vitro, more than 99% of a solution can be loaded into any of the previous four microspheretypes within 1 hour (5). However, other microsphere characteristics differ by product, and some can efficiently load doxorubicin concentrations as high as 45 mg/mL, regardless of the bead size (7) (Fig. 1).
Many preclinical in vivo studies have shown the sustained release of pharmacologically active concentrations of doxorubicin into target cancerous tissues over several weeks, with drug diffusion of over 600 µm from the circumference of the beads (89). The local delivery of doxorubicin in HCC explants was compared among patients embolized receiving DEBs with histological modifications. The results revealed that the distribution of the beads in the cancerous and surrounding tissue vasculature could be controlled. Indeed, drug release started within the first few hours of bead infusion and was maintained for at least 1 month, with effective necrosis of the target tissue (10).
It has also been reported that peak serum doxorubicin concentrations are significantly lower after DEB-TACE than after c-TACE (111213). This suggests that the interaction time between the chemotherapeutic agent and tumor cells is increased, while the plasma concentration of the agent is decreased, resulting in more effective treatment and fewer systemic complications (14).
Drug-eluting microspheres are available in different sizes (Table 1). Although large-caliber microspheres (>300 µm) can cause ischemia, they may be associated with premature embolization of the feeding artery before the chemotherapeutic agent can be completely effective (15). Premature arterial embolization may damage the blood vessel, prevent subsequent tumor-directed treatment (16), and cause hypoxia-induced neoangiogenesis (1718). Infusion of 100–300-µm microspheres in an animal model of liver cancer resulted in the delivery of these microspheres intothe tumor or near its margins, justifying their use for precise drug delivery or embolization (19). Although many institutions in Korea suggest using 100–300-µm microspheres in the procedure (20), the choice of microsphere size depends on many factors, including tumor size, feeding artery diameter, personal preference and experience, and the presence or absence of an arteriovenous shunt that increases the risk of pulmonary complications (21).
Indications and Contraindications
In general, the indications and contraindications for DEM-TACE are similar to those for c-TACE (Tables 2, 3). Its use depends on the size and vascularity of the tumor, the number of tumors, whether the lesion is infiltrative, and whether the lesion extends to surrounding vessels. Other factors associated with the use of DEM-TACE are the results of liver function tests and possibility of cure. The guidelines of the European Association for the Study of the Liver-European Organisation for Research and Treatment of Cancer recommend TACE as a first-line treatment for asymptomatic patients with preserved liver function who have multinodular lesions but show no evidence of vascular invasion or extrahepatic spread (intermediate stage, or stage B in the Barcelona Clinic Liver Cancer [BCLC] staging system) (222324). TACE is also an appropriate palliative treatment for patients who require curative treatment but are not suitable for surgery or percutaneous ablation (25). Moreover, DEM-TACE is considered a better option than c-TACE for patients with more advanced disease or cardiac failure, and for those expected to have severe post-embolic toxicity (26).
Although liver transplantation is a curative treatment for appropriately selected patients with HCC, a donor liver may not be immediately available, requiring the candidate to wait. By inducing ischemic tumor necrosis and inhibiting tumor progression, both c-TACE and DEM-TACE can extend the period, during which the patient meets the morphologic criteria for liver transplantation, as well as increasing the potential for curative treatment (2728). The reduction of active tumor tissue in such a setting would suggest that patients initially not fulfilling the morphologic criteria may ultimately be shown to benefit from liver transplantation (29).
Drug-eluting microsphere transcatheter arterial chemoembolization is contraindicated inpatients with decompensated baseline liver function, massive arteriovenous shunts, or infiltrative HCC (213031). While portal vein thrombosis was previously considered a contraindication for transarterial therapy (32), it has not been shown to affect survival after DEM-TACE or c-TACE adversely (333435). Other contraindications are related to the chemotherapeutic drugs and angiographic procedures, such as hypersensitivity to contrast media, renal insufficiency, uncorrectable coagulopathy, and peripheral vascular disease preventing arterial access.
