

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Restless legs syndrome (RLS), also known as Willis-Ekbom disease, is a neurological sensorimotor disorder characterized by a strong urge to move the legs and by unpleasant, creeping sensations within the legs.1 These symptoms mainly occur at rest, worsen in the evening or at night, and improve with movement, such as walking and stretching.2 Sleep disturbance is a major consequence of RLS; as shown in previous studies, RLS is associated with insomnia, poor sleep quality, and excessive daytime fatigue and sleepiness.34 In agreement with these reports, polysomnographic studies have demonstrated that RLS is characterized by longer sleep latency, higher arousal index, and lower sleep efficiency compared with those in controls.56 RLS is also associated with cognitive dysfunction, such as decreased frontal executive function and mental flexibility, which might be mediated by chronic sleep loss, reduced attention, and psychiatric comorbidities.7
Evidence has been accumulating that RLS is associated with increased risk of cardiovascular diseases.89 A prospective study showed that women with RLS lasting for ≥ 3 years had a significantly higher risk of incident coronary heart disease than those without RLS.10 However, this association remains inconclusive because contradictory results have been reported in other prospective studies.1112 Several possible mechanisms may account for the increased risk of cardiovascular diseases in RLS patients. Periodic limb movements in sleep (PLMS), commonly accompanied by RLS, are associated with sympathetic activation and blood pressure elevation.1314 RLS is also associated with a non-dipping pattern of nocturnal blood pressure, which might be responsible for hypertensive target organ damage.15 Furthermore, short sleep duration and insomnia resulting from RLS can act as a risk factor for cardiovascular diseases.16
In this context, the association of RLS with hypertension has also been suggested. However, as previous studies have reported mixed results, a definitive conclusion regarding the possibility of RLS being linked to hypertension has not been reached.17 Furthermore, prior epidemiological studies have predominantly investigated the Caucasian population, and relatively little research has focused on the association between RLS and hypertension in Asian adults.1819 The current general consensus is that the prevalence of RLS in Asian countries is lower than that in Western countries.20 Furthermore, Asian patients with RLS are characterized by a lower rate of coexisting PLMS than Caucasian adults with RLS.2122 These ethnic differences suggest an important role of genetic background in RLS pathophysiology. Therefore, we herein investigated the prevalence of RLS and its association with hypertension in a cross-sectional nationwide sample of the Korean adult population.
METHODS
Study sample
The subjects of this study were participants in the Korean Headache-Sleep Study (KHSS). The KHSS is a nationwide, cross-sectional, questionnaire-based survey for sleep and headache in Korean adults aged ≥ 19 years.23 Gallup Korea conducted the survey in a sampled population through face-to-face interviews as previously described.24 Briefly, in 2009, the estimated number of the Korean adult population aged ≥ 19 years was 37,782,000. The number of target population was 2,800, which was sampled from 15 administrative districts according to the clustered, proportionate quota sampling method. Among 7,615 individuals approached by trained interviewers, 2,836 (37.2%) completed the survey with the sampling rate of 7.5 individuals per 100,000. We excluded 96 subjects because of incomplete data on sleep habits (n = 22), sleep questionnaires (n = 20), and socio-demographic information (n = 54). Therefore, we eventually analyzed data from 2,740 subjects in this study.
Diagnosis of RLS
We used the 2003 National Institutes of Health/International Restless Legs Syndrome Study Group (IRLSSG) criteria for the diagnosis of RLS.2 First, we identified subjects who met the four essential criteria for RLS. For criterion 1, positive responses to the following two questions were required: “Do you have, or have you had, recurrent uncomfortable feelings or sensations in your legs while you are sitting or lying down?” and “Do you, or have you had, a recurrent need or urge to move your legs while you are sitting or lying down?” For criterion 2, subjects had to answer “resting” to the question “Are you more likely to have these feelings when you are resting (either sitting or lying down) or when you are physically active?” To meet criterion 3, participants had to answer “yes” to the question “If you get up or move around when you have these feelings, do these feelings get any better while you actually keep moving?” Finally, those who answered “evening” and/or “night” to the question “At which times of day are these feelings in your legs most likely to occur?” were considered to meet criterion 4. We additionally investigated the frequency of RLS symptoms with the options of “every day,” “4–5 days a week,” “2–3 days a week,” “1 day a week,” “2 days a month,” and “1 day a month or less.” Finally, the RLS group was defined as subjects who met the four essential criteria and reported a frequency of RLS symptoms of ≥ 1/week. Controls were defined as those who did not meet the essential criteria, or who met the essential criteria but reported RLS symptoms less than once weekly.
