

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Hip fracture surgery is a common medical treatment in elderly patients. However, these patients often encounter abdominal problems that may require secondary surgeries or additional invasive procedures.1 Acute cholecystitis is one such representative abdominal problem. Cholecystitis, inflammation of the gallbladder, is sometimes accompanied by gallstones and is associated with symptoms of upper abdominal pain, fever, and leukocytosis.2 The risk factors of post-surgical cholecystitis generally include stasis of highly viscid bile induced by dehydration; hypovolemia; fever; obstruction at the sphincter of Oddi following starvation, narcotic use, and anesthesia; pigment load following blood transfusion; sympathetic stimulation; impaired circulation to the gallbladder; and septicemia with septic emboli reaching the gallbladder.34 These risk factors occur more frequently in elderly hip fracture patients than other fracture patients, who consequently exhibit a higher risk of acute cholecystitis.5 In a previous study, the incidence of acute cholecystitis occurring within 2 months after hip fracture surgery was reportedly 0.74% – much higher than expected – and the authors stated that these patients may have poorer prognosis.6 Furthermore, another study assessing acute abdominal complication that occurred after hip fracture surgery showed that two of 9,268 patients required cholecystectomy.1 The existing studies demonstrated lower incidences of acute cholecystitis and a smaller hip fracture patient group; therefore, the exact incidences could not be reported. Moreover, information from the patients' medical records were limited due to the retrospective nature of the studies.7 In addition, they did not analyze the effects of acute cholecystitis on the mortality of elderly hip fracture patients.
Here we utilized data from a nationwide claims database and attempted to assess the following questions: 1) what is the incidence of acute cholecystitis in elderly hip fracture patients (≥ 65 years of age); and 2) how does cholecystitis affect mortality rates after hip fracture?
METHODS
Study subjects
Study subjects were from the Korean National Health Insurance Service-Senior cohort (NHIS-Senior, NHIS-2018-2-036) compiled by the Korean NHIS. The data can be accessed via the Korean NHIS website (https://nhiss.nhis.or.kr/bd/ay/bdaya001iv.do). From a population of approximately 5.5 million Korean enrollees > 60 years of age in 2002, a total of 588,147 participants were randomly selected using 10% simple random sampling. This cohort statistically represents the population over age 60 in Korea. All individuals included in the NHIS-Senior were followed until 2015 unless death or disqualification for National Health Insurance, such as emigration, occurred. The NHIS, as a single payer under the single-insurer system of universal health coverage, maintains all personal information, demographics, and medical treatment data for Korean citizens, who were categorized as insured employees, insured self-employed individuals, or medical aid beneficiaries.89 The information in the dataset included all inpatient and outpatient medical claims data, including treatment procedure codes and primary and secondary diagnostic codes.89
Elderly hip fracture cohort
The eligibility criteria for elderly hip fracture patients were as follows: 1) first-time admission to an acute care hospital (index admission) with diagnostic codes of femoral neck fractures (International Classification of Diseases, 10th Revision [ICD-10] S720) or intertrochanteric fracture (ICD-10 S721)1011; 2) a hip fracture-free period of ≥ 4 years; 3) typical surgeries or procedures including open reduction of a fractured extremity (femur), closed pinning (femur), external fixation (pelvis or femur), closed reduction of fractured extremity (pelvis or femur), bone traction, skin traction, or hemiarthroplasty (hip)1011; and 4) age 65–99 years at the time of a hip fracture to identify fracture.11
Hip fracture patients with a prior diagnosis of gallbladder, biliary tract, or pancreatic cancer (ICD-10 C23, C24, or C25) were excluded to rule out the possibility of malignancy-induced cholecystitis. To ensure a minimal 180-day follow-up period, patients enrolled in the hip fracture cohort less than 180 days before the end of the observation period (June 31, 2015) were further excluded.
The incidence date (index date) of hip fracture was defined as the date of admission to the acute care hospital that fulfilled the eligibility criteria. The last date of follow-up was defined as the date of death or 31 December 2015, whichever came first.
Acute cholecystitis
Among the elderly hip fracture patients, the development of acute cholecystitis was defined as follows: 1) admission to an acute care hospital with diagnostic codes of acute or other cholecystitis regardless of calculus (ICD-10 K800–802, K804, K808, K810, K818–823, K828–829, K870)12; and 2) typical surgeries or procedures including cholecystectomy, cholecystostomy, cholecystotomy, cholecystoenterostomy, percutaneous cholecystostomy, or percutaneous transbiliary drainage. The incidence date of acute cholecystitis was defined as the date of admission to the acute care hospital for the treatment of acute cholecystitis. Patients who had acute pancreatitis (ICD-10 K85) between the date of hip fracture and the date of acute cholecystitis diagnosis were excluded.12
All-cause mortality
In the NHIS-Senior, each subject's unique de-identified number was linked to mortality information from the Korean National Statistical Office.8 Time from index date to date of death was used to define survival time. Considering acute and serious consequences of acute cholecystitis, 30-day cumulative mortality (mortality rate, %) was selected as the main outcome. In addition, 60-, 90-, and 180-day and 1-year mortality were used as secondary outcomes for evaluating the severity of acute cholecystitis.