Technique
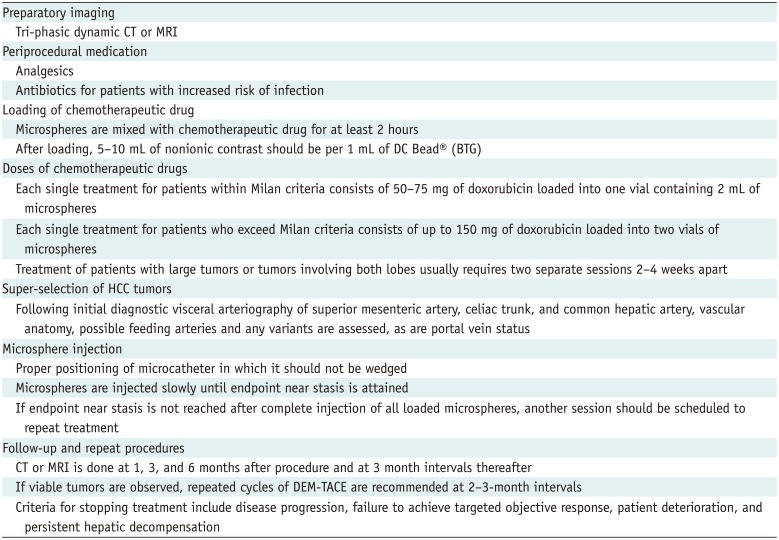
The principle of DEM-TACE is to standardize targeted chemotherapeutic agent delivery to ensure a good ischemic effect on tumors and to overcome the drawbacks associated with c-TACE. Although, Lencioni et al. (36) previously described a technique that they proposed as a general guideline for DEM-TACE use (Table 4), there are some approaches that consider each patient and tumor characteristic. DEM agents can be applied to the extrahepatic arteries supplying the tumors (20); however, to the best of our knowledge, no studies have focused on the safety and efficacy of DEM-TACE in this context.
Imaging
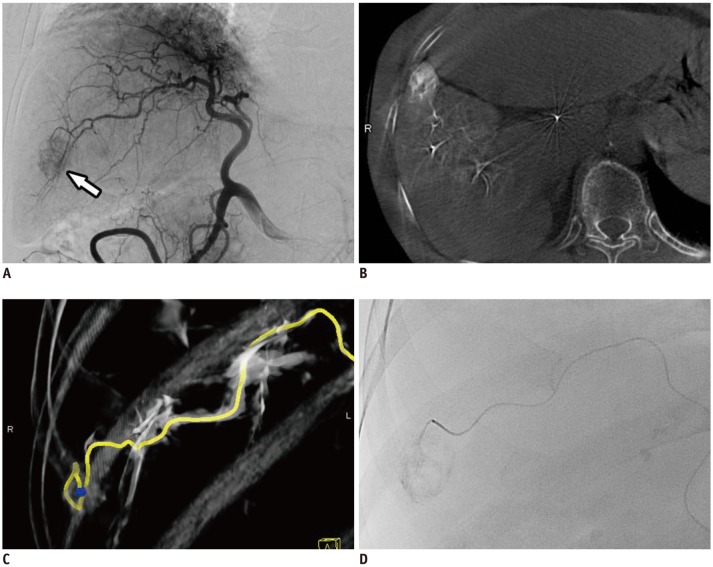
An appropriate planning of DEM-TACE requires hepatic tri-phasic dynamic computed tomography (CT) or magnetic resonance imaging to optimize a microsphere delivery of a chemotherapeutic drug to a lesion. Cone-beam CT is considered a useful imaging tool for determining vascular anatomy and anatomical variants, facilitating better tumor targeting and the avoidance of non-target embolization, as well as predicting the efficacy of DEM-TACE (Fig. 2) (3738). Recent literature has indicated that it should be considered a standard technique, particularly in cases of difficult lesion access, such as when lesions are present in the caudate lobe or when they have extrahepatic collateral arteries (39).
