

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Within the field of medical education, competency-based medical education (CBME) is an emerging approach that has been adopted in many countries.1 Twelve Accreditation Council for Graduate Medical Education (ACGME) specialties in the United States have already developed competency-based achievement guidelines for their residents.2 Graduate medical education traditionally follows a specific time-based curriculum that includes required experience during training. However, the healthcare environment is rapidly changing such that traditional training programs cannot meet current societal needs.
Resident physicians have the right to be properly trained in a safe environment, but they are commonly regarded as cheap labour and are prone to exploitation, sometimes working over 100 hours per week.3 In 2016, Korea launched a special act to restrict residents' work hours to improve the poor working conditions of trainees as well as patient safety. Then in 2017, the duration of internal medicine residency in Korea was changed from 4 years to 3 years. Thus, there is now an urgent need to develop methods to ensure trainees' competence despite these losses of teaching and clinical time. Pressure to maintain efficiency of care, changes to patient safety requirements, and the recent restrictions of resident duty hours have driven the transition to CBME.456
In the present study, we describe the process of developing and implementing CBME in the internal medicine residency program at a tertiary university-affiliated hospital. We further report the results of a survey of the residents' satisfaction following CBME implementation.
METHODS
In 2015, the Residency Curriculum task force team of the Seoul National University Bundang Hospital Department of Internal Medicine (SNUBH IM) was convened to develop a competency-based internal medicine residency curriculum. The task force team includes eleven faculty members representing multiple medical specialties, including gastroenterology, nephrology, and medical education.
Design of the residency training program
The task force team again applied the consensus workshop method to determine the principles that would guide the training program design, ultimately selecting on five main areas of focus. It was decided that the training program should be 1) resident-centred, 2) systematic rather than opportunistic, and 3) focused on general internal medicine rather than specialty training; and that it should 4) include experience in various care setting (e.g., inpatient, ambulatory care, emergency room, intensive care unit, and consult services), and 5) work-based assessment and feedback.
Development of the competency-based curriculum
The competency-based curriculum was developed and implemented in multiple steps, as follows78: 1) analysis of current situation, 2) identification of objectives, 3) identification of competencies, 4) determination of competency components and performance levels, 5) mapping of objectives and competencies to learning experiences, 6) adjustment of individual residents' training programs, 7) development of an assessment system, and 8) overall evaluation of the training program.
Step 1: analysis of current situation
We started by analysing the current situation regarding the environment within and surrounding SNUBH IM. There were a total 36 residents at SNUBH IM, including 9 residents in each training year. The recent opening of a cancer centre at SNUBH meant more beds at the hospital, such that a limited number of resident physicians were caring for an increasing number of patients. Residents complained of work overload and dissatisfaction with their training program. Outside of the hospital, the healthcare system environment was rapidly changing, including the scheduled legislation restricting residents' working hours. Specifically, the special act for resident workplace improvement included a restriction to 80 work hours per week, prohibition of continuous duty for over 36 hours, a guarantee of at least one day off-duty, and other changes.
Step 2-4: identification of objectives, identification of competencies and determination of competency components and performance levels
To develop our objectives, we referred to the literature, including the RESPECT 100 research project, performed by the Research Development Committee of Korean Medical Education and Evaluation. This project describes a comprehensive curriculum that embodies the fundamentals of resident education, which originated from the need to develop generic competencies for training and evaluating high-quality professionals. RESPECT is an acronym for the six competencies included in the curriculum: respect, ethics, patient safety, professionalism, excellence, and teamwork.9 We also reviewed the Doctor's Role 5th research project (2014) sponsored by the Ministry of Health & Welfare, which suggests the following five competencies: patient care, communication & collaboration, social accountability, professionalism, and education & research.10 Finally, we considered the ACGME six competencies of graduate medical education: medical knowledge, patient care, professionalism, interpersonal and communication skills, practice-based learning and improvement, and systems-based practice.11
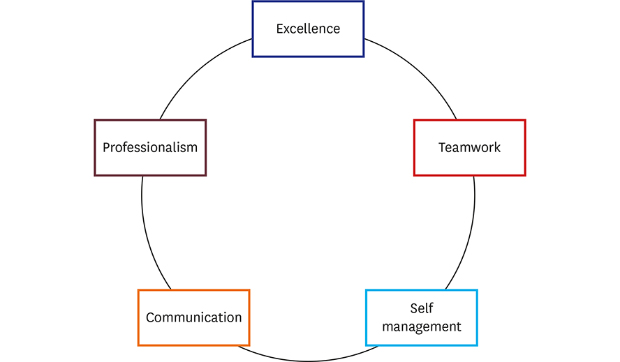
Using the consensus-building workshop method, we determined that the most desirable outcome competencies for an internal medicine doctor were excellence, professionalism, communication, teamwork, and self-management. We further assigned detailed sub-competencies to each component. Next, we set desired performance level targets for the ends of training periods, and mapped them to learning experiences. This framework was used to adjust the training program and to developing an assessment system.
Step 5-6: mapping of objectives and competencies to learning experiences and adjustment of individual residents' training programs
We further endeavoured to map objectives and competencies with defined proficiency levels to learning experiences, with the aims of integrating the desired competencies into the curricula and of implementing evaluation systems for performance in each area. Residents acquire clinical experience in a variety of patient care settings, including the intensive care unit, emergency room, inpatient services, ambulatory care, and consult services. We structured each resident's rotation to ensure that they had the clinical experiences necessary to reach the required competencies. Notably, residents represent an important component of the manpower of hospital's healthcare team, and thus their placement was also influenced by the needs of the hospital.
