

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the incidence is unknown and variable occurrence has been documented in the literature (1), bone tunnel widening after anterior cruciate ligament (ACL) reconstruction is well established (23456). It occurs predominantly during the first six months after surgery and has been documented up to two years postoperatively (1378910). Some authors report a decrease in tunnel diameter three years after surgery (3).
There have been debates on the clinical relevance of bone tunnel widening after ACL reconstruction. Although many studies showed no effects of bone tunnel widening on clinical outcomes or objective laxity (358911121314), a few investigations demonstrated that it might be associated with anterior knee laxity and an early sign of graft failure (1516). Thus, the clinical significance of bone tunnel widening has not yet been fully established and is still unclear.
However, bone tunnel widening has usually been assessed with plain radiographs, which are easily accessible and widely acceptable to both clinicians and radiologists (17). However, it is not enough to evaluate bone tunnels exactly and reproducibly, especially when multiple tunnels exist in a single bone (for example, double-bundle reconstruction). Although a number of studies used cross-sectional imaging tools such as computed tomography (CT) or magnetic resonance imaging (MRI) to evaluate bone tunnel widening (121317), they could not measure the tunnel diameters exactly because they used only conventional orthogonal planes, which could not be parallel or perpendicular to the axes of the bone tunnels. As such, we decided to conduct this study using CT with multiplanar reconstruction (MPR) along the axis of each tunnel in patients who underwent double-bundle ACL reconstruction. We hypothesized that the bone tunnel widening might be correlated with clinical findings. The aim of the study then was to evaluate the correlation between the bone tunnel diameters in patients who had undergone double bundle ACL reconstruction, measured by CT using MPR, and their clinical scores and stability.
MATERIALS AND METHODS
Patients
This retrospective study was approved by the Institutional Review Board, and informed consent was waived.
A cohort of 329 consecutive patients who had undergone primary arthroscopic ACL reconstruction using the double-bundle technique at a referral hospital between July 2011 and April 2013 were identified by searching the electronic medical records by one of the authors. Among them, we included patients who had had ACL reconstruction using double-bundle auto-hamstring tendon grafts with available immediate postoperative CT images, follow-up CT images, and clinical scores and stability examined within 40 days before or after follow-up CT imaging. In our institute, immediate postoperative CT images were usually obtained for evaluating the location and angle of bone tunnel in addition to evaluating immediate postoperative complications.
Twenty-five patients who did not receive immediate postoperative CT scans and 239 patients who did not have follow-up CT scans were excluded. Eighteen patients who underwent clinical scoring more than 40 days after follow-up CT imaging were also excluded. Finally, 47 patients (41 men and 6 women, 20 left and 27 right knees) were enrolled. The mean age of the patients was 34 years (range: 15-60) at the time of surgery.
Arthroscopic Procedure
All ACL reconstructions were performed by one subspecialty trained arthroscopic orthopedic surgeon (who at the time had 12 years of experience in arthroscopic ACL reconstruction). Preparation and arthroscopic examination were performed in the usual manner. From the ordinal anteromedial arthroscopic view, the femoral footprints of the anteromedial and posterolateral bundles of the ACL were carefully defined by the ACL remnant or bony anatomy, and the centers of each footprint were marked with a microfracture awl. After arthroscopic examination, the semitendinosus and gracilis tendons were harvested, and each tendon was prepared as a triple (three-stranded) graft. The graft made by the semitendinosus tendon was then used to reconstruct the anteromedial bundle, and the graft made by the gracilis tendon was used for the posterolateral bundle. The drill diameters of the femoral and tibial tunnels were decided based on the diameter of the prepared graft. The grafts were fixed by a cortical suspensory device for the femoral side and bioabsorbable interference screws with a post-tie for the tibial side.
