

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The rapid decline in the incidence of diphtheria and tetanus after the widespread use of the diphtheria-tetanus-pertussis combination vaccine (diphtheria-tetanus-whole cell pertussis [DTwP] or diphtheria-tetanus-acellular pertussis [DTaP]) since the mid-1940s is a classic example of major diseases where the efficacy of the vaccines was proven. Tetanus, however, is still a major problem as a form of neonatal tetanus in low-socioeconomic-status countries, and is still a threatening infection in unvaccinated people. Diphtheria is a droplet-mediated infectious disease and still occurs in Korea's neighboring countries. It should also be noted that diphtheria pandemics occurred in the former Soviet Union, with a decline in DTP vaccination following its collapse in the 1990s.12345
After the introduction of DTwP in 1958, the rate of DTaP vaccination exceeded 90% in the 1980s, and there has been no reported case either of infant tetanus or of diphtheria since 1987 in Korea. Nevertheless, as the disease still exists, the protective immunity against tetanus should be maintained after childhood. In addition, several seroepidemiologic studies revealed that elderly subjects are especially vulnerable to diphtheria and tetanus in Korea.36789
The tetanus diphtheria (Td) vaccine is recommended as an essential vaccine for adolescents and adults due to its personal and public benefits. The efficacy and effectiveness of diphtheria and tetanus toxoids have been reported to be 70%–90% according to the number of vaccinations. Adolescents or adults who completed the primary vaccination series can be effectively protected by a booster dose of the Td vaccine every 10 years.12
In Korea, several clinical trials assessed the immunogenicity and safety of the Td vaccine in adolescents and adults, and proved its clinical efficacy and safety.101112
GC1107 is a newly developed Td vaccine by GC Pharma, Korea. In this phase 3 clinical study, the immunogenicity and safety of GC1107 were evaluated and were compared to those of a commercial Td vaccine (Td-pur; GlaxoSmithKline, London, UK) in adults aged 18 years or above.
METHODS
Study subjects and design
A total of 376 healthy men and women subjects were included in this clinical study for evaluating the immunogenicity and safety of GC1107. The study duration was 5.5 months, from May 12 to October 30, 2014. In the first stage, assessment of the immunogenicity and safety of GC1107 was conducted in a double-blind, randomized, multi-center, active-controlled clinical study. In the second stage, additional safety evaluation was conducted in an open-label, multi-center study. The subjects were selected among individuals without any vaccination with Td or adult tetanus-diphtheria-pertussis (TdaP) vaccines within 5 years before the screening. Excluded were those who were allergic to ingredients like aluminum hydroxide in the vaccine that was used for the study, those whose antitoxin potency against diphtheria and tetanus was 1.0 IU/mL or higher, and those with a history of significant adverse events (AEs) following vaccination against diphtheria, tetanus, or both. Detail eligibility was described in Supplementary Table 1.
In the first stage, the subjects were interviewed and examined to identify the vaccination history and antibody levels against diphtheria and tetanus, and blood samples were collected. The final screening test was conducted in the second visit, and the qualified subjects were randomized to GC1107 or the control group. The study or control vaccine was administered to the subjects in each group, on the deltoid muscle. After vaccination, the subjects were monitored for 30 minutes for the occurrence of any immediate AE. The final visit was made on the fourth week after vaccination, wherein blood samples were collected for immunogenicity assessment. To evaluate the safety of the vaccine, each subject's diary, in which any AE that occurred after the vaccination was recorded, was submitted. After the completion of randomization in stage 1, additional subjects were assigned to the GC1107 (stage 2) group to assess the safety of GC1107 with more adult subjects. The rest of the study procedure was similar to that of stage 1.