Self-reported hypertension
The presence of hypertension, a variable of primary interest in this study, was defined as a self-reported history of physician-diagnosed hypertension. Thus, subjects who answered “yes” to the question “Have you ever been told by a doctor that you have hypertension?” were defined to have self-reported hypertension.
Other examined parameters
We investigated age, gender, body mass index (BMI), education level, alcohol consumption, smoking status, physical activity, and other cardiovascular risk factors, such as diabetes mellitus and hyperlipidemia. Based on the BMI, the subjects were classified as underweight (< 18.5 kg/m2), normal weight (18.5–25 kg/m2), and overweight (≥ 25 kg/m2). Alcohol consumption was evaluated based on the frequency of alcohol intake, and the responses were categorized into three groups: ≥ 2 days a week, ≤ 1 day a week, and none. Smoking status was categorized as current smoker, ex-smoker, and never-smoker. Physical activity was assessed by the question “How many days per week have you done vigorous physical activities making you sweaty?” and the responses were classified as ≥ 3 days a week, 1–2 days a week, and none.
We investigated sleep-related variables, such as average sleep duration, insomnia, chronotype, and presence of habitual snoring. Average sleep duration was calculated as the weekly average of weekday and weekend sleep duration: [(weekday sleep duration × 5) + (weekend sleep duration × 2)]/7. According to the insomnia severity index score, we evaluated insomnia with the following categories: 15–28, clinical insomnia; 8–14, subthreshold insomnia; and 0–7, no insomnia.25 Chronotype was measured by the midpoint of sleep on free days corrected for free-day oversleep.26 In addition, the subjects were asked the question “How often do you snore?” and the snoring frequency of ≥ 3 nights a week was defined as habitual snoring.
Statistical analysis
We compared the clinical characteristics between RLS patients and controls. We used Student's t-test for continuous variables, and Pearson's χ2 test or Fisher's exact test for categorical variables. Then, we performed multiple logistic regression analyses to determine the independent association between RLS and self-reported hypertension. The presence of self-reported hypertension was set as a dependent variable, while the presence of RLS was an independent variable. This model was adjusted for covariates that showed P values of < 0.1 in the univariate analyses. Potential confounding factors were additionally included as covariates. The level of statistical significance was defined as a two-tailed P value of < 0.05. All statistical analyses were carried out using SPSS version 18 (SPSS Inc., Chicago, IL, USA).
Ethics statement
We obtained written informed consent from all participants before enrollment. All information gathered in the survey was anonymized to preserve the participants' privacy. This study was approved by the Institutional Review Board of Soonchunhyang University Cheonan Hospital (No. 2017-03-028) and conducted in accordance with the Declaration of Helsinki and the Good Clinical Practice guidelines.
RESULTS
In a total of 2,740 subjects, the mean age was 44.5 ± 15.0 years, the mean BMI was 23.0 ± 3.0 kg/m2, and 1,372 (50.1%) were women. The prevalence of self-reported hypertension was 12.9% (95% confidence interval [CI], 11.6%–14.2%). One hundred fifty-two (5.5%) subjects met the four essential criteria for RLS, and among them 68 (2.5%; 95% CI, 1.9%–3.1%) were identified as the RLS group whose RLS symptoms occurred at least once a week. The prevalence of RLS was 3.2% (95% CI, 2.3%–4.2%) in women and 1.8% (95% CI, 1.1%–2.5%) in men. The clinical characteristics of the RLS group are summarized in Table 1. Hypertension was more frequently reported in the RLS group (30.9%; 95% CI, 20.5%–42.0%) than in controls (12.4%; 95% CI, 11.2%–13.6%). In the univariate analyses, the RLS group was significantly associated with old age (odds ratio [OR], 1.04; 95% CI, 1.02–1.05) and the women gender (OR, 1.86; 95% CI, 1.12–3.07). Moreover, the RLS group was associated with a low education level (OR, 2.61; 95% CI, 1.49–4.57), not drinking alcohol (OR, 2.02; 95% CI, 1.25–3.28), diabetes mellitus (OR, 2.28; 95% CI, 1.02–5.09), short sleep duration (OR, 0.73; 95% CI, 0.61–0.88), and insomnia (subthreshold, OR, 4.76; 95% CI, 2.73–8.29; clinical, OR, 8.58; 95% CI, 4.45–16.52).