CT Imaging
CT images were obtained with a 64-section CT scanner (LightSpeed VCT, GE Healthcare, Milwaukee, WI, USA). The parameters for image acquisition and reconstruction were as follows: 120 kVp, collimation width of 0.625 mm, acquisition matrix of 512 × 512, amperage of 100 mA to 120 mA, field of view of 150 mm to 170 mm adapted to each patient, reconstruction thickness of 0.625 mm, and standard reconstruction algorithm. Immediate postoperative CT scans were performed an average of 2.5 days (range: 1-4 days) after surgery. Follow-up postoperative CT scans were performed an average of 410.4 days (range: 297-644 days) after surgery. Both immediate postoperative and follow-up CT scans were performed according to the referring surgeon's postoperative patient management protocol and were not confined to symptomatic patients.
Image Evaluation
CT assessments were independently performed by the two fellowship-trained musculoskeletal radiologists, who each had five years of experience and who were blinded to clinical score or stability status. Both observers measured twice with an interval of more than four weeks to calculate intra-observer agreement. The reconstructed CT data were loaded into a workstation. MPR and measurements were accomplished simultaneously with dedicated software (Aquarius NET 0.4.4.7; TeraRecon, San Mateo, CA, USA). At first, reformatted images were displayed in the axial, coronal, and sagittal planes automatically on the viewer. Next, observers made dedicated longitudinal planes according to each bone tunnel (two femoral and two tibial) using MPR tools. They recorded the diameters of each tunnel on both the immediate postoperative CT (T1) scans and the follow-up CT (T2) images at five points (proximal end, mid-portion, distal end, one-quarter, and three-quarter portion), and their mean value was regarded as the diameter of each bone tunnel (Fig. 1).
Clinical Assessment
To evaluate stability, bilateral knee joints were examined using a single-calibrated arthrometer (KT-2000, Medmetric Corp., San Diego, CA, USA) with constant forces of 15, 20, and 30 lbs. and manual maximum displacement by a physical trainer with five years of arthrometry experience at the time of the test who was blinded CT imaging findings, International Knee Documentation Committee (IKDC) results, and clinical history. Measurements were calculated with a force of 30 lbs., and a difference between the treated knee and the contralateral uninjured knee equal or less than 3 mm was designated as normal, whereas a difference of more than 3 mm was recorded as abnormal (1819). Knee joint functional scores were evaluated using IKDC objective and Lysholm knee scales, which were designed for knee ligament injuries.
Statistical Analysis
The differences in T1 and T2 for each tunnel were tested by a linear mixed-effect model with Bonferroni's correction after adjustment to the time interval between T1 and T2. A p value less than 0.05 was regarded as statistically significant. The correlations of (T2 - T1) / T1 and T2 for each of the four tunnels, with KT-2000 result, Lysholm score, and IKDC objective score, were analyzed using a Spearman partial correlation analysis after adjustment for patient sex, age, side (right/left), and time interval between T1 and T2. Corrected p values less than 0.05 were regarded as statistically significant. The concordance correlation coefficient was used to assess intra- and inter-observer variability (95% confidence interval). Observer agreement was categorized as poor (< 0.40), moderate (0.40-0.75), or excellent (> 0.75). All statistical analyses were executed using SAS version 9.3 (SAS Institute, Cary, NC, USA).
RESULTS
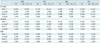
Table 1 shows the diameters of each bone tunnel on both immediate postoperative CT (T1) and follow-up CT (T2) and the ratio of the change in diameter between T1 and T2 ([T2 - T1] / T1). The difference between T1 and T2 for the tibial bone tunnel for the anterior medial bundle (TAM) was statistically significant (observer 1, 0.578 mm to 0.698 mm, p value of < 0.001; observer 2, 0.581 mm to 0.707 mm, p value of < 0.001). There were no statistically significant differences between T1 and T2 for the other bone tunnels. There were 42 normal and 5 abnormal results for KT-2000. IKDC scoring placed 11 in group A (normal), 17 in group B (near normal), 14 in group C (abnormal), and 5 in group D (severely abnormal). The mean Lysholm score was 89.42 ± 8.67. Spearman partial correlation analysis showed that neither the T2 nor the (T2 - T1) / T1 of either observer had a significant relationship with clinical scores (corrected p value of 1) (Table 2). Intraobserver agreement for the measurements was excellent (> 0.8) for both observers. Interobserver agreement for measurement was excellent (> 0.8) except for the most distal portion of the femoral bone tunnel for anterior medial bundle in immediate postoperative CT, which showed moderate agreement (concordance correlation coefficient = 0.6311).
