

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recently, breast magnetic resonance imaging (MRI) has been accepted as an important tool for the characterization of breast lesions (1), and its clinical use has become more widespread such as for the screening in high risk groups and in women with augmentation or cosmetic injection, local staging in patients with newly diagnosed breast cancer, evaluation of positive surgical margin at initial excision and for the response monitoring to neoadjuvant chemotherapy. Notwithstanding a relatively small field of view (FOV) and primarily focusing on the mammary glands and axillary regions, a part of other structures such as the lung, mediastinum, upper abdomen and bony thorax are included in breast MRI also (2, 3). Preoperative breast MRI is usually used for local staging such as the assessment of breast cancer extend and the evaluation of the contralateral breast, however, the lesions detected on the extra-mammary structures in that FOV can influence the staging. Irrespective of the nature of extra-mammary findings (2, 3), the detection of those findings is important, because it can be a clue of systemic metastasis or concurrent malignancy. Therefore, radiologists should pay attention not only to mammary and axillary regions but also to all the structures included in the FOV of breast MRI. The purpose of this pictorial essay was to review extra-mammary findings observed in preoperative breast MRI examinations of breast cancer patients.
Lung Lesions
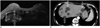
It is known that incidentally detected lesions of lung parenchyma are highly likely to be malignant compared to lesions in other structures (4). Unexpected pulmonary nodules detected on breast MRI in patients with breast cancer are identified as one of a large spectrum of abnormalities ranging from benign to malignant lesions. The rates of these abnormalities have been reported with 34.2-75% for metastatic lesions, 11.5-48.1% for primary lung cancer and 13.5-17.7% for benign lesions (5). CT and MRI share similar criteria for raising suspicion of a malignant nature of lung nodules, such as multifocality and increase in the size and number of the nodules on follow-up examinations (6). A CT is advantageous in discriminating the nature of lung nodule(s) concerning the assessment of shape, border and density. Therefore, a CT should be considered for the differential diagnosis if the incidental lung nodule(s) are detected on breast MRI (6). We have found three cases of lung abnormalities (Figs. 1,2,3) on breast MRI. In two of them were the treatment plans changed after MRI. In one case was an incidental lung mass found in the right upper lobe (Fig. 1A) on breast MRI and this did not change on the two-year follow-up chest CT (Fig. 1B). In the second case, incidental pleural lesions with pleural effusion which were confirmed as metastases were found in the left hemithorax (Fig. 2A, B). A chest CT showed multiple pleural masses with a large amount of pleural effusion (Fig. 2C). The plan of direct operation was changed to chemotherapy after this detection. In the third case, primary lung cancer was confirmed and a simultaneous lobectomy was conducted (Fig. 3).
Mediastinal Lesions
When a unexpected mediastinal mass is found, the differential diagnosis can be narrowed based on the location within the mediastinal compartment and by age (7). Most masses (60%) located in the mediastinum are thymomas, neurogenic tumors or benign cysts. As most mediastinal cysts are developmental in origin (Fig. 4), there is no need to delay a breast cancer operation. Many mediastinal lesions, such as mediastinal lymph nodes, vascular abnormalities (e.g., aneurysms) and normal structures (e.g., pericardial recess, pericardial fat pad) can be observed on breast MRI. Normal structures can be mistaken as mediastinal mass as we obtain breast MRI with the patient in a prone position. For example, prominent pericardial fat can be seen as a contour-bulging mass in the anterior mediastinum (Fig. 5A, B). The bulging contour can be changed to a straight line on CT images (Fig. 5C) by supine positioning the patient. In addition, as this is a fat pad around the pericardium, the fat signal drops with a fat-suppressed scan. Mediastinal lymph nodes certainly represent the most common cause of mediastinal masses. A positron emission tomography (PET) for systemic evaluation should be considered if mediastinal lymph nodes are found on breast MRI (Fig. 6A, B) and CT for local staging (Fig. 6C), because the management strategy may be changed according to the status of regional lymph nodes (Fig. 6D).
Liver Lesions
The most frequent extra-mammary findings on breast MRI are hepatic lesions (2). Most hepatic lesions are benign and the probability of a hepatic lesion being malignant is less than 20% (2, 8). Further examinations must rely on any suspicious characteristics observed on the MRI, such as the presence of multiplicity (Figs. 7, 8), indistinct margins (Fig. 8) or rim enhancement (Fig. 8) on both, unenhanced and enhanced sequences. Further evaluation is not necessary if the lesions have typical findings such as those of a simple hepatic cyst, which show a high signal intensity on T2-weighted images (Fig. 7A) and no internal or rim enhancement (Fig. 7B) after contrast injection (9). However, further evaluation should be conducted (e.g., nuclear scan or CT with a liver protocol or MRI with a hepatobiliary contrast agent) if the findings are not typical for benign lesions. We report a case of left breast cancer which was widely excised at another hospital. The MRI showed numerous high signal-intensity masses on T2-weighted images, which lesions were not enhanced at all after contrast injection and suggestive of hepatic cysts. Then a subsequent lumpectomy of the left breast followed (Fig. 7). In another case with right breast cancer, multiple masses with high signal intensity on T2-weighted images (Fig. 8A) and low signal intensity on T1-weighted images (Fig. 8B) were seen, which exhibited enhancement after contrast injection (Fig. 8C, D). So, operation was cancelled and treatment plan was changed to chemotherapy.
Bony Lesions
Bony lesions are occasionally observed on breast MRI. More attention should be given to bony lesions, because bone is one of the most common sites for breast cancer metastasis (2, 10, 11). An early detection of metastatic disease may change treatment plans and offer a better chance of survival and quality of life. Approximately 65-75% of patients with metastatic disease from breast cancer have bone metastases (10). In a recent study, bone lesions accounted for 7% (20/285) of all incidental extra-mammary findings in breast cancer patients, and the positive predictive value for MRI to detect a metastatic lesion was high if it was located within the bone (89%) (11). Signal changes in the marrow on T1-weighted images are the most frequently observed findings. However, these findings are nonspecific and observed on both, benign (e.g., inflammation or stress fractures) (Fig. 9) and malignant lesions (Fig. 10). Typical features of bone metastases include a low signal intensity on T1- and a high signal intensity on T2-weighted images with peripheral edema of the bone marrow (Fig. 10) (2). Therefore, MRI with a bone protocol, bone scan or PET should be recommended if bony lesions were detected on breast MRI in patients with breast cancer.
CONCLUSION
Breast MRI is one of the most useful imaging modalities for the detection and characterization of breast lesions. With the widespread use of breast MRI, incidental extra-mammary findings are detected more often than before. Radiologists should pay attention not only to breasts but also to extra-mammary areas, because the prevalence of malignant incidental extra-mammary findings is not negligible and these might alter the treatment plan, particularly for breast cancer patients. The awareness of extra-mammary findings on breast MRI may lead to an early detection and appropriate management of extra-mammary findings in patients with breast cancer.









 XML Download
XML Download