Periprocedural Antibiotics
Although a meta-analysis has shown that routine antibiotics may be unnecessary, the judicious use of antibiotics is appropriate for patients at an increased risk of infection (40). Risk factors include old age, larger nodules, bilioenteric anastomosis, biliary stent implantation, compromised hepatic function, hypoalbuminemia, portal vein cancer embolus, and diabetes mellitus (4142). The antibiotics used should cover gram-positive and gramnegative aerobic and anaerobic organisms, according to previous reports (40).
Super-Selection of HCCs
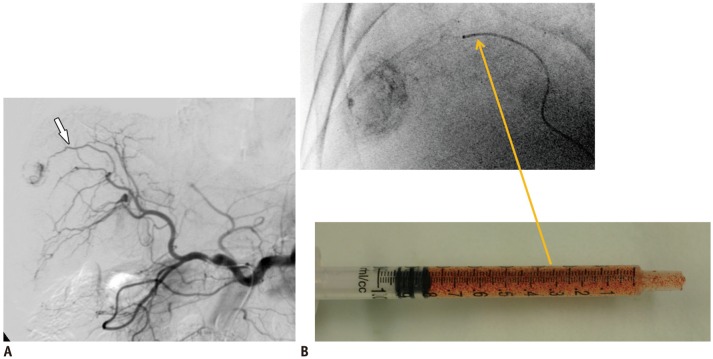
Arterial super-selection at the segmental, subsegmental, and tumor-feeding artery levels was previously considered a favorable prognostic factor for disease-free survival among patients with HCC undergoing c-TACE (43). This was supported by animal studies showing the retention and sustained release of doxorubicin after DC Bead® embolization for up to 90 days after liver embolization (44). Hence, the ischemic effect due to DC Bead® reflux may continue for more than 3 months and be more severe than that produced by c-TACE (44). Recently, a case of multi-organ ischemia was described as a consequence of DC Bead® reflux into the gastroduodenal, right gastric, right gastroepiploic, left gastric, and splenic arteries (45). Therefore, it is preferable for all tumor-feeding arteries to be super-selected to prevent non-target embolization (Fig. 3).