DISCUSSION
The principal findings of this study were that only the tibial bone tunnel for anteromedial bundle was significantly widened on follow-up CT and that the diameters of the bone tunnels on follow-up CT and their change ratios were not correlated with stability or clinical scores.
It has been reported that as many as 10% of these patients may experience graft failure and recurrent instability (4). Therefore, the increased number of ACL reconstructions being performed has led to an increased demand for postoperative imaging evaluation (1820).
Bone tunnel widening is a well-established procedure after ACL reconstruction; however, its etiology is still unknown, and a multifactorial process including biological and mechanical theories has been proposed as an explanation (2345621). Biologic factors include increased cytokine levels caused by the immune response or inflammatory response caused by synovial fluid leakage within the bone tunnel (1222). Mechanical factors include the types of graft and devices, the location of the graft, and the presence and degree of stress shielding proximal to the interference screw that results in bone resorption (23421). Regarding this issue, a previous study reported that the extra-cortical fixation of the graft is associated with more laxity and significantly more tunnel enlargement than that of close-to-joint fixation (23). Although bone tunnel widening with fibrotic tissue proliferation has been known to be a clinically significant finding that may complicate revision surgery, many clinical studies failed to demonstrate an association between bone tunnel widening and instability or prevalence of post-traumatic osteoarthritis after ACL reconstruction (1232124). In terms of imaging modality, conventional radiographs and CT have been studied (1121317). In daily practice, measuring bone tunnel diameter has been subjective with the use of conventional radiographs. They are widely used as the primary modality, but they cannot show the bone tunnel consistently because they only provide two-dimensional images (225). Although CT imaging has been regarded as a reliable imaging modality for evaluating ACL bone tunnels, as proven by superior intra- and interobserver agreement compared with radiographs (1), MPR for the axis of each bone tunnel is mandatory for exact measurement. To the best of our knowledge, this study marks the first attempt to evaluate bone tunnel widening using MPR with CT images, and it shows excellent intra-observer and moderate to excellent inter-observer agreement. In this study, the bone tunnel widening on follow-up CT images was statistically significant at TAM only. Because of the lack of previous studies on this topic, we cannot entirely explain it; however, we postulate that the TAM could be exposed to much more mechanical stress because of its longer length and extra-cortical fixation in our enrolled patients.
To estimate knee stabilities, we performed objective testing using a KT-2000 arthrometer. Additionally, all patients were assessed according to Lysholm scores, which have been validated for functional scoring of knee ligament injuries; however, their use may lead to overestimating subjective parameters, and existing problem areas may not be sufficiently judged (19). Therefore, we added IKDC objective scores. The current study showed no statistically significant correlations between diameters and their change ratios for each bone tunnel as measured on follow-up CT images and clinical scores with a mean follow-up of 13.5 months (range: 10-22 months); these results are similar to those from previous studies. Nevertheless, the strengths of the current study are thought to be the homogenous patient group who were treated with a double-bundle auto-hamstring tendon graft and compared with clinical scores as well as stability in terms of KT-2000.
This study has a number of limitations. First, variable follow-up periods caused by the retrospective nature of the study could have resulted in low correlations between measurements and clinical scores. Second, only the patients who underwent both immediate postoperative and follow-up CT scans were enrolled, which might have increased the possibility of selection bias. Third, the lack of a long-term follow-up should also be a limitation. Fourth, we could not evaluate the nature of bone tunnel widening such as bone tunnel cyst formation or fibrosis. Finally, we could not evaluate the status of ACL grafts and other structures such as cartilage, meniscus, and other ligaments that could influence clinical outcomes because of the suboptimal soft tissue contrast of CT images. Additional studies that use MR imaging with three-dimensional isotropic fast spin echo sequences may be needed to evaluate all structures including the graft and the nature of the bone tunnel widening and for objectively measuring bone tunnels with MPR in the future.
In conclusions, neither the diameter nor its change ratio during the interval follow-up is correlated with stability or clinical scores.


 XML Download
XML Download