Vaccine administration
A 0.5 mL dose of GC1107 (Batch No. T401003; GC Pharma, Yongin, Korea) included ≥ 2 IU diphtheria toxoid, ≥ 20 IU tetanus toxoid, and 0.55 mg aluminum hydroxide gel. The control vaccine was Td-pur inj (Batch No. 064101A; GlaxoSmithKline) 0.5 mL per dose, which was composed of ≥ 2 IU diphtheria toxoid, ≥ 20 IU tetanus toxoid, and 1.5 mg aluminum hydroxide. For the stage 1 immunogenicity and safety evaluation, a single dose of either GC1107 0.5 mL or Td-pur inj 0.5 mL was injected on the deltoid muscle. In stage 2, for additional safety evaluation, additional subjects were given a single injection of GC1107 0.5 mL on the deltoid muscle.
Evaluation of immunogenicity
The initial immunogenicity was evaluated by comparing the protective antibody ratios against diphtheria and tetanus of the GC1107 and control groups on day 28 after vaccination. Approximately 5 mL each blood samples were taken for diphtheria and tetanus antibody tests in visits 1 and 4. The serum was stored at −18°C until analysis, and neutralization antibody tests for diphtheria and tetanus were conducted at the Vaccine Bio Research Institute of the Catholic University of Korea. The antibody test for the diphtheria toxin was conducted using the specific anti-diphtheria toxin immunoglobulin G (IgG) antibody enzyme-linked immunosorbent assay (ELISA) kit (Cat. No. RE56191; IBL, Hamburg, Germany), and the antibody test against tetanus was conducted using the specific anti-tetanus toxin IgG antibody ELISA kit (Cat. No. RE56901; IBL). After diluting the serum samples to a 1:100 ratio and letting them stand for 60 minutes at room temperature, the samples were washed three times, centrifuged for 30 minutes, and then washed again. After 20-minute incubation for color development, the samples were measured spectrophotometrically at 450 nm. The standard curve was prepared at the same time, and was used to determine the antibody titer of each sample. Besides the booster response, the secondary immunogenicity was evaluated by the geometric mean titers (GMTs) of the anti-toxin antibody titers against diphtheria and tetanus, respectively. Regardless of the pre-vaccination antibody titers, the protective antibody response was defined as a post-vaccination antibody titer of 0.1 IU/mL or above, as determined via ELISA. The booster response was considered positive when the less than 0.1 IU/mL pre-vaccination antibody titer increased to ≥ 0.4 IU/mL after vaccination, or when the 0.1 IU/mL or higher pre-vaccination titer showed a fourfold or higher increase after vaccination.
Safety evaluation
The subjects enrolled in this trial were asked to submit their respective diaries, in which they recorded the AEs that occurred to them after vaccination. For safety evaluation, severity evaluation was conducted for the solicited AEs (pain, pressure, irritation, swelling, fever, vomiting, nausea, diarrhea, headache, fatigue, and myalgia) that manifested within 7 days after vaccination and for the unsolicited AEs that manifested within 28 days after vaccination.
In addition, the changes in the subjects' vital signs (systolic pressure, diastolic pressure, pulse, respiration, and axillary temperature) before and 28 days after vaccination, and the normal/abnormal change rates of the physical examination were evaluated based on the frequency and percentage.
Statistical analysis
The collected data were analyzed in the safety, full-analysis (FA), and per-protocol (PP) groups. The safety group included all the subjects who received the GC1107 or control vaccine at least once. The subjects who were assigned to the study groups but were excluded before vaccination were excluded from the safety analysis. The FA group included all the subjects who completed the vaccination and for whom immunogenicity data were available at least once. The PP group included all the subjects who completed the current study in accordance with the protocol for analysis. For immunogenicity analysis, the PP group was used as the primary analysis set, and the FA group was used as an additional analysis set. The safety assessment was conducted using the safety group. The missing values were not substituted, and all the statistical verifications were based on the 5% or lower significance level, through a two-sided test.
