

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Oral allergy syndrome (OAS) is an immunoglobulin E (IgE)-mediated hypersensitivity that occurs frequently in older children with pollen sensitization. OAS results from the cross-reactivity between pollen sensitization and food proteins due to their homologous protein structures. OAS is therefore also known as pollen-food syndrome. Patients who are sensitized to pollen frequently present with allergic symptoms after the ingestion of certain fruits, vegetables, and nuts.
The symptom complex consists of itching, a tingling or burning sensation, and swelling of the lips, mouth, and throat immediately after the ingestion of plant-derived foods. The symptoms may sometimes develop into urticaria, conjunctivitis, nausea, vomiting, asthma, and anaphylaxis.12
The number of epidemiological studies investigating OAS in pediatric populations is limited. A few international studies have reported that the prevalence of OAS is 5.0%–29.7% in children and 4.1%–70.0% in adults.345678910111213 A nationwide multicenter study conducted in Korea in 2017 reported that the prevalence of OAS in Korean pollinosis patients was 41.7%.14
Birch pollen-related food allergy is considered a common immunologic cross-reactivity between ubiquitous birch pollen and structurally related food proteins. Food proteins also interact with each other.151617 There are only a few studies regarding OAS in atopic dermatitis (AD) children, and birch sensitization exacerbates their skin and perioral symptoms when they eat certain foods. The OAS symptoms are reported more often by patients with a birch pollen allergy (70%) than by patients without a birch pollen allergy (19%).181920 We therefore focused our study on OAS in children with birch pollen sensitization.
The aim of this study was to determine the characteristics of OAS in the Korean pediatric population with birch pollen sensitization and AD.
METHODS
Patients
Outpatients attending the Department of Pediatrics at Soonchunhyang University Hospital between January 2016 and March 2017 were recruited for this study. A total of 186 patients aged 2–18 years who had AD and birch sensitization were enrolled in this study. We performed a retrospective medical record review of the enrolled patients. The patients were divided into 3 groups according to their ages (group 1, 2–6 years; group 2, 7–12 years; and group 3, 13–18 years).
Serum specific IgE (sIgE) measurements
Blood samples were taken to detect the patients' total IgE (tIgE) and birch-sIgE levels using the ImmunoCAP test (Thermo Fisher Scientific, Uppsala, Sweden) at their first or follow-up visits. Levels were expressed in kUA/L within 7 classes, the upper limits of which were: class 0, 0.35 kUA/L; class 1, 0.7 kUA/L; class 2, 3.5 kUA/L; class 3, 17.5 kUA/L; class 4, 50 kUA/L; class 5, 100 kUA/L; class 6, > 100 kUA/L. The classes ≥ 1 were considered positive.
Pediatric population interviews
Interviews regarding their OAS symptoms (e.g., itching, burning, swelling, and rash) were carried out with the children with AD and birch sensitization. Information about the kinds and number of causative foods was also obtained. If children could not explain their symptoms and causative foods, we obtained the information from their parents.
Statistics
A two-tailed unpaired t-test or otherwise a nonparametric Mann-Whitney U test was applied to compare the results between the groups. The χ2 test or Fisher's exact test was used to compare the frequencies between the groups. A P value < 0.05 was considered statistically significant. The cut-off level of sIgE against birch to predict OAS was determined by analyzing the receiver operating characteristic (ROC) curves. SPSS version 22.0 (SPSS Inc., Chicago, IL, USA) was used for all the analyses.
RESULTS
Demographics and prevalence
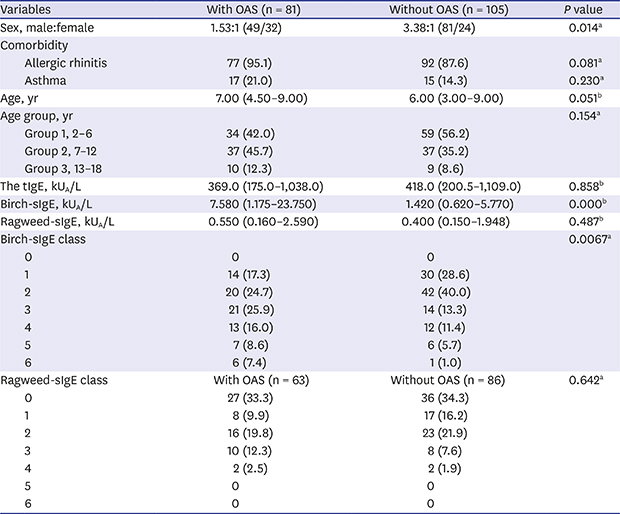
A total of 186 patients with AD and birch sensitization (130 male and 56 female patients) were included in this study. Of these, 81 (43.5%) had OAS at the time of their visit to the hospital. The number of male patients with OAS was 49 while the number of female patients with OAS was 32. Eighty-six patients (46.2%) had ragweed co-sensitization. The data on sex, age, tIgE, birch-sIgE, ragweed-sIgE, and comorbidities of allergic rhinitis and asthma were summarized according to the existence of OAS (Table 1).