Tumor Response to DEM-TACE
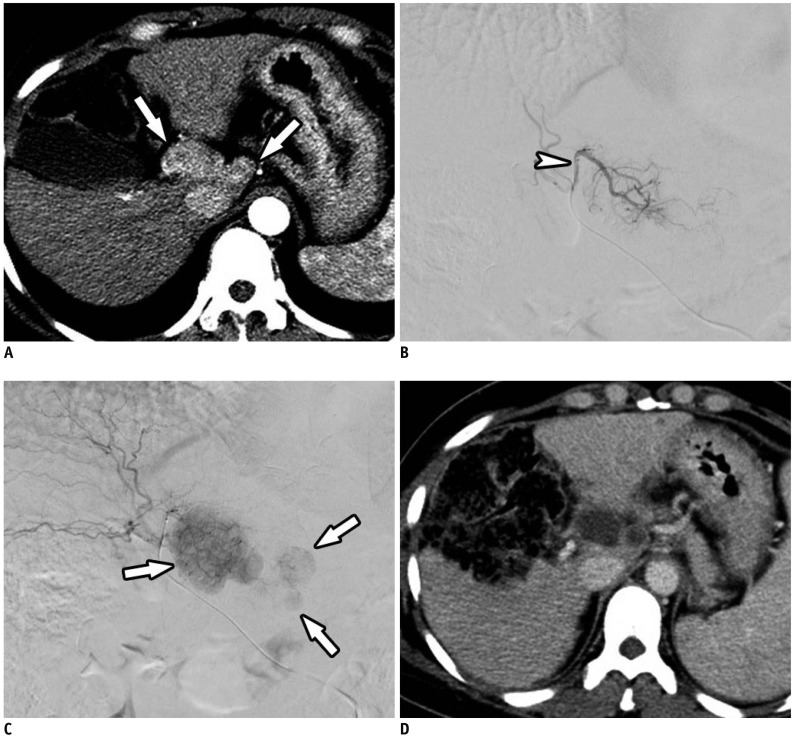
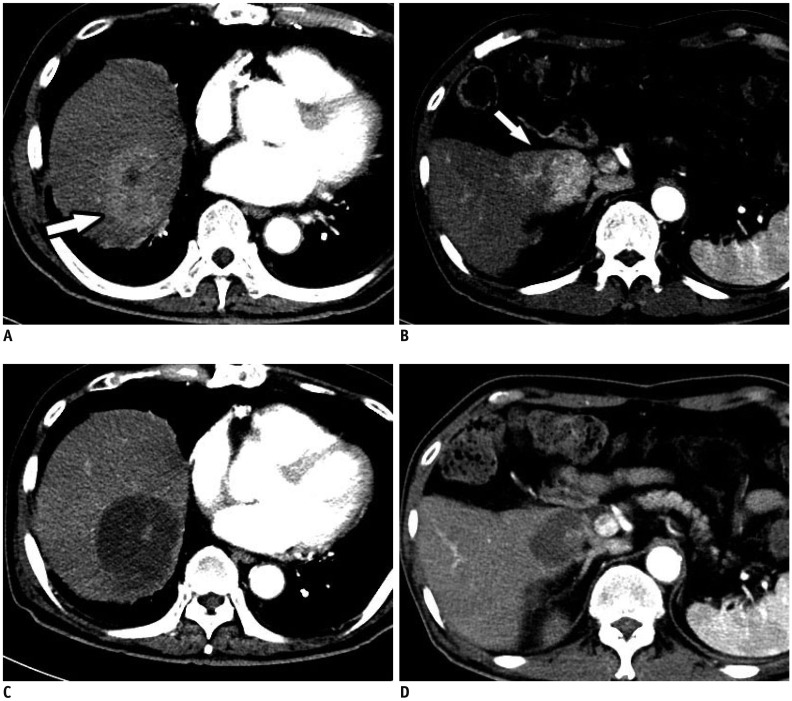
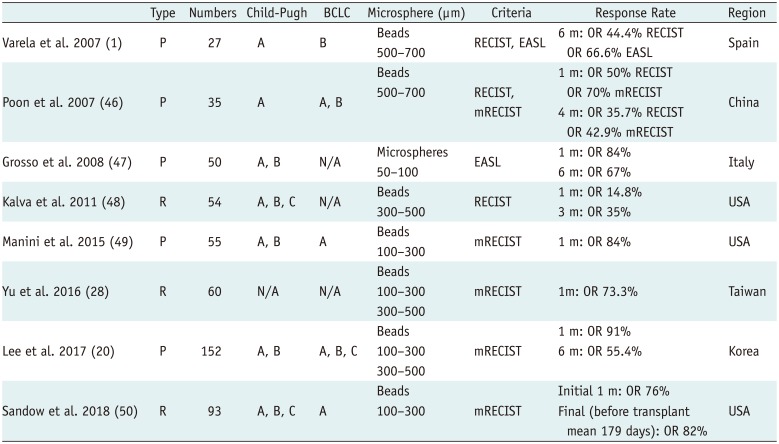
Initial clinical studies confirmed an association between favorable pharmacokinetic profiles of microspheres and good tumor response (Table 5). Objective response rates, defined as the percentages of patients who achieve complete or partial response according to the modified Response Evaluation Criteria in Solid Tumors (RECIST) guidelines, have been found to range from 66.6% to 76.8% (Fig. 4) (14647). Since the initial reports, multiple clinical trials have reinforced the use of DEM-TACE in patients with HCC (20284849). However, clinical results depended on many factors, including cancer stage, number of patients, type and size of microsphere, and follow-up duration.
In a recent Korean prospective multicenter clinical trial using DEB-TACE among 152 patients, 103 (67.8%) had a Child-Pugh class of A5, 114 (75.0%) had a performance status of 0, and 77 (50.7%) had stage A disease according to the BCLC classification (20). One month after treatment with doxorubicin-loaded DC Bead®, the complete and objective response rates were 40.1% and 91.4%, respectively. Among the 121 patients who were analyzed at 6 months, the complete and objective response rates were 43.0% and 55.4%, respectively (20).