For primary assessment, the upper limits of the 97.5% confidence intervals (CIs) for the difference of protective antibody ratio between two groups were calculated. As secondary endpoint, the GMT/GMR of antibody titers and booster response rate were calculated with 95% CI. For adjusting age group, Cochran-Mantel-Haenzel test was used to compare seroprotection rate between groups. The difference in GMT between groups was analyzed using Ancova with age as a covariate. For continuous variable, Independent two sample t-test or Wilcoxon rank-sum test was used to compare the mean between two groups. For categorical data, χ2 test or Fisher's exact test was used to compare the percentage between groups.
Ethics statement
For this clinical study, the study protocol, the study introduction form, and the informed consent form for the subjects were approved by the Ministry of Food and Drug Safety. In addition, all the clinical study aspects, including the study protocol, were approved by the Institutional Review Boards (IRBs) of the study centers. The study centers that were approved for this study included Incheon St. Mary's Hospital, The Catholic University of Korea (IRB No. OC14BDMT0025), Daejeon St. Mary's Hospital The Catholic University of Korea (IRB No. DC14BDM0017), Bucheon St. Mary's Hospital The Catholic University of Korea (IRB No. HC14BDMT0045), St. Vincent Hospital The Catholic University of Korea (IRB No. VC14BDMT0052), St. Mary's Hospital The Catholic University of Korea (IRB No. SC14BDMT0041), Kyung Hee University Hospital (IRB No. 1410–01), Soonchunhyang University Seoul Hospital (IRB No. SCHUH2014-03-012-001), and Hallym University Kangnam Sacred Heart Hospital (IRB No. 2014-03-30 [601]). All the subjects who participated in the study submitted their signed informed consent form.
RESULTS
Study subjects
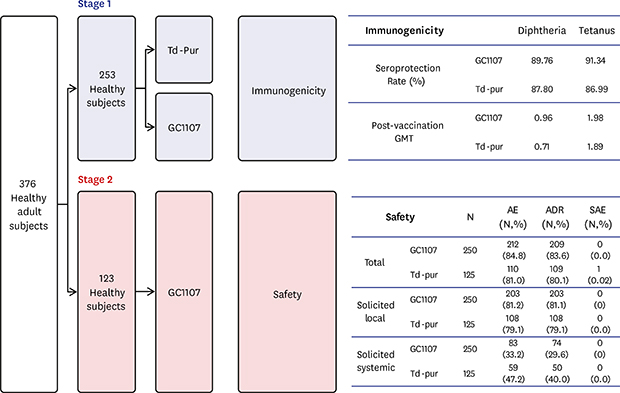
For this study, a total of 415 subjects were screened, and 127 subjects were assigned to the GC1107 group while 125 subjects were assigned to the control group in the first stage. In the second stage, 123 subjects were included in the GC1107 group in an open-labeled, single-arm study. Only one subject dropped out during the study. As a result, a total of 375 subjects completed the study (Fig. 1).

Of the study subjects, 93 were men (24.8%) and 282 were women (75.2%). In the GC1107 group, there were 71 men (28.4%) and 179 women (71.6%), and in the control group, 22 men (17.6%) and 103 women (82.4%). As a result, the difference in the ratio of men and women subjects between the two groups was statistically significant (P = 0.022). As for the age distribution in the GC1107 group, 141 subjects (56.4%) were 18–40 years old, 87 (34.8%) were 41–60 years old, and 22 (8.8%) were older than 60 years old. In the control group, 62 subjects (49.6%) were 18–40 years old, 42 (33.6%) were 41–60 years old, and 21 (16.8%) were older than 60 years old. There was no statistically significant difference between the two groups in terms of age. The difference in medical history and concomitant medication of GC1107 group and control group was not statistically significant (Supplementary Table 2).
Immunogenicity
The primary endpoint (protective antibody ratios after vaccination) in the GC1107 group was 89.76 and 91.34% for diphtheria and tetanus, respectively. In the control group, the ratios were 87.80 and 86.99%, respectively. The non-inferiority was confirmed when the GC1107 group was compared to the control group, as the peak of the one-sided credibility interval (97.5%) on the differences in the protective antibody ratios between the two groups was less than 10%, which was the limit of the clinical non-inferiority (diphtheria, 5.87; tetanus, 3.35) (Table 1).