Table 1
The characteristics of OAS and the absence of OAS in pediatric patients with birch sensitization and AD

Values are presented as median (interquartile range) or number (%).
OAS = oral allergy syndrome, AD = atopic dermatitis, tIgE = total immunoglobulin E, sIgE = specific immunoglobulin E.
aThe Pearson χ2 test was used to compare the frequencies among the groups; bThe Mann-Whitney U test was used to compare the continuous variables among the groups when the condition was respected.
There was a difference in the male:female sex ratio between the patients with OAS and those without OAS (P = 0.014). A comparison of the male:female sex ratios of the patients revealed a much smaller difference (1.53:1) for those with OAS compared to those without OAS (3.38:1) (sex ratio for the total population, 2.32:1).
Most of the study population (90.9%, 169/186) had allergic rhinitis, and 17% (32/186) had asthma. However, no relevant difference was found in their comorbidities according to the existence of OAS. There was also no statistical difference in age between with those with OAS (median, 7.0; interquartile range [IQR], 4.50–9.00) and those without OAS (median, 6.0; IQR, 3.00–9.00).
Correlation between pollen sIgE and OAS
We analyzed the serum levels of tIgE (n = 186), birch-sIgE (n = 186), and ragweed-sIgE (n = 149). No difference in tIgE levels between the patients with OAS and those without OAS was found (median, 369.0 kUA/L; IQR, 175.0–1,038.0 and median, 418.0 kUA/L; IQR, 200.5–1,109.0, respectively). There was also no statistical difference in the levels of ragweed-sIgE between the patients with OAS and those without OAS (median, 0.550; IQR, 0.160–2.590 and median, 0.400; IQR, 0.150–1.948, respectively). Additionally, the OAS prevalence of the group with ragweed sensitization and without ragweed sensitization showed no statistical difference (44.2% vs. 39.7%, respectively).
However, the birch-sIgE levels were significantly higher in the group with OAS (median, 7.580; IQR, 1.175–23.750) than in the group without OAS (median, 1.42; IQR, 0.620–5.770). When comparing the presence of OAS by birch-sIgE class, it was found that the proportion of patients with OAS increased to birch-sIgE class 3 and above although there were more patients without OAS below class 3 (Table 1).
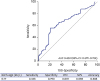
The ROC curve analysis indicated a birch-sIgE of 6.77 kUA/L, which was set as the optimal cut-off point for assessing the diagnostic value of OAS. The area under the curve (AUC) was 0.653, with a sensitivity of 55.6% and a specificity of 79.0% for the cut-off value of ≥ 6.77 required for an OAS diagnosis (Fig. 1).
Causative foods and symptoms
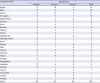
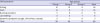
There were significant differences in the number of causative foods in each age group (P = 0.001). The older age groups described more causative foods than the younger groups (Table 2). The most frequent causative foods were apples (n = 33), followed in order by kiwis (n = 26), peaches (n = 21), and pineapples (n = 18). Kiwis were the most common causative food in group 1 (n = 11) while apples were in group 2 (n = 19) and group 3 (n = 5) (Table 3).
Table 2
The relationship between age groups in the pediatric population and the number of causative foods in OAS

Table 3
The causative foods of OAS among pediatric patients with AD and birch sensitization by age group
Itching was the most common symptom in this study, followed by rash across all the age groups. In the youngest age group (group 1), rash was the most common symptom (Table 4).
Table 4
The symptoms of OAS in pediatric patients with AD and birch sensitization by age group
DISCUSSION
In 1987, Amlot et al.18 first reported “oral allergy syndrome,” which comprises symptoms induced by eating a particular food. It includes primarily oral mucosal symptoms and, occasionally, systemic symptoms. The term “pollen-food allergy syndrome” is also used, but OAS is the more specific term. In 2003 and 2005, Ma et al.3 and Kondo and Urisu,19 respectively, reviewed OAS that is restricted to the oral mucosa.
The prevalence of OAS in children has rarely been investigated. In the United States in 2003,3 a survey among allergists reported that the prevalence of OAS was 5% in children with atopic diseases. Meanwhile, a study involving children with pollen-induced allergic rhinitis in Italy found that the prevalence was 24%.6 By way of contrast, a 2014 study in Australia7 assessing 163 patients aged 4–17 years found that the occurrence of OAS was 14.7%, while in Mexico in 2016,10 267 Mexican children with atopic disease, aged 6–14 years, were evaluated and the OAS prevalence was determined to be 8.9%. In this study, the prevalence of OAS was 45.7%, which is higher than that in other studies. This is because the study population was limited to birch sensitization children with AD.
