

 PDF
PDF Citation
Citation Print
Print




INTRODUCTION
The out-of-hospital cardiac arrest (OHCA) is a global health problem with prevalence ranging from 50 to 90 cases per 100,000 person-years worldwide.1 Although the major advance has been achieved in the emergency medical service system and cardiac arrest resuscitation techniques, the overall survival rate in patients with OHCA is still low, especially in Asians.123 Among various etiologies of OHCA, coronary artery disease (CAD) has been reported as the most common cause of OHCA, and over 50% of OHCA patients without definite evidence for non-cardiac causes had significant CAD.456789 Numerous studies have attempted to assess the clinical benefit of invasive coronary angiography (ICA) with coronary revascularization after resuscitation; however, their results were inconsistent.2567101112 Although the current guideline recommended ICA for those with ST-segment elevation on the post-resuscitation electrocardiogram (ECG),13 the decision on ICA based on ST-segment changes in post-resuscitation ECG has limitations because of a low diagnostic yield of ECG.141516 In addition, clinical presentation is similar between patients with arrest due to hemorrhagic stroke and those with cardiac arrest. In such cases, physicians sometimes performed unnecessary ICA and antithrombotic treatment, which could delay accurate diagnosis and lead to deleterious outcome.1718 Moreover, due to its invasiveness, patients would be exposed to additional complication risk following ICA such as vascular injury, hemorrhage, myocardial ischemia, infection or event death.19 On the contrary, delaying ICA can be fatal in OHCA patients who have a significant stenosis or occlusion of the coronary artery by prohibiting maximal benefit from life-saving coronary revascularization. Therefore, it is very important to identify clinical factors guiding physicians to perform appropriate ICA on OHCA patients. The aim of the current study was to investigate clinical factors related to obstructive CAD among OHCA patients at initial presentation.
METHODS
Study subjects
Study subjects and clinical data were obtained from the database of The Korean Cardiac Arrest Research Consortium (KoCARC) registry. The KoCARC is a collaborative research network organized in 2014 which consists of seven research committees including Epidemiology and Preventive Research Committee (EPR), Community Resuscitation Research Committee (CRR), EMS Resuscitation Research Committee (ERR), Hospital Resuscitation Research Committee (HRR), Hypothermia and Post-resuscitation Care Research Committee (HPR), Cardiac Care Resuscitation Committee (CCR) and Pediatric Resuscitation Research Committee (PRR). The KoCARC has administrated multicenter registry database in the field of OHCA resuscitation (NCT03222999). The following conditions were excluded from the registry enrollment: 1) those with terminal illness, 2) those under hospice care, 3) those in pregnancy, 4) those with pre-documented ‘Do Not Resuscitate (DNR)’ card, 5) those who disagreed for registration and 6) those with definite non-cardiac cause comprising trauma, drowning, poisoning, burn, asphyxia or hanging. From October 2015 to June 2017, a total of 4,757 OHCA patients who were transported to 32 participating emergency departments with resuscitation efforts were registered. For the current study, 1,523 (32.0%) patients achieved a return of spontaneous circulation; of these patients, 516 (33.9%) underwent ICA during hospitalization.
Data collection
Clinical characteristics, including age and gender as well as the history of cardiovascular risk factors such as hypertension, diabetes mellitus, dyslipidemia, current smoking and family history of CAD were acquired. Hypertension was defined as previous history of hypertension or use of antihypertensive medication. Diabetes mellitus was defined as prior history of diabetes mellitus or use of antidiabetic medication. Dyslipidemia was also defined as previous history of dyslipidemia or anti-dyslipidemic medication. Current smoking was defined as regular smoking habit in the past 12 months. Patients with family members who were diagnosed for CAD with or without coronary revascularization were defined as positive family history of CAD. Data on resuscitation comprising bystander cardiopulmonary resuscitation (CPR), bystander application of automated external defibrillator (AED) and time duration of CPR was also obtained. Initial ECG was reviewed for the presence of shockable rhythm (ventricular fibrillation or pulseless ventricular tachycardia) or non-shockable rhythm (pulseless electrical activity or asystole). A positive cardiac enzyme was defined based on initial laboratory data on cardiac enzymes such as creatine kinase-MB (CK-MB) (> 5 ng/mL) or cardiac troponin I (> 0.028 ng/mL). Data on the treatment after ICA including percutaneous coronary angiography (PCI), coronary artery bypass graft surgery (CABG), intra-aortic balloon pump (IABP), implantable cardioverter defibrillator (ICD), and extracorporeal membrane oxygenation (ECMO) was also obtained.