Table 1
Immunogenicity evaluation of the diphtheria and tetanus protective antibody rates

As for the secondary endpoint for immunogenicity, which is the GMT of the anti-toxin antibodies, the GC1107 group showed an increase in the GMT of the anti-diphtheria antibodies from 0.07 before vaccination to 0.96 after vaccination, and the control group showed an increase from 0.07 to 0.71. As for the GMT of the anti-tetanus antibodies, the GC1107 group showed an increase from 0.05 before vaccination to 1.98 after vaccination, and the control group showed an increase from 0.05 to 1.89. The GMT differences before and after vaccination for the diphtheria and tetanus antibodies were not statistically significant between the two vaccines. The geometric mean ratio (GMR) of the diphtheria antibody titers before and after vaccination was 12.88 for the GC1107 group and 10.63 for the control group. The GMR of the tetanus antibody titers before and after vaccination was 39.53 for the GC1107 group and 34.55 for the control group, respectively. The GMR differences between the groups of the diphtheria and tetanus antibodies were not statistically significant (P values for GMR differences were 0.200 and 0.478 for diphtheria and tetanus, respectively) (Table 2).
Table 2
Immunogenicity evaluation of diphtheria and tetanus anti-toxin antibody potency's geometric average

The diphtheria booster responses for the GC1107 and control groups were 70.87% (90/127) and 64.23% (79/123), respectively, while the tetanus booster responses for the GC1107 and control groups were 78.74% (100/127) and 78.86% (97/123) and there was no statistical difference (P values were 0.262 and 0.981 for diphtheria and tetanus, respectively) (Table 3).
Table 3
Immunogenicity evaluation of the diphtheria and tetanus booster response

The protective antibody ratios of diphtheria and tetanus for each age group showed no statistically significant difference (Supplementary Table 3). For the GMR of the diphtheria antibody titers among the subjects older than 60 years old, the GC1107 group showed statistically and significantly higher GMR compared to the control group. When the age groups were corrected, the comparison of the GMTs of diphtheria and tetanus did not show any statistically significant difference (Supplementary Table 4).
Safety
In this study, the AEs in terms of safety, vital signs, and physical examinations were monitored. After vaccination, the incidence rates of AEs, regardless of the causal relationship with the vaccination, were 84.8% (572 cases) for the GC1107 group and 88.0% (337 cases) for the control group. Among these, the incidence rate of adverse drug reactions (ADRs) of the GC1107 group was 83.6% (502 cases), and that of the control group was 87.2% (297). Serious AEs did not occur in the GC1107 group, but there was 1 case (gastroenteritis, 0.8%) of serious AE in the control group, which, however, was not an ADR. None of the subjects dropped out from the study because of AEs (Table 4). Detail solicited local, solicited system and other AEs were shown in Supplementary Table 5. Most common local AE was tenderness (78.0% and 78.4% for GC1107 and Td-pur, respectively), then pain and swelling of injected site. Most common systemic AE was myalgia (22.0% and 33.6% for GC1107 and Td-pur, respectively).
Table 4
Adverse event summary

The analysis of the incidence rate of AEs based on gender, age, past history, current history, operation history, previous medications, and concomitant medications showed that the incidence rates of AEs in the two groups were not significantly different from each other. All the subjects were examined for their vital signs (systolic pressure, diastolic pressure, pulse, respiration, and axillary temperature) at each visit, and no significant changes were found during the study. The safety evaluation revealed no significant differences between the GC1107 and control groups.
DISCUSSION
In this study, a newly developed Td vaccine, GC1107, showed a non-inferior immunogenicity profile and a similar safety profile compared to the control vaccine (Td-pur).
