

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hyperglycemia is common in critically ill patients irrespective of the presence of diabetes mellitus,1 which is called stress hyperglycemia. Stress hyperglycemia has been regarded as a poor prognostic factor influencing morbidity and mortality of critically ill patients. The mechanism has been explained by stress hormone secretion, which reflects severity of the disease,23 and by the hyperglycemia itself, which exacerbates the cytokine, inflammatory, and oxidative stress response, potentially setting up a vicious cycle.45 Previous studies conducted in various critically ill patients showed that admission blood glucose (BG) level was related to prognosis6; however, most previous studies regarding cardiovascular disease focused on acute coronary syndrome7 or decompensated heart failure.8 Furthermore, the prognostic role of BG level may differ in diabetic versus non-diabetic patients because BG level inevitably depends on the degree of glucose control with glucose-lowering strategies in diabetic patients. Several studies have reported that hyperglycemia is associated with clinical outcomes irrespective of the presence of diabetes mellitus,9 while some studies have reported that the relationship was valid only in non-diabetic patients.7 Meanwhile, there are concerns that mild to moderate stress hyperglycemia might be protective since it could provide a source of fuel for the immune system and brain and contribute to the survival of critically ill patients.10 Therefore, we sought to investigate the association between admission BG level and clinical outcomes in critically ill patients with various cardiovascular diseases who were admitted to cardiac intensive care unit (CICU) according to the presence or absence of diabetic mellitus.
METHODS
Study population
We consecutively screened patients who were admitted to the CICU in Samsung Medical Center from January 2013 to December 2015. There were 2,923 patients admitted to the CICU of our hospital during the study period. We excluded 492 patients admitted to the CICU due to diseases other than cardiovascular problems and 651 patients who did not have admission BG level data. Finally, 1,780 patients were included in this study (Fig. 1). Then, we classified study populations by clinically important glucose levels according to the guidelines from American Diabetes Association11; group 1 (< 7.8 mmol/L), group 2 (7.8 mmol/L to 10.9 mmol/L), group 3 (11.0 mmol/L to 16.5 mmol/L), and group 4 (≥ 16.6 mmol/L).

Definitions and outcomes
Underlying diseases including hypertension, cerebrovascular disease, chronic kidney disease, liver cirrhosis, and malignancy were extracted from the electronic medical records. Diabetes mellitus was diagnosed at a fasting BG level ≥ 7.0 mmol/L or a random glucose level ≥ 11.1 mmol/L or glycated hemoglobin ≥ 6.5%.12 Patients who were taking insulin or oral hypoglycemic agents were also defined as having diabetes mellitus. For evaluation of disease severity, we calculated acute physiology and chronic health evaluation II (APACHE II) scores of study participants. Admission BG level was defined as the maximum serum glucose level within 24 hours of CICU admission.
The primary outcome was CICU mortality. Use of intra-aortic balloon pump, extracorporeal membrane oxygenation, mechanical ventilator, renal replacement therapy, or heart transplantation was also assessed.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation, and categorical variables were expressed as frequency and percentage. Continuous variables between non-diabetic and diabetic patients were compared using the t-test or Mann-Whitney U test. Categorical variables were compared using χ2 or Fisher's exact tests. Event-free survival was estimated by the Kaplan-Meier method and was compared using the log-rank test. Cox proportional hazard regression analysis was performed to evaluate the influence of admission BG level on CICU mortality in non-diabetic patients and diabetic patients. Parameters that were revealed to influence patient outcomes in the Cox regression model were adjusted in the final model. Disease severity was assessed by APACHE II score, and patients were divided into two groups using the cutoff point of 16.5, which was defined by the Yuden index for multivariable cox regression analysis. We used SAS version 9.4 (SAS Institute, Cary, NC, USA) and R 3.4.0 (R Foundation, Vienna, Austria) for Windows for all statistical analyses, with P < 0.05 considered statistically significant.
RESULTS
Baseline characteristics of the patients
Among the 1,780 patients in this study, 595 (33.4%) had diabetes mellitus; the mean age of patients was 65 ± 14 years. Baseline characteristics are shown in Table 1. The most common cause of admission was acute coronary syndrome (935, 52.5%), and other leading causes were heart failure (434, 24.4%) and cardiac arrhythmia (211, 11.9%). When the cause of admission was compared between non-diabetic and diabetic patients, acute coronary syndrome and heart failure were more common in diabetic patients. APACHE II score and the frequency of shock development during CICU admission were also higher in diabetic patients. The admission BG level for all patients was 10.0 ± 4.8 mmol/L; it was 8.3 ± 2.3 mmol/L in non-diabetic patients and 13.2 ± 5.6 mmol/L in diabetic patients (P < 0.001).
Table 1
Baseline characteristics of non-diabetic and diabetic patients