ICA
The severity of coronary artery stenosis and the extent of CAD such as multi-vessel disease or left main CAD were evaluated at the time of ICA. Further treatment strategies such as revascularization and medical treatment were determined by attending physicians' preference based on the ICA results. Obstructive CAD was defined as the lesion with % diameter stenosis ≥ 50% in 1 or more major epicardial coronary arteries.
Statistical analysis
Baseline characteristics, including demographic information, cardiovascular risk factors, information on cardiac resuscitation, laboratory results and post-ICA treatment, were compared between patients according to ICA and the presence of obstructive CAD. Continuous variables are presented as mean with standard deviation or median with interquartile range, and were compared using Student's t-test for parametric variables or Mann–Whitney U test for non-parametric variables. Categorical variables are presented as numbers with percentage and were compared by the χ2 test. To investigate independent factors associated with obstructive CAD, multivariable logistic regression analysis was performed. The following potential confounders were controlled in the multivariable analysis: age, gender, hypertension, diabetes mellitus, dyslipidemia, current smoking, family history of CAD, positive result of initial cardiac enzyme and presence of shockable rhythm at initial ECG. To assess the discrimination ability of clinical information on obstructive CAD, 4 prediction models were constructed. Baseline prediction model (model 1) was derived from age and gender. Next, model 2 was designed by combining cardiovascular risk factors (model 1 + hypertension + diabetes mellitus + dyslipidemia + current smoking + family history of CAD). Then, model 3 was derived by combining positive results of the cardiac enzyme (model 2 + positive cardiac enzyme). The final model (model 4) included the results of initial ECG (model 3 + initial shockable rhythm). The discriminatory ability of each prediction model was assessed using the area under the receiver operator characteristics curve (AUC) with 10,000 permutation resampling method. The distributions of estimated AUC for incremental models from models 1 to 4 were compared. To evaluate the association of ICA with long-term prognostic benefit among OHCA patients, 1-year cumulative risk of death was assessed for patients who underwent ICA (n = 516) and those who did not (n = 1,007) after resuscitation by Kaplan-Meier survival analysis and compared using Cox proportional hazard model adjusting baseline characteristics. All analyses were performed 2-sided, and a P value of < 0.05 was considered statistically significant. All data was analyzed using SPSS version 21.0 for Windows (IBM, Armonk, NY, USA) and R, version 3.5.3 (R Development Core Team, Vienna, Austria).
Ethics statement
The study protocol complied with the Declaration of Helsinki, and was reviewed and approved by the Institutional Review Board (IRB) of the Seoul Metropolitan Government-Seoul National University Boramae Medical Center (IRB No. 16-2014-32). The study was waived for informed consent by the IRB.
RESULTS
Clinical characteristics of the study patients
Of 4,757 OHCA patients, 516 underwent ICA, and 254 (49%) of them had obstructive CAD. Table 1 shows clinical characteristics of patients according to ICA and those with and without obstructive CAD. Patients who underwent ICA were younger (58 vs. 66 years, P < 0.001), had a higher proportion of men, and had higher prevalence of hypertension (45% vs. 39%, P < 0.001), dyslipidemia (7% vs. 4%, P = 0.008), current smoking (32% vs. 10%, P < 0.001), and family history of CAD (4% vs. 1%, P < 0.001). Regarding resuscitation, ICA group had a higher proportion of bystander CPR (56% vs. 43%, P < 0.001), bystander AED (2.1% vs. 0.4%, P < 0.001) and shorter duration of CPR. At initial presentation, those who underwent ICA showed higher rates of positive cardiac enzymes (79% vs. 46%, P < 0.001) and shockable rhythm on ECG (66% vs. 12%, P < 0.001). Comparisons of clinical characteristics between patients with and without obstructive CAD is also demonstrated in Table 1. Patients with obstructive CAD were older (61 vs. 55 years, P < 0.001), and had higher prevalence of hypertension (54% vs. 36%, P < 0.001) and diabetes mellitus (29% vs. 21%, P = 0.032) than those without. There was no difference in the proportion of bystander CPR, bystander AED and duration of CPR between the 2 groups. Compared to patients without obstructive CAD, those with obstructive CAD showed higher rates of having positive cardiac enzymes (84% vs. 74%, P = 0.010) and shockable rhythm at initial ECG (70% vs. 61%, P = 0.033). Among the patients with obstructive CAD, 58.3% (n = 148), 5.5% (n = 14), 4.7% (n = 12), 1.6% (n = 4), and 7.9% (n = 20) received treatment with PCI, CABG, IABP, ICD, and ECMO, respectively. Those with obstructive CAD showed a significantly higher rate of PCI (58% vs. 10%, P < 0.001) and IABP (5% vs. 2%, P = 0.018), whereas a lower rate of ICD insertion (2% vs. 11%, P < 0.001) compared to those without.