Yu et al. (28) conducted a prospective study of the effects of DEB-TACE in 60 patients with HCC who were evaluated before liver transplantation. Following initial DEB-TACE with DC Bead®, 40% achieved complete response and 33.3% achieved partial response according to the modified RECIST guidelines; among these, 15% had stable disease and 11.7% had progressive disease (Fig. 5). No patient experienced major complications or hepatic failure after the procedure. Of the 23 patients who initially did not meet the University of California San Francisco criteria for liver transplantation, 17 (73.9%) were successfully downstaged following DEB-TACE. The high percentage of patients who experienced tumor necrosis with minimal discomfort and without major complications suggests that DEB-TACE may be a safe and effective bridge therapy to liver transplantation in patients with HCC and poor liver function (28).
A retrospective single-center cohort analysis was conducted among 93 consecutive patients between 2011 to 2016 who underwent DEB-TACE using 100–300 µm LC Bead® (BTG) before liver transplantation (50). This showed a favorable long-term treatment response in 87% of patients with histologically low-grade tumors (grades 0–2), including complete and partial response rates of 49% and 38%, respectively. Incontrast, only 33% of patients with histologically high-grade tumors (grades 3–4) responded, with complete and partial response rates of 0% and 33%, respectively (p = 0.001) (50).
Complications, Safety, and Survival
Drug-eluting microsphere transcatheter arterial chemoembolization is a safe procedure for patients with HCC, with reports showing low rates of serious complications (1.6–7.2%) (2051). These complications included hepatic insufficiency or infarction, liver abscess, tumor rupture, bile duct injury, cholecystitis, upper gastrointestinal bleeding, pleural effusion, pulmonary embolism, splenic infarction, and spinal embolization. In contrast, minor procedural complications are more frequent, most being associated with the post-embolic syndrome. These complications are observed in 30.2–67.6% of patients and include fever, nausea and vomiting, and abdominal pain (2052). In addition, the incidence of bile duct injury has been reported to be higher in patients with HCC treated with DEMTACE than in those treated with c-TACE (53). This biliary complication may be due to stasis of the microspheres when there is complete embolization of the feeding artery (20).
Although chemotherapeutic drugs are typically accompanied by systemic complications, including fatigue, fever, gastrointestinal symptoms, neurological injury, pulmonary edema, bone marrow suppression, pulmonary edema, and cardiomyopathy, these are rarely observed in patients treated with DEM-TACE (2026). Indeed, it seems that the characteristic pharmacokinetics of DEM-TACE result in much lower systemic concentrations of doxorubicin compared with c-TACE (13567).
Notably, according to recently published studies, the 30-day mortality rates in patients treated with DEM-TACE ranged from 0% to 1.2% (5455). Whereas the median overall survival periods were 43.8–54 months, the 1-, 2-, 3-, 4-, and 5-year survival rates were 88.2–93.6%, 83.8%, 62.0–67.8%, 41.04–54.2%, and 33.9–39.4%, respectively (5456575859).
C-TACE Versus DEB-TACE
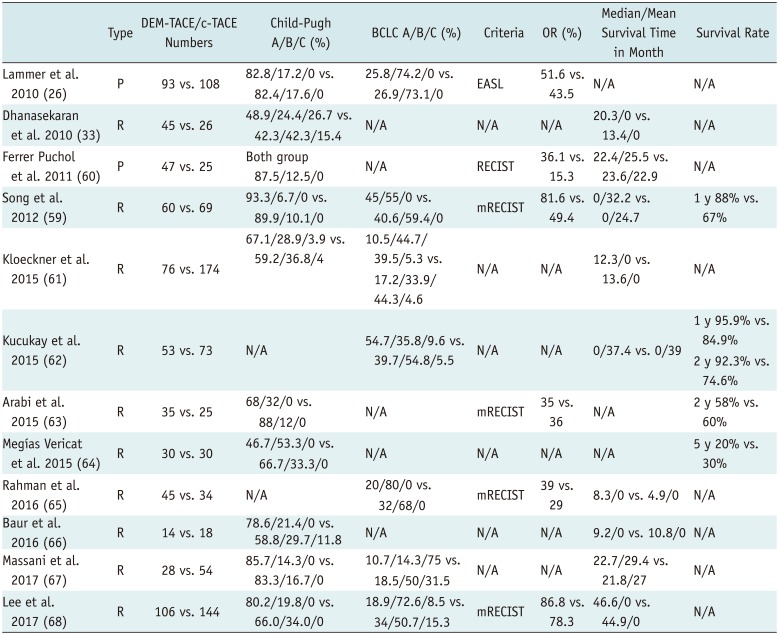
Since DEB-TACE first became commercially available in 2006, many clinical trials have shown its efficacy in patients with HCC and its ability to overcome the drawbacks of c-TACE (Table 6) (263359606162636465666768). DEB-TACE has, therefore, been used in some institutions as a first-line treatment in addition to c-TACE for the treatment of HCC in patients who are ineligible for curative treatment.