For purposes of the study, patients were divided into four groups according to admission BG level. The prevalence of shock increased according to admission BG level (11.8%, 22.3%, 40.8%, and 61.9%, P < 0.001 in non-diabetic patients; 18.1%, 19.6%, 25.5%, and 45.5%, P < 0.001 in diabetic patients). APACHE II scores were also higher in the patient group with higher admission BG levels, both in non-diabetic and diabetic patients (P < 0.001, in both). The difference of baseline characteristics by admission BG level is in Supplementary Table 1.
Clinical outcomes according to admission BG level
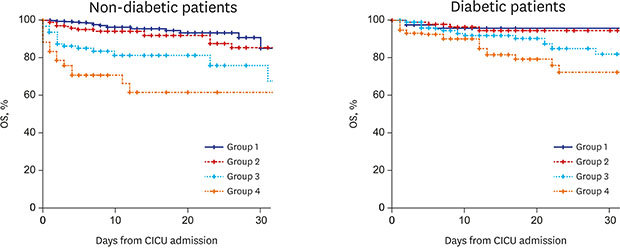
During the study period, median duration of hospital stay was 6 (3–12) days in all patients; it was 5 (3–10) days in non-diabetic patients and 7 (4–15) days in diabetic patients (P < 0.001). Median duration of CICU stay was 2 (1–3) days; 2 (1–3) days for non-diabetic patients and 2 (1–4) days for diabetic patients (P < 0.001). CICU mortality occurred in 105 patients (5.9%), which included 62 (5.2%) non-diabetic patients and 43 (7.2%) diabetic patients (P = 0.105). In non-diabetic patients, the CICU mortality rate was higher in patient groups with higher admission BG levels (1.5%, 5.5%, 15.8%, and 33.3% in groups 1 to 4; P < 0.001). In diabetic patients, although the cumulative CICU mortality gradually increased, it was lacking in statistical significance (3.6%, 3.2%, 7.3%, and 14.2% in groups 1 to 4; P = 0.279) (Fig. 2). The prevalence of patients who received extracorporeal membrane oxygenation, mechanical ventilation, continuous renal replacement therapy, and cardiac transplantation increased with the increase in admission BG level in the non-diabetic patients. However, there was no significant increase in BG level with the use of extracorporeal membrane oxygenation and cardiac transplantation in diabetic patients, unlike mechanical ventilation and continuous renal replacement therapy (Table 2).
Fig. 2
Kaplan-Meier curves for mortality during the follow-up. (A) non-diabetic patients, and (B) diabetic patients. Patients were divided into four groups by admission BG level both in non-diabetic and diabetic patients respectively; group 1 (< 7.8 mmol/L), group 2 (7.8 mmol/L to 10.9 mmol/L), group 3 (11.0 mmol/L to 16.5 mmol/L), and group 4 (≥ 16.6 mmol/L).
OS = overall survival, CICU = cardiac intensive care unit, BG = blood glucose.

Table 2
Frequencies of organ support by the different baseline glucose levels in non-diabetic and diabetic patients