Table 1
Clinical characteristics of study patients
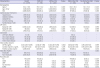
Values are given as mean ± standard deviation, median (interquartile range, 25th and 75th percentile) or number (%) unless otherwise indicated.
ICA = invasive coronary angiography, CAD = coronary artery disease, CPR = cardiopulmonary resuscitation, AED = automated external defibrillator, CK-MB = creatine kinase-MB, ECG = electrocardiogram, PCI = percutaneous coronary intervention, CABG = coronary artery bypass graft surgery, IABP = intra-aortic balloon pump, ICD = implantable cardioverter defibrillator, ECMO = extracorporeal membrane oxygenation.
Independent risk factors associated with obstructive CAD
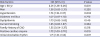
Independent risk factors associated with obstructive CAD are shown in Table 2. In binary multiple logistic regression analysis, older age (≥ 60 years) (odds ratio [OR], 2.01; 95% confidence interval [CI], 1.36–3.00; P = 0.001), hypertension (OR, 1.74; 95% CI, 1.18–2.57; P = 0.005), positive cardiac enzyme (OR, 1.72; 95% CI, 1.09–2.70; P = 0.019) and initial shockable rhythm (OR, 1.71; 95% CI, 1.16–2.54; P = 0.007) were associated with obstructive CAD even after controlling for potential confounders.
Table 2
Independent risk factors associated with obstructive CAD
Four different prediction models for obstructive CAD
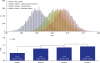
Table 3 and Fig. 1 present the discrimination ability of prediction models from the various combination of clinical information. Model 1 showed modest performance in prediction for obstructive CAD (AUC, 0.601; 95% CI, 0.600–0.602). The discriminant ability was improved when cardiovascular risk factors were added to model 1 (“model 2”) (AUC, 0.601 to 0.658; P < 0.001). Model 2 with cardiac enzyme (“model 3”) also showed significantly improved discriminant ability compared to model 2 (AUC, 0.658 to 0.673; P < 0.001). When information on initial shockable rhythm was combined to model 3 (“model 4”), the highest performance of discrimination was found (AUC, 0.673 to 0.687; P < 0.001).

Prognostic impact of ICA among OHCA patients
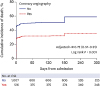
OHCA patients who underwent ICA was associated with a significantly lower rate of 1-year mortality compared to those who did not (log-rank P < 0.001, Fig. 2). After adjusting baseline characteristics, ICA group consistently showed a lower risk of mortality (adjusted hazard ratio, 0.72; 95% CI, 0.57–0.91).
DISCUSSION
The present study showed that old age, hypertension, positive cardiac enzyme and shockable rhythm at initial ECG were independently related to higher risk of obstructive CAD in patients with ROSC after OHCA. Our study also demonstrated incremental prediction abilities for obstructive CAD when these 4 factors were sequentially added.
The role of ICA in patients with OHCA
As CAD is the most common cause of OHCA, previous studies have assessed the clinical benefit of early ICA on survival or good neurologic outcome among patients after OHCA.25671112 Although some studies have demonstrated the prognostic benefit of early ICA in patients after OHCA,256712 others showed no benefit of early invasive approaches.11 As previous studies were not randomized but retrospectively designed, discordance among studies could be attributed to different baseline characteristics. Indeed, as the prevalence of obstructive CAD was higher in studies showing a positive prognostic impact of ICA,56 compared to those presenting no benefit of ICA in OHCA patients.11 This implies that immediate ICA for patients who are highly suspected for obstructive CAD will maximize the prognostic benefit of ICA. However, imprudent application of early ICA after OHCA may increase not only false positive test results but also delay proper differential diagnosis.20 Moreover, ICA is sometimes associated with an increased risk of fatal bleeding following unnecessary antithrombotic treatment,172122 and its invasiveness increases the mortality rate.18 Therefore, appropriate discrimination of patients who have obstructive CAD is also essential to minimize the potential risk of early ICA among OCHA patients. In our study results, OHCA patients who underwent ICA showed a significantly lower rate of 1-year mortality. Also, we found 4 clinical factors associated with obstructive CAD in patients with OHCA, which can be obtained at early phases on initial presentation. Identification of these 4 factors may have prognostic values in augmenting clinical benefit of ICA among patients with OHCA.