In the original research, DEB-TACE produced major tumor necrosis while reducing the side effects of chemotherapy due to the reduced passage of chemotherapeutic agents into the systemic circulation. Although good results were obtained with a mean doxorubicin dose of 128 mg (range, 47–150 mg), the systemic concentrations of doxorubicin were significantly lower in patients treated with DEB-TACE than in those treated with c-TACE (1). Similarly, a prospective single-blind, randomized phase II study of 30 patients with unresectable HCC treated with c-TACE or doxorubicin-eluting HepaSphere™ microspheres showed that the latter had a superior toxicity profile to c-TACE (12). The multicenter, prospective, randomized, single-blind, phase II PRECISION V trial of 212 patients reported objective response rates of 51.6% with DC Bead® and 43.5% with c-TACE (26). However, the overall rates of treatment-emergent complications and serious liver toxicity after embolization were lower among patients treated with DC Bead® than in those treated with c-TACE. These findings indicate that, although the two methods did not significantly differ in efficacy, DEB-TACE was better tolerated and allowed treatment to be repeated in these more vulnerable patients (26).
A retrospective study involving 71 patients reported that DEB-TACE provided a survival advantage over c-TACE, with subgroup analysis showing clear survival benefits in patients with Okuda stage I tumors, Child-Pugh classes A and B disease, and a Cancer of Liver Italian Program score of ≥ 3 (33). However, the safety profiles of the two modalities were similar (33). In another retrospective study involving 129 patients, DEB-TACE with DC Bead® resulted in superior treatment response and delayed tumor progression compared with c-TACE; however, there were no significant differences in treatment-related hepatic toxicities (59).
Liu et al. (69) also showed high safety and efficacy profiles for DEB-TACE compared with c-TACE. In a retrospective study involving 158 patients with HCC, 64 (40.5%) received TACE with lipiodol-doxorubicin and gelatin sponges (Group A), 41 (25.9%) received TACE with lipiodol-doxorubicin and microspheres (Group B), and 53 (33.5%) received TACE with doxorubicin-loaded DEBs (Group C). The study found that more patients in Group C (32.1%) achieved complete response than did those in either Group A (6.3%) or Group B (2.4%) (p < 0.001). Minor complications were also more common in Group A (54.7%) and Group B (34.1%) than in Group C (5.7%) (69).
In contrast to these data, a meta-analysis of seven studies (n = 693 patients) comparing the efficacy of DEB-TACE and c-TACE revealed that tumor response did not differ significantly among methods (70). However, it was conceded that additional large-scale, randomized, controlled studies are required (70). More recent meta-analyses have included multiple randomized controlled trials, prospective studies, and retrospective studies have also shown conflicting results. In a meta-analysis of seven clinical studies (n = 700 patients), Huang et al. (71) showed that tumor response was significantly better, and that the 1- and 2-year survival rates were significantly higher for DEB-TACE than for c-TACE. Xie et al. (72) also performed a meta-analysis of four randomized controlled trials, one uncontrolled prospective study, and one prospective case-control study (n = 652 patients). They reported similar overall survival rates between c-TACE and DEB-TACE, but that the latter was associated with a significantly higher objective response rate and a slightly lower incidence of complications (72). Chen et al. (73) performed a large meta-analysis of 1832 patients and found that DEB-TACE had higher 1-, 2-, and 3-year overall survival rates, and higher 1- and 2-year relapse-free survival rates. Finally, a meta-analysis involving 1449 patients found no significant differences in the 1-, 2-, and 3-year overall survival and complications rates between c-TACE and DEB-TACE (74).