With regards to educational methodologies, we deliberated adopted teaching methods incorporating workplace-based learning with interactive lectures, discussions, and tutor-facilitated small-group debriefings. We further planned that trainees would actively participate in education and research activities to foster academic minds within the field of internal medicine.
Step 7: development of an assessment system
Residents were assessed using workplace-based assessments, such as the mini-CEX, oral examination, record review, global rating, checklist and case-based discussion (Supplementary Data 1, 2, 3, Supplementary Table 1). We assessed trainee's competency using assessing tools (e.g., 10-Likert scale) every month through training period. Successful CBME implementation requires a reliable and practical evaluation system that promotes learning. Workplace-based assessment must be widely administered, and preceptors should provide constructive behaviourally based feedback, as well as assess and illustratively document the residents' performances. CBME requires a more time-consuming assessment process compared to that provided in most traditional training programs, and the assessors must use a standardized method to provide reliable and valuable assessments. Therefore, faculty recruitment and development were urgent and inevitable issues in this transition.
Step 8: overall evaluation of the training program
Through monthly assessment of resident's competency, we had followed each resident's improvement and analysed individual resident's learning needs. Each resident has a mentor with whom resident can get the counselling through regular meeting.
At 18 months after implementing the new resident training program, we surveyed the residents with regards to overall satisfaction and opinions on the training program. We surveyed residents' overall satisfaction using 5-point Likert scale, where 5 = extremely satisfied, 4 = very satisfied, 3 = satisfied, 2 = somewhat satisfied, and 1 = not satisfied. We also asked the residents to describe the merits and demerits of their current training program and whether they had ever considered stopping their resident training. If they answered “yes,” they were asked to provide a detailed description of the reasons that they considered stopping training.
RESULTS
Participants' demographic characteristics
A total of 21 (100%) internal medicine residents completed the questionnaire. The average age, the proportion of women, and marital status were described in Table 1.

Residents' performance
With more often direct observation and documented feedback on competency standards, we could assess residents' performance more accurately and could find earlier both residents in difficulty and those with excellent performance. Through multiple observations and meetings, mentors could guide their mentee to individualized program; for example, residents in difficulty have counselling sessions for improving their performance and those with excellent performance could participate in research project.
Residents' overall satisfaction score and feedback on training program
The overall satisfaction score was 3.24 and the total satisfaction score did not significantly differ according to gender or marital status (Table 2).
Table 2
Comparison of internal medicine residents' total satisfaction scores on training program
Commonly noted merits of the CBME training program included the preceptor's practical training in an educational atmosphere and improvement through training (n = 13), and the clinical autonomy (n = 7). As for the demerits of the training program, residents answered that their heavy workload was the biggest problem (n = 7). Some residents stated that they needed a more organized welfare and support system.
Noted merits and demerits showed that residents were satisfied with the training program but they complained about the working condition, which was not direct part of the training program. As residents' training is linked with the working condition such as duty hours or patient care workload, it is hard to think separately of working condition and training program.
DISCUSSION
In this report, we describe our experience of redesigning an internal medicine residency training program to follow a CMBE model. We also report the results of a survey of job satisfaction among residents following implementation of the new training program. Our findings suggest that the transition to CBME had a positive influence on the educational environment for residents.
CBME is a predominant feature of graduate medical education reform worldwide. Theoretically, the transition to CBME implies a transition from the traditional time- and process-based framework to a competency-based model having a defined outcome, in which physicians-in-training achieve a well-defined set of competencies, including the knowledge, skills, attitudes, and behaviours required for safe and effective practice. Our CBME training program might not be a perfect program such as ACGME milestone project or EPA. But, we had established our own outcome competencies and we assessed trainee's competency using assessing tools every month through training period.
We are just one small institution and did not have sufficient time to develop a fully satisfactory new training program. And recruiting faculty members for resident education and evaluation was not easy because most of them are under the pressure of clinical overload and research requirements. Despite these difficulties, our task force reached agreements regarding the ideal outcomes of internal medicine residency, the desirable competencies of internal medicine doctors, and how to modify our residency training program.
In this study, we also surveyed whether residents had ever considered ending their training. Among the 21 residents, 11 residents answered that they had considered stopping their resident training. The most common reason for considering withdrawing from training was work overload (n = 7) and loss of patient rapport (n = 1).
In teaching hospitals, institutional service needs are often prioritized over educational needs, such that resident physicians are tasked with chores in the hospital. Thus, redesigning the training program and educational environment alone cannot solve all of the current problems, such as work overload, without hiring a substitute workforce to lessen the burden on residents. It is important to consider training program and working condition together, rather than in isolation from one another. Moreover, the ACGME already recommends that the implementation of advanced training systems requires evaluation and management of residents' attitudes and mental health. We should pay attention to residents' job satisfaction and well-being. A physician's well-being can be influenced by patient service size,12 work hours,13 and rotation length14; therefore, we suggest that resident scheduling should be organized with consideration of the physician's well-being in addition to the hospital needs and ensuring competencies.
Our study has several limitations. First, this study was performed at a single institution and only included 21 internal medicine residents. Therefore, our results may not be generalizable to other institutions, which might have different circumstances. Second, residents' satisfaction on training program could be influenced by various factors such as working environment, work load, and salary, not only by training program.
Overall, our present results indicate that residents showed their general satisfaction with the educational environment of the hospital with implementation of CBME in residency training. Greater efforts to improve the educational program and environment are warranted. Because required competencies should be revised with the change of societal needs, implementing and maintaining CBME should be ongoing process.
 XML Download
XML Download