Table 1
Clinical information according to presence of restless legs syndrome

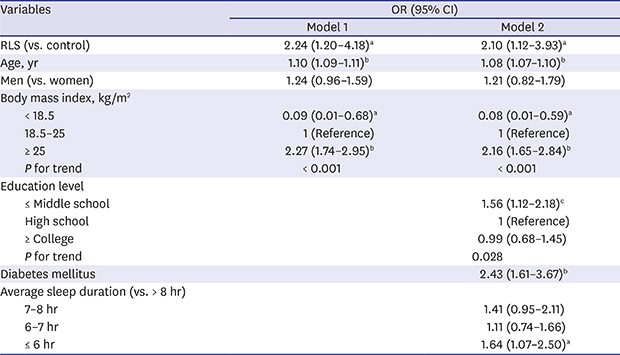
Next, we conducted multivariate logistic regression analysis to determine the independent association between the RLS group and self-reported hypertension after adjusting for confounding variables. In this model, age, gender, BMI, education level, alcohol drinking, smoking status, physical activity, diabetes mellitus, habitual snoring, average sleep duration, and insomnia were included as covariates. We found a significant association of the RLS group (OR, 2.10; 95% CI, 1.12–3.93) with self-reported hypertension after adjusting for the covariates. As shown in Table 2, self-reported hypertension was also significantly associated with old age (OR, 1.08; 95% CI, 1.07–1.10), being overweight (BMI ≥ 25 kg/m2; OR, 2.16; 95% CI, 1.65–2.84), low education level (OR, 1.56; 95% CI, 1.12–2.18), diabetes mellitus (OR, 2.43; 95% CI, 1.61–3.67), and short average sleep duration (≤ 6 hours per night; OR, 1.64; 95% CI, 1.07–2.50). In addition, we observed a linear trend in the adjusted ORs of the BMI categories (P for trend < 0.001) and education levels (P for trend = 0.028) for self-reported hypertension. However, habitual snoring showed only a marginal association with the prevalence of hypertension (OR, 1.22; 95% CI, 0.91–1.65). Moreover, no significant interaction effect was found between gender and RLS symptoms on the prevalence of self-reported hypertension (P = 0.703).
Table 2
Multivariate logistic regression analysis for self-reported hypertension
Model 1 was adjusted for age, gender, and body mass index. Model 2 was adjusted for the variables in model 1 plus education level, alcohol drinking, smoking status, physical activity, diabetes mellitus, average sleep duration, habitual snoring, and insomnia.
OR = odds ratio, CI = confidence interval, RLS = restless legs syndrome.
aP < 0.05; bP < 0.001; and cP < 0.01.
DISCUSSION
In this study, we found a significant association between RLS symptoms and self-reported hypertension. This association was independent of potential confounders, such as age, gender, BMI, education level, alcohol drinking, smoking status, physical activity, diabetes mellitus, habitual snoring, insomnia, and average sleep duration. To the best of our knowledge, this is the first study to investigate the effect of RLS symptoms on the prevalence of hypertension in a nationwide sample of the Korean adult population, which is the main strength of this study. Previous studies have shown that the prevalence of RLS and coexisting PLMS differ by race and ethnicity.202127 Although it is also possible that the relationship between RLS and hypertension may be affected by ethnic differences, there have been relatively little studies performed in Asian adults.1819 Therefore, it is of importance that our results provide novel information that an independent association may exist between RLS symptoms and hypertension among Korean adults.
Batool-Anwar et al.28 reported that women with RLS were 1.2 times more likely (95% CI, 1.10–1.30) to have hypertension compared to those without RLS after controlling for confounders. This association was further supported by a significant dose-response relationship between the RLS symptom frequency and the risk of hypertension. In addition, two recent meta-analyses have demonstrated a significant association between RLS and hypertension.2930 Furthermore, a retrospective cohort study with a mean follow-up of 3.9 years showed that, compared to controls, RLS patients had a significantly higher risk of incident hypertension, which supports the hypothesis that RLS may act as an independent risk factor for hypertension.31 However, a prospective cohort study in Germany showed that RLS status at baseline was not a significant predictor of incident hypertension or any cardiovascular diseases.12 Therefore, further prospective studies are required to address the controversy regarding the association between RLS and hypertension, as well as its directionality.