A recent retrospective study included 82 non-surgical patients with HCC who underwent c-TACE or DEB-TACE and performed follow-up for a minimum of 12 months (67). In the DEB-TACE group, they used beads measuring 100–300 µm in diameter that were loaded with 50 mg of doxorubicin. Although the two methods showed similar efficacy, DEB-TACE was better tolerated, with survival mainly affected by preserved liver function (67). Another retrospective study comparing the clinical outcomes of DEB-TACE and c-TACE in 250 consecutive patients showed comparable treatment outcomes (68). Moreover, it not only failed to identify clinical factors that could help when choosing between these treatment modalities but also showed that tumor size was not associated with treatment outcomes in either group. However, because DEB-TACE showed a better safety profile when used to treat large carcinomas, it was recommended that its role should be further examined in patients with HCC at risk of aggravated liver function after treatment with c-TACE (68).
A retrospective comparison of survival outcomes was recently performed in 313 patients with unresectable HCC treated with two different TACE regimens: a c-TACE regimen with three drugs and a DEB-TACE regimen with a single drug (75). Interestingly, it showed no significant difference in survival between the two, though patients who underwent DEB-TACE had shorter hospital stays (75).
Together, these conflicting findings indicate that the comparative efficacy, safety, and survival rates of DEB-TACE and c-TACE remain unclear. However, DEB-TACE has consistently been shown to have superior pharmacokinetic proprieties and lower rates of systemic chemotherapy-associated toxicity, making it the more tolerable option when compared to c-TACE. Based on the current evidence, DEB-TACE may be the superior option when treating patients who are vulnerable or in whom we anticipate deterioration after locoregional chemotherapy.
Strategies for Improving DEM-TACE
Small-Sized Microspheres
Smaller caliber microspheres (< 100 µm) may provide better outcomes, with evidence that they show greater distal penetration and more effective embolization than larger microspheres, without influencing patient safety. An animal study of distal embolization showed that occlusion was more distal and that microsphere distribution in the embolized territory was denser when using 30–60-µm rather than 50–100-µm HepaSphere™ microspheres (76). Moreover, the tissue concentration of doxorubicin was higher after embolization with the smaller beads, while the plasma concentration remained very low (76). HepaSphere™ microspheres of dry caliber 30–60-µm are loadable and expand to 120–240 µm in saline and to 96–192 µm after loading with doxorubicin (76). Use of such microspheres in 45 patients who had intermediate stage HCC or who were ineligible for curative treatment produced a local objective response rate of 68.9% in patients who received an intended doxorubicin dosage of 50–100 mg, with an overall complete response rate of 17.8% (Fig. 6) (13). That study also showed very low complication rates, with no deaths or grade 5 complications at 30 days (13). In contrast, the use of larger HepaSphere™ microspheres resulted in lower objective and complete response rates (56% and 12.6%, respectively) (77). Moreover, the complication rates were lower than previously reported for periprocedural mortality (3%) and post-embolic syndrome (18.54%) with other DEMs (47).
An animal study found that beads ranging in diameter from 70 µm to 150 µm are associated with greater tumor coverage, more distal penetration, and higher doxorubicin concentrations in the tumor, without increasing systemic exposure, than is c-TACE (78). An evaluation of the efficacy of 70–150-µm DEBs (M1 DEB) in 45 patients with HCC who were undergoing TACE as either a primary therapy or as a bridge to liver transplantation reported an objective response rate of 77.7% and a median time to best response of 3 months (95% confidence interval: 2–4 months) (Fig. 7) (79). In 13 patients, DEB-TACE served as an effective bridge, downstaging the tumor to make it eligible for liver transplantation or surgery. Pathological examination also revealed more than 90% necrosis in 10 of the 28 nodules. The most common mild complications (grade 1 or 2) were post-embolic syndrome and abdominal pain, each of which occurred in 4.4% of patients. The only serious complication (grade 3) was bleeding from esophageal varices, which was observed in a patient after portal hypertension worsened; however, this patient was treated conservatively and recovered fully within 1 month (79).