In Korea, the Td vaccine was introduced in 2003 and has been recommended for adolescents and adults. There are currently three Td vaccines that have been approved in Korea: the SK Td vaccine (SK Chemicals, Seongnam, Korea), Td-pur (GlaxoSmithKline), and diTebooster SSI (Accesspharma, Seoul, Korea). As the TdaP vaccine contains similar amounts of tetanus and diphtheria toxoids as the Td vaccine, as well as pertussis antigens, the TdaP and Td vaccines are known to provide similar protection against tetanus and diphtheria. There are two types of TdaP vaccine available in Korea: Adacel (Sanofi Pasteur, Lion, France) and Boostrix (GlaxoSmithKline).
Although there was no controlled clinical trial on the efficacy of the diphtheria and tetanus toxoids, many observational studies have supported the effectiveness of both toxoids.12 In the aspect of immunogenicity, a level of antibodies greater than 0.01 IU/mL is regarded as the minimal protective level in both diphtheria and tetanus. In most cases, three doses of diphtheria toxoids in adults resulted in the achievement of anti-diphtheria toxoid titers greater than 0.1 IU/mL. The tetanus antibody titers are also regarded as protective if they are greater than 0.1 IU/mL, but this is based on in-vivo neutralization tests and animal studies.12
Three immunogenicity studies on the Td vaccines were reported in Korea between 2008 and 2010.101112 With Korean children aged 11–12 years old with 4–5 times vaccination of DTaP before 6 years old, the proportions of subjects with pre-vaccination antibody titers of < 0.1 IU/mL against diphtheria and tetanus were 22.4 and 20.2%, respectively. After vaccination, all the subjects (100%) showed protective antibody titers of ≥ 0.1 IU/mL. The proportions of subjects with high protective antibody titers of ≥ 1.0 IU/mL against diphtheria and tetanus were 8.7% and 21.3% before vaccination and 95.1 and 98.9% after vaccination, respectively.10
A similar result was reported in pre-adolescent and adolescent Korean subjects aged 11–18 years old with 4–5 times vaccination of DTaP before 6 years old; all the subjects showed protective antibody titers of ≥ 0.1 IU/mL, and the proportions of subjects with high titers of > 1.0 IU/mL against diphtheria and tetanus also increased from 17.6% and 13.7% pre-vaccination to 91.3% and 99.3% post-vaccination, respectively, after a single-dose vaccination.11
In one study with non-vaccinated adults aged ≥ 40 years, 33.9% and 96.7% of the study participants showed less than 0.1 U/mL antibody titers against diphtheria and tetanus before vaccination, respectively. After the administration of one dose of the Td vaccine, 92.6% and 77.6% of the study participants showed antibody levels of more than 0.1 U/mL for diphtheria and tetanus, respectively. After the administration of three doses of the Td vaccine, 99.6% and 100% of the study participants showed antibody levels of more than 0.1 U/mL for diphtheria and tetanus, respectively. After the administration of three doses of the Td vaccine, 83.1% and 93.8% of the subjects achieved antibody levels of ≥ 1.0 IU/mL against diphtheria and tetanus, respectively.12
In the present study, the immunogenicity results of GC1107 were similar to those of other studies in children, pre-adolescents, and unimmunized adults in Korea. After GC1107 vaccination, 50.4% and 66.1% of the subjects achieved antibody levels of ≥ 1.0 IU/mL against diphtheria and tetanus, respectively. The control vaccine resulted in 45.6% and 66.4% of the subjects achieving antibody levels of ≥ 1.0 IU/mL against diphtheria and tetanus, respectively (data not shown).