There is no study on higher prevalence of OAS in the children with AD and birch sensitization. According to Eigenmann et al,21 the prevalence of food allergy in children with AD is significantly higher than the general population. Severity of AD is a major risk factor for food allergy22 and birch pollen-related food is a provocation factor of allergic symptoms in AD patients.23 In addition, it is already known that OAS and AD both belong to IgE mediated hypersensitivity.182425 For this reason, we presumed OAS and AD may be interrelated with each other, like the relationship between food allergy and AD. Further studies about the correlation analysis and case-control study between OAS with AD are necessary. Because the prevalence of OAS in group 1 (the children who had AD and birch sensitization aged 2–6 years) was 36.6% in this study, clinicians should be aware that OAS can occur in young children.
There was a difference in the sex ratio between the OAS group and the non-OAS group in this study. The percentage of male patients without OAS was 77.1% but 60.5% in those with OAS. This result is very similar to that of the Italian study, which reported that the percentage of male patients without OAS was 70% and, in those with OAS, 61%.6 Another study found that male patients without OAS accounted for 37.5% of the study population, which contrasted with the 28.1% of male patients with OAS.9 Further studies on OAS in relation to sex are thus required.
The Italian report6 stated that patients with allergic rhinitis had severe symptoms if they had asthma or OAS. Furthermore, patients with allergic rhinitis and AD have shown a higher prevalence of OAS.9 Notwithstanding, in this study there were no significant differences in the prevalence of comorbidities such as allergic rhinitis and asthma between the groups with OAS and those without OAS.
There are no standard diagnostic criteria for OAS. The diagnosis of OAS depends on the patient's clinical history and conformational tests such as the ImmunoCAP test (sIgE), skin prick test, and food challenge test.21126 We found a significant difference in birch-sIgE levels between the group with OAS (7.580) and the group without OAS (1.420). Moreover, when the class of birch-sIgE changed from 1 to 6, the prevalence increased concomitantly from 31.9% to 85.7%. Where birch-sIgE levels were class 3 or higher, there were more patients with OAS than those without OAS. This result means that levels of birch-sIgE can help diagnose OAS. We calculated the diagnostic value of birch-sIgE using the ROC curve. The cut-off value was 6.77 kUA/L with 55.6% sensitivity and 79.0% specificity (AUC 0.653).
No significant differences were identified in the prevalence of OAS according to the existence of ragweed sensitization (44.4% in the ragweed positive group and 41.9% in the ragweed negative group). The prevalence of OAS in terms of ragweed-sIgE levels showed no statistical differences, either. It seems that the influence of ragweed sensitization on OAS was low compared to that of birch sensitization. Some studies have shown that geographic and dietary differences account for various influences in OAS prevalence.6121317 An investigation should be done to determine the relationship between OAS and each kind of pollen sensitization in Korea. Nevertheless, further studies to improve diagnostic tests will also be necessary so that a more specific approach to the diagnosis of OAS in Korea can be developed.
The causative foods and symptoms differed depending on the age group. We found that the older age groups had a large number of causative foods than the younger groups. In this study, itching was the most common symptom, followed by rash. However, for group 1 (younger children aged 2–6 years), rash was the most common symptom. This may be because itching is not well expressed by young children whereas rash can be recognized quickly by parents. The most frequent causative foods were apples, followed in order by kiwis, peaches, and pineapples. This result mirrors those of other studies regarding the most common foods causing birch sensitization in OAS.31213152027
This study had some limitations. First, the prevalence of OAS was calculated for a specific population of children with both AD and birch sensitization. Because of that, the actual prevalence in the pediatric population could have been overestimated. Second, this study was performed in a single center. A nationwide study of the entire pediatric population is thus needed. Lastly, we could not conduct food challenge tests, and the information regarding causative foods was obtained through interviews with patients only.
The aim of this study was to determine the characteristics of OAS in the Korean pediatric population. There are many studies about OAS in children overseas; however, this is the first attempt to evaluate OAS in Korean children with AD and birch sensitization. Accordingly, our results have important implications for future studies about OAS in our country.
In conclusion, the prevalence of OAS in the children with AD and birch sensitization in this study was high at 43.5%. Even in the preschool age group, the prevalence of OAS was considerable. Furthermore, we found that patients with high levels of birch-sIgE were more likely to have OAS. Clinicians should therefore be vigilant about OAS in patients with a high degree of sensitization to birch pollen and even young children if they have birch sensitization.
 XML Download
XML Download