Prognostic significance of admission BG level in non-diabetic and diabetic patients
We performed Cox proportional regression analysis to identify the prognostic significance of admission BG level on CICU mortality in non-diabetic and diabetic patients. Among non-diabetic patients, admission BG level, hypertension, mechanical ventilator support, continuous renal replacement therapy, and APACHE II score were significantly associated with CICU mortality. With group 1 as a reference, adjusted hazard ratios (HRs) of groups 3 and 4 were 3.31 (95% confidence interval [CI], 1.47–7.44; P = 0.004) and 6.56 (95% CI, 2.76–15.58; P < 0.001), respectively. In diabetic patients, continuous renal replacement therapy and APACHE II score were significantly associated with CICU mortality. Although HR for CICU mortality gradually increased in patient groups with an increased admission BG level, the statistical significance was not valid even when mortality was compared between group 1 and group 4 (HR, 1.37; 95% CI, 0.40–4.73; P = 0.616) (Table 3).
Table 3
Multivariable Cox regression analysis of CICU mortality in non-diabetic and diabetic patients
DISCUSSION
In this study, we evaluated the relationship between admission BG level and CICU mortality in non-diabetic and diabetic patients. There was significant association between baseline BG level and CICU mortality in non-diabetic patients, whereas such an association was not valid in diabetic patients. Admission BG level, APACHE II score, use of mechanical ventilator, renal replacement therapy, and hypertension were prognostic factors for CICU mortality in non-diabetic patients, while only APCHE II score and continuous renal replacement therapy were prognostic factors in diabetic patients.
Stress hyperglycemia is thought to be caused by excessive hepatic glucose production and insulin resistance due to the complex interplay between counter regulatory hormones including cortisol, glucagon, growth hormone, and cytokines.313 Since a severe disease status may cause increased stress hormone secretion, hyperglycemia in critically ill patients may be related to more severe disease, which may explain the relation between higher BG level and poor prognosis. In this study, the strong relationship between admission BG level and CICU mortality in non-diabetic patients did not change even when we adjusted for severity of the disease using APACHE II score. The result implies that the relationship between admission BG level and the prognosis of non-diabetic patients is independent from the severity of the disease. This is supported by the finding that hyperglycemia itself in stressful conditions deteriorates endothelial function and promotes pro-inflammatory cytokines.14
The relationship between stress hyperglycemia and prognosis has been documented in various critically ill conditions such as sepsis, postsurgical state, stroke, and trauma.115 Similarly, numerous studies were performed in patients with cardiovascular disease,816 and they showed a strong relationship between BG level and prognosis. However, these studies regarding the association of admission BG level with clinical outcomes focused primarily on patients with acute coronary syndrome171819 and decompensated heart failure.2021 Thus, the results of previous studies were not applicable in the overall critically ill patients with cardiovascular disease. Therefore, in this study, we evaluated the association between admission BG level and clinical outcomes in critically ill patients with cardiovascular diseases including pulmonary thromboembolism, acute aortic syndrome, and cardiac arrhythmia as well as acute coronary syndrome and heart failure in diabetic and non-diabetic patients. Then, we found a significant relationship between admission BG level and CICU mortality in this group of patients, especially those without diabetes mellitus.
In this study, the relationship between admission BG level and CICU mortality was different in non-diabetic and diabetic patients. The relationship in diabetic patients was not significant. Some previous studies have reported that the relationship was valid in all patients irrespective of diabetes mellitus,6922 while other studies reported that the relationship was valid only in non-diabetic patients.717 Our results suggest that the influence of BG level on prognosis among diabetic patients might be weaker than that in non-diabetic patients. Although the reasons for the relatively weak relationship between BG level and clinical outcomes in diabetic patients is unclear, there are several possible explanations. First, in diabetic patients, BG level is influenced by the degree of BG control before CICU admission, and basal BG level before the cardiac event may also be higher in diabetic patients than in non-diabetic patients, which influences the prognostic role of hyperglycemia during index hospitalization due to critical illness. Second, under critically ill conditions, glucose transporters are abnormally upregulated in non-diabetic patients; therefore, patients become highly susceptible to glucose toxicity.4 However, in diabetic patients, chronic hyperglycemia downregulates the glucose transporters in cells, and the cellular conditioning has been reported to protect cells from acute hyperglycemia-mediated damage423 and to contribute to the increase in threshold admission BG level which influences poor prognosis in relation to hyperglycemia. Likewise, since glucose metabolism is very complex in critically ill conditions in diabetic patients and the prognostic role of BG level is still controversial, further large-scale, well-designed studies should be performed to confirm these findings.
This study has several limitations. First, it is possible that patients who present with hyperglycemia may include those with undiagnosed diabetes mellitus. However, diagnostic evaluation for diabetes mellitus is generally performed if patients repetitively present an abnormal BG level during admission. Therefore, the proportion of undiagnosed diabetic patients included in the non-diabetic group is expected to be small. Second, we used a random BG level. Influence of diet or a stressful event was not considered when evaluating admission BG level. Third, patients who presented with hypoglycemia were included in group 1. Hypoglycemia has a negative influence on patient prognosis, which may have resulted in the finding of no significant difference in clinical outcomes between groups 1 and 2 within non-diabetic patients. Finally, we evaluated the relationship between admission BG level and mortality in the acute phase of critical illness, but not the effect of glucose control on patient mortality. From this study, we could not conclude whether glucose control may improve the prognosis for these patients.
In conclusion, admission BG level was associated with increased CICU mortality in critically ill, non-diabetic patients; however, the relationship lacked statistical significance even though CICU mortality numerically increased with baseline BG level in diabetic patients. Further large-scale studies are warranted to confirm these findings, particularly in diabetic patients.
 XML Download
XML Download