Statistical analysis
For the descriptive and interim analysis, a Kaplan-Meyer curve was used to compare survival probability up to 365 days between hip fracture patients with and without acute cholecystitis. A generalized estimating equation model with Poisson distribution and logarithmic link function was performed to estimate adjusted risk ratios (aRRs) and 95% confidence intervals (CIs) to assess the association between acute cholecystitis and the risk of death. If the treatments for hip fracture and acute cholecystitis were provided at the same admission episode, the incidence date of acute cholecystitis was set to the same date (time 0) as that of hip fracture.
Potential confounders were adjusted using multivariate-adjusted regression models: age group, gender, household income level, residential area, Charlson Comorbidity Score (CCS), hip fracture type, surgery and anesthesia types, number of hospital beds, and calendar year of the hip fracture incidence. Each subject's number of comorbidities was assessed by diagnostic codes during the 3 years before the index date using the Quan's ICD-10 coding algorithm of the CCS. The presence of disease-constituting disease categories of the CCS was defined by at least two outpatient visits or one admission upon the primary or first secondary diagnosis.
The statistical analyses were conducted using SAS Enterprise Guide version 7.1 (SAS Institute, Cary, NC, USA). P values < 0.05 were considered statistically significant.
RESULTS
Between January 1, 2002 and December 31, 2015, a total of 19,950 hip fracture patients were admitted to hospitals and received specific treatment. The 3,465 patients who first developed a hip fracture before December 31, 2005 were excluded due to hip fracture free period. Additionally, 52 patients < 65 or > 99 years of age and 734 patients whose index date was within 180 days prior to December 31, 2015 were excluded, as were 89 patients with prior gallbladder, biliary tract, or pancreatic cancer or comorbid pancreatitis. Finally, 15,210 patients were enrolled in the cohort as hip fracture patients (Table 1).
Table 1
Baseline characteristics of study participants

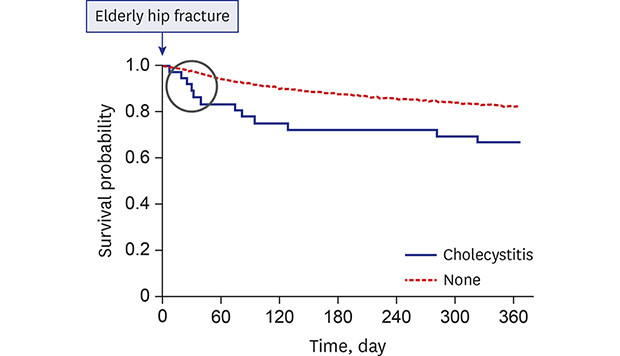
Among the study participants, 11,435 (75.2%) were women and 7,793 (51.2%) were 75–85 years of age. There were 7,888 cases (51.9%) of femoral neck fracture and 7,443 (48.9%) cases of hemiarthroplasty. Thirty-six patients developed acute cholecystitis within 30 days after the index date (30-day cumulative incidence, 0.24%). A descriptive comparison of survival probability up to 365 days is shown in Fig. 1. There is a large difference in initial mortality within 30 days.
Fig. 1
Kaplan-Meyer curve of hip fracture patients with and without acute cholecystitis. The P value of the log-rank test was 0.007.
Four of the 36 acute cholecystitis patients (11.1%) died within 30 days versus 2.92% of patients without acute cholecystitis (Tables 2 and 3). In the multivariate-adjusted Poisson regression model, hip fracture patients with incident acute cholecystitis were 4.35 (aRR, 4.35; 95% CI, 1.66–11.37; P = 0.003) times more likely to die within 30 days than those without acute cholecystitis. The risk of mortality decreased with time as follows: 60-day mortality aRR, 2.88 (95% CI, 1.32–6.26), 90-day mortality, aRR, 2.71 (95% CI, 1.42–5.18), 180-day mortality aRR, 2.15 (95% CI, 1.27–3.65), and 1-year mortality aRR, 1.78 (95% CI, 1.17–2.73).
Table 2
Effect of incident acute cholecystitis on 30-day mortality

Table 3
Effect of incident acute cholecystitis on cumulative mortality of different time frame
DISCUSSION
There have been several reports on the occurrence of acute cholecystitis in the field of orthopedic surgery. The previous report on nine cases of perioperative cholecystitis included four cases of post-hip fracture surgery, two cases of post-tibial fracture surgery, and one case each of post-infection, post-hip arthroplasty, and post-spine surgeries.13 Another study of 14 acute cholecystitis cases after orthopedic surgery included 12 cases of post-hip fracture surgery and 1 case each of post-hemipelvectomy and post-spine fusion surgery.14 These studies reported that acute cholecystitis occurs occasionally after orthopedic surgery and most prevalently after hip fracture surgery.6 However, the above studies are either outdated case reports or merely case series; therefore, very few studies have assessed the exact incidence or effect on mortality rate.15
Another large-scale study that utilized the medical records of 1,211 hip fracture patients from a single hospital reported that the incidence of acute cholecystitis after hip fracture was 0.74%, while other studies have reported the same incidences of 0.5% and 0.2%. However, these studies have limitations as retrospective studies.116 Furthermore, no previous studies assessed whether acute cholecystitis is a factor that increases the mortality rate of elderly hip fracture patients. The incidence of acute cholecystitis in elderly hip fracture patients from this study was 0.24%, and this is the value from a first incidence report to use a representative large dataset. In addition, this is the first study to assess the effect of acute cholecystitis on the mortality rate in elderly hip fracture patients.