Regardless of the symptom frequency, the prevalence of RLS was found to be 5.5% in this study. However, when the frequency criterion of at least once a week was included, the prevalence of RLS decreased to 2.5%. We used this frequency criterion because RLS symptoms occurring less than once a week are considered have little impact on sleep and hypertension. In line with this, subjects with RLS symptoms occurring at least 5 times per month were defined to have symptomatic RLS in previous studies.928 It has been well known that among patients who fulfilled the four essential IRLSSG criteria, approximately 50%–60% report RLS symptoms occurring at least once a week.20 Similarly, a previous Korean nationwide survey of RLS using the Johns Hopkins telephone diagnostic interview reported that the prevalence of definite RLS with a frequency of at least once a week and with any frequency was 2.0% and 3.9%, respectively.32 In addition, a community-based study revealed that 8.3% of the Korean elderly population were diagnosed as having RLS.33 In accordance with this report, the prevalence of RLS with any frequency among those aged ≥ 65 years in our study was 10.1%. Moreover, the prevalence of RLS with a frequency of at least once a week among Korean women was reported as 3.9%,34 which is comparable to that of 3.2% in our data. Collectively, our results are largely consistent with the results of the previous Korean epidemiological studies, indicating that our study sample represents the adult population of Korea and that the definition of RLS based on the IRLSSG criteria was appropriate.
Among the strengths of this study is the adjustment for sleep-related risk factors of hypertension, such as habitual snoring, insomnia, and short sleep duration, in the multivariate logistic model. Adjusted variables in previous cross-sectional studies mostly were socio-demographic factors rather than sleep-related factors. In line with previous studies,3536 our results demonstrated a significant association between short sleep duration and increased risk of hypertension. In addition, chronic insomnia has been reported to be associated with an increased risk of hypertension.3738 Notably, Vgontzas et al.37 found that the association between insomnia and hypertension was significant only when insomnia was accompanied by short sleep duration (≤ 6 hours per night). Finally, a bidirectional relationship between obstructive sleep apnea (OSA) and hypertension has been well established in epidemiological and experimental studies.39 Habitual snoring, a subjective measure of sleep disordered breathing commonly used in epidemiological studies, has also been found to be an independent risk factor for incident hypertension in previous prospective cohort studies.404142 In this regard, we found a weak, albeit not significant, association between habitual snoring and hypertension in this study. However, this finding should not be mistakenly interpreted that there is no possible association between OSA and hypertension. Further studies with polysomnographic evaluations are warranted to determine the effect of OSA on the relationship between RLS and hypertension.
This study has several limitations. OSA is a sleep-related risk factor for hypertension, which should be controlled for when evaluating the association between RLS and hypertension. However, because polysomnographic evaluations of sleep apnea were not conducted in this questionnaire-based study, habitual snoring rather than the apnea-hypopnea index was included as a covariate. For the same reason, PLMS, although its clinical significance as a risk factor for hypertension has not been clear yet, was not investigated in this study. Therefore, our analysis might not have fully controlled for the effect of OSA and PLMS on hypertension. Another limitation is that hypertension was defined as a self-reported history of physician-diagnosed hypertension. Although self-reported hypertension has been commonly used in population-based studies, an analysis based on objective measurements of blood pressure could have provided more convincing evidence regarding a link between RLS and hypertension. The effect of antihypertensive drugs or RLS medications on the association between hypertension and RLS was not considered in our analysis, which is another limitation of this study. In addition, because we defined RLS based on diagnostic questionnaires and symptom frequency, possible mimics of RLS, such as nocturnal leg cramps, peripheral neuropathy, and anxiety, might have been mistakenly included. However, it is essentially impossible to perform thorough neurological examination in a population-level study. The Cambridge-Hopkins diagnostic questionnaire for RLS may be useful to diagnose RLS while excluding potential mimics,43 although a larger sample size will be required to produce statistical significance. Finally, the cross-sectional design of this study precludes drawing any conclusions about causality.
In summary, the prevalence of RLS with symptoms occurring at least once a week was 2.5% in Korean adults. Although the association between RLS and hypertension remains controversial, our results support that RLS symptoms might be independently associated with a high risk of hypertension. Despite several limitations, this study represents our own ethnic data about the relationship between RLS and hypertension, which needs to be confirmed in the future.
 XML Download
XML Download