Traditional risk factors and ECG changes
Traditional cardiovascular risk factors and ECG changes can be clues to obstructive CAD in patients with OHCA. It has been suggested that patients with acute coronary syndrome (ACS) or obstructive CAD tend to have higher rate of cardiovascular risk factors compared to those without.23 ST segment changes in post-resuscitation ECG have been widely adopted as a guideline for deciding coronary revascularization,13 although several studies have raised questions for its value in prediction.141516 Abe et al.24 reported a prediction model for identifying patients who have angiographically normal coronary arteries after OHCA by retrospectively analyzing 47 consecutive adult survivors who underwent immediate ICA after resuscitation. In that study, patients without diabetes mellitus, previous history of ACS and ST-segment abnormalities were associated with normal coronary arteries. Higny et al.9 demonstrated clinical factors related to significant CAD in patients without ST-segment elevation after OHCA, which were the previous history of CAD, and the presence of cardiovascular risk factors including diabetes mellitus and dyslipidemia. In line with those studies, our results also showed that, among cardiovascular risk factors, old age and the presence of hypertension were independently associated with obstructive CAD in OHCA patients. Previously, patients at younger age were reported to be related to better neurologic and functional outcome after OHCA, which may have been attributed to the relatively lower burden of cardiovascular risk factors.2526 We suggest a possibility that poor prognoses in elderly patients with OHCA could be partially due to a lower rate of ICA,27 despite higher risk of obstructive CAD as in our study results. Recently, Legriel et al.28 indicated the benefit of early ICA in elderly patients after OHCA, suggesting that elderly patients should be more optimally managed with appropriate treatment.
Hypertension is one of the traditional cardiovascular risk factors. Compared to those without hypertension, patients with hypertension were related to increased prevalence and severity of CAD including extent and calcification, and were associated with higher risk of adverse cardiovascular events.2930 Also, previous studies have reported hypertension as an independent risk factor for OHCA among patients with CAD as well as poor in-hospital and subsequent long-term outcome after resuscitation.3132 Although the pathophysiologic association between hypertension and OHCA in patients with CAD is not completely understood, several explanations have been proposed.32 Hypertension leads to myocardial hypertrophy which augments myocardial ischemia caused by obstructive CAD as coronary arteries fail to grow with a sufficient rate to supply hypertrophic myocardium.33 Additionally, hypertrophic myocardium is arrhythmogenic compared to normal myocardium, which is more vulnerable to ectopic trigger leading to lethal arrythmias.34 Increased activity of sympathetic nerves and the renin-aldosterone system in hypertensive status could also involve the arrhythmogenic condition of the myocardium.35
Initial shockable rhythm
Patients with initial shockable rhythm have considered to be associated with higher risk of myocardial infarction (MI) as an origin for OHCA and are likely to be referred for ICA.2736 Youngquist et al.37 investigated 151 autopsy cases of OHCA patients with failed resuscitation and found that 43% of the OHCA cases were related to coronary occlusion. They also stated that old age and initial shockable rhythm were associated with CAD, which is consistent with ours. Also, previous studies of patients who had intracranial hemorrhage as a cause of OHCA found that the prevalence of shockable rhythm was significantly lower compared to those who did not.1738 Although regarding the role of shockable rhythm as a positive prognostic factor is not fully understood in MI patients, a short time to administration of medical assistance and a relatively lower burden of myocardial ischemia may contribute to better outcome in those with shockable rhythm.39 This may be supported by a previous experimental study showing that cardiac arrest secondary to severe hypoxemia or respiratory arrest causes asystole rather than shockable rhythm and severe global ventricular dysfunction.40
Clinical implications
Identifying patients with OHCA related to obstructive CAD is important for not only maximizing the clinical benefit of early coronary revascularization but also avoiding unnecessary invasive procedures. In the current study, we found 4 clinical factors associated with obstructive CAD in patients with OHCA, which included old age, hypertension, positive cardiac enzyme and initial shockable rhythm on ECG. As information on all these clinical factors can be obtained easily in a short time period at initial presentation, identification of these 4 factors may be clinically valuable in selecting patients and maximizing benefit of ICA in the setting of OHCA.
Study limitations
There are several limitations in this study. First, although we screened patients from the multicenter OHCA registry, the number of patients included for analysis is relatively small. Secondly, as this study was retrospectively designed, some concerns could be raised regarding the selection of patients who survived to undergo ICA. Therefore, it could be limited to generalize our study results for overall OHCA patients. Thirdly, the association of traditional cardiovascular risk factors with obstructive CAD may differ in other populations with a different prevalence rate of the risk factors. Finally, clinical outcome data is not available in our cross-sectional analysis.
In summary, among the patients with OHCA and ROSC, old age, hypertension, positive cardiac enzyme test and initial shockable rhythm may be associated with obstructive CAD. Early ICA should be considered in this group of patients with these risk factors.
 XML Download
XML Download