A recent retrospective study involving 421 patients with HCC who underwent DEB-TACE using 70–150 µm DC Bead® (M1) showed that the overall objective response rates were 94.5% and 99.5% at 3 and 6 months, respectively (55). These rates were higher than those in a previous multicenter randomized controlled trial (26) using DEB-TACE particles of 300–500 µm and 500–700 µm in diameter, where the objective response rate was 52% at 6 months. No patient experienced treatment-related bleeding, pulmonary complications, or death (55). However, embolization with larger particles has been associated with a 30-day mortality rate of 1.2% (2 of 173 patients died due to procedure-related liver abscess or sepsis) (54) and 10 major complications among 104 patients (3 abscesses and 1 death) (56).
Microcatheter Super-Selection
A successful delivery of loaded microspheres to tumors, while minimizing complications, requires super-selection of the feeding artery to avoid damage of non-targeted arteries. Several recently developed techniques have sought to achieve this goal.
In one report, detachable microcoils were used to divert blood flow temporarily in a patient who was undergoing DEB-TACE for a recurrent HCC in segments 8 and 4 after previously undergoing left hepatectomy (80). The recurrent tumor had a small feeding artery arising at an acute angle from the proximal right hepatic artery. Two microcatheters were inserted: the first in the right hepatic artery distal to the opening of the branch vessel supplying the residual tumor and the second in the proximal right hepatic artery, proximal to the ostium of the feeding artery. A 5-mm detachable coil was subsequently loaded through the distal catheter and deployed in the right hepatic artery, followed by the infusion of DC Bead® (80).
Similarly, a double-lumen microballoon catheter with a side hole at the leading end of the balloon was used to infuse chemotherapy during c-TACE in the treatment of HCC, although without super-selective catheterization of the target artery (81). This technique enabled prompt infusion of chemotherapeutic agents into the target artery via distal occlusion of the parent artery, with the distal occlusion ensuring the preservation of a broad area of normal hepatocytes.
Radio-Opaque Microspheres
Mixing nonionic contrast with loaded beads is essential for direct fluoroscopic monitoring and is typically achieved using drug-eluting radio-opaque beads (8283). LC Bead LUMI™ microspheres are sulfonate-modified polyvinyl alcohol hydrogel micro-beads that measure 70–150 µm in diameter and contain covalently bound iodine (83). Their radio-opacity allows for the real-time assessment of their deposition in the target tumor. Theoretically, the density and distribution of the radio-opaque beads can provide additional information to refine the embolization endpoint and the degree of flow stasis. This allows a better prospective visualization of non-target reflux and small branch feeders. Moreover, contrast retained by DEBs in dense vessels is typically washed out within minutes of the procedures, ensuring a lack of peripheral contrast retention, which has been reported to be a risk factor for treatment failure (84). Performing non-enhanced CT scan immediately to assess contrast retention after embolization may provide important information about treatment (85). The visibility of radio-opaque beads may also provide additional information about the expected effects of treatment, follow-up, and planning for the next session, as required.
Conclusion
Most patients with HCC are diagnosed with intermediate stage tumors, making curative treatment unavailable. Although c-TACE has been considered the treatment of choice for these patients, it has several limitations. DEM-TACE, was therefore, developed to overcome the drawbacks typically associated with c-TACE. Although studies comparing the safety and effectiveness of these methods have failed to show statistically significant superiority with the use of DEM-TACE, this method is considered more tolerable because it eliminates the toxicity associated with systemic chemotherapy. Further improvements in embolization techniques and microsphere types, including a better delineation of the optimal size, are needed to improve the efficacy of DEM-TACE and to widen its applications.




 XML Download
XML Download