Many previous studies have assessed the factors that increase the mortality rate of elderly hip fracture patients.17 More specifically, these included the patient-related factors such as myocardial infarction, congestive heart failure, current pneumonia, renal failure, and malignancy as well as environmental factors such as the long time period between hospital admission and surgery.18 One previous study reported that the patients with a medical history of myocardial infarction exhibited a 2.2-fold increased mortality rate within 30 days of hip fracture and that patients who developed a chest infection during their hospitalization period exhibited a 3.7-fold increased mortality rate.19 Another study demonstrated that hip fracture patients with cardiovascular disease events or pneumonia that occurred within 1 year exhibited a 3.6–3.8- or 3.4–4.7-fold increased mortality rate, respectively.20 Elderly hip fracture patients in this study who developed acute cholecystitis demonstrated increased 30-, 60-, and 90-day mortality rates by 4.35-, 2.88-, and 2.71-fold compared to patients who did not develop acute cholecystitis. The 30-day mortality rate after acute cholecystitis in elderly hip fracture patients is similar to that of cardiovascular disease and is much higher than that of chest infection patients. In the Kaplan-Meyer curve of this study, the survival probability of patients with acute cholecystitis was markedly decreased at the early stage.
There are a few possible explanations for how acute cholecystitis increases the mortality rates in elderly hip fracture patients. First, since acute cholecystitis is not easily distinguishable from other gastrointestinal symptoms and involves atypical clinical behaviors, it may not be diagnosed in the early stage. Consequently, this can lead to progression into the fulminant state.21 Narcotic analgesics used to control pain may relieve abdominal pain but can also contribute to the occurrence of cholecystitis.22 It was reported that 27% and 45% of elderly acute cholecystitis patients (≥ 70 years of age) do not exhibit right upper quadrant pain and fever, respectively.21 If acute cholecystitis is left undiagnosed, there is an increased chance of gallbladder perforation, which may be a serious threat for the patient.5 Second, the occurrence of acute cholecystitis in cases of elderly hip fracture may indicate a poor nutritional status. More than half of hip fracture patients exhibit poor nutritional status, consequently increasing the incidence of perioperative complications.23 The sign of malnutrition itself is reportedly a factor affecting 30-day mortality.24 Malnutrition induced by dehydration and starvation increases bile viscosity, encourages bile stasis, induces obstruction at the sphincter of Oddi, and consequently leads to the development of cholecystitis.22 Third, complications caused by the treatment of cholecystitis can increase the mortality rate of elderly hip fracture patients.1825 Fourth, the occurrence of acute cholecystitis in elderly hip fracture patients may indicate the development of complications during hip fracture treatment or a worsened general condition. Several factors lead to the onset of acute cholecystitis.22 Profuse bleeding or hypotension without adequate intravenous fluid treatment during hip fracture surgery may cause gallbladder circulation problems, while blood transfusion may cause acute cholecystitis due to an increased pigment load.3
There are several limitations of this study. First, the exact incidence date of acute cholecystitis could not be identified if treatments for acute cholecystitis were performed during the same admission episode of hip fracture. This could introduce an immortal time bias due to the additional survival time of incident acute cholecystitis patients.26 However, although the immortal time bias could induce a protective effect of acute cholecystitis on mortality, the results of this study showed an increased risk of mortality. This phenomenon might represent an underestimation of effect size. Second, administrative claims data have intrinsic limitations. Diagnostic codes listed for the cohort may not represent a participant's true disease status, an inherent limitation of insurance databases. However, the incidence of hip fracture and acute cholecystitis in this study could be measured fairly well because nearly all types of healthcare providers follow the fee-for-service system and all treatment procedures such as surgeries are claimed by hospitals. Third, due to the rare incidence of acute cholecystitis following elderly hip fracture treatment, the two groups have distinct sample inequality (36 vs. 15,174). However, large senior cohort data were used to confirm the incidence of acute cholecystitis after elderly hip fracture. In addition, we adjusted the potency confounders such as age, anesthesia type using multivariate-adjusted regression models to find that acute cholecystitis is an independent risk factor for elderly hip fracture mortality.
In conclusion, incidence of acute cholecystitis in elderly patients after hip fracture within 30 days after the index date was 0.24%. Acute cholecystitis in elderly hip fracture patients dramatically increases the 30-day mortality rate by 4.35-fold. Therefore, early disease detection and management are crucial for patients.
 XML Download
XML Download