A total of 84.8% of the subjects in the GC1107 group and 88.0% of the subjects in the control group experienced AEs after vaccination, and there was no significant difference between the groups. The incidence rates of AEs were similar to those of the previous studies with children and adolescents.1011 They were much higher, however, than those in adults.12 This discrepancy might have been due to the active reporting of AEs by the parents in the study with children and adolescents. Consistent with this, in the present study, the AEs were more strictly monitored and recorded by a clinical research associate (CRA) and a contract research organization (CRO), and a higher rate of AEs was shown compared with the previous study. As in the other studies, however, there were no severe and significant AEs in the GC1107 group, which confirmed that the new Td vaccine is safe.
It is a well-known recommendation that protective immunity against diphtheria and tetanus be obtained from proper primary series immunization, and be maintained by a booster dose every 10 years.12 In Korea, a DTwP vaccine was introduced in 1958. Therefore, those who were born before 1958 had never been vaccinated with either the DTwP or DTaP vaccine introduced in 1982.121314
The latest report on the seroprevalence of tetanus in Korea revealed that the population with anti-tetanus IgG antibody titers higher than 0.1 IU/mL was 92.0% in the 11- to 20-year-old subjects, 95.7% in the 21- to 30-year-old subjects, 72.3% in the 31- to 40-year-old subjects, 33.3% in the 41- to 50-year-old subjects, 17.3% in the 51- to 60-year-old subjects, and 19.3% in the subjects ≥ 61 years old. An increasing tendency of seroprevalence was observed in the younger age groups with seropositivity compared with the studies done in 2000 and 2008.389
The latest report on the seroprevalence of diphtheria in Korea revealed that the population with anti-diphtheria IgG antibody titers higher than 0.1 IU/mL was 89.5% in the subjects < 11 years old, 78.0% in the 11- to 20-year-old subjects, 59% in the 21- to 30-year-old subjects, 49% in the 31- to 40-year-old subjects, 39% in the 41- to 50-year-old subjects, 67% in the 51- to 60-year-old subjects, and 71% in the subjects ≥ 61 years old.3 As mentioned, no case of diphtheria have been reported in Korea since 1987.
There are quite a number of elderly people with low serum levels of tetanus in Korea, and the mean age of the onset of tetanus infection was 63.3 years in the 17 cases reported in the early 2000s in Korea.15 As mentioned, the tetanus seroprevalance of adults older than 41 years is lower than 40%, and therefore, decennial Td vaccination should be encouraged in Korea.1213
According to a report of Korea Center for Disease Control and Prevention (KCDC) in 2013, the vaccination rate of DTaP in Korea was 99.9% in children less than 3 years old, and the Td vaccination rate was 9.4% in the 19- to 49-year-old subjects, 3.4% in the 50- to 64-year-old subjects, and 3.1% in the 65-year-old subjects. The report implies that people > 19 years old are rarely vaccinated with Td for the maintenance of the protective antibody titer, and most of the vaccinated cases were vaccinated in the hospital that the subject visited for other reasons, such as trauma. The Td and TdaP vaccines' coverage in the adult population (≥ 18 years) were 57.5 and 28.9% in the United States and 61%–74% in 2010/2011 in Europe.141617 The clinical implication of the Td vaccine is limited in routine vaccination practice because several combination vaccines (diphtheria/tetanus/acellular pertussis/inactivated polio vaccine [DTaP-IPV], diphtheria/tetanus/acellular pertussis/inactivated polio vaccine/Haemophilus influenzae type b [DTaP-IPV-Hib], ditheria/tetanus/acellular pertussis/hepatitis B/inactivated polio vaccine [DTaP-HebB-IPV]) for children are now available. Td is licensed for use over 7 years old, and TdaP is preferentially used for additional prevention effect against pertussis. The Td vaccine, however, is one of the essential vaccines for adults. Therefore, decennial vaccination with the Td vaccine in adults should be further encouraged in the field with the support of governmental policy.
An immunogenicity study on a new Td vaccine (GC1107) was conducted in Korean adults, and it was concluded that GC1107 showed non-inferior immunogenicity and safety compared to the control Td vaccine currently used in Korea.
 XML Download
XML Download