

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronary artery disease (CAD), which consists of angina pectoris and myocardial infarct (MI), is one of the leading causes of death in South Korea, due to the rapid increase of the aging population and changes in people's lifestyles.1 It is an ischemic heart disease caused by an imbalance between supply and demand of oxygen in cardiac muscles, as coronary arteries narrow. The onset of this disease can cause fatal results such as premature death.2
Among the risk factors of CAD, there are incurable factors such as sex, past history, family history, and age. On the contrary, there are factors such as smoking, hypertension, obesity, diabetes mellitus, and hyperlipidemia that can be improved with improved diet, physical exercise, and smoking cessation. These efforts are believed to put blood pressure and cholesterol levels under control, reducing risk for CAD and minimizing relapse effectively.3 However, these factors alone cannot explain the reasons behind relapse and prognosis of the disease. Recently, more attention has been focused on the connection between the outbreak of CAD and psychological factors.4
Such psychological factors that might lead to the CAD incidence and mortality include depression, anxiety, aggression, anger, and stress.5 CAD patients often suffer from depression. Depressive symptoms or any past history of major depressive disorder (MDD) could increase CAD incidence and mortality rate.6 Anxiety also shows significant relations with incidence and mortality of CAD. Patients with severe anxiety are more likely to have a relapse after being diagnosed.7 Research done by Pimple et al.8 found that there is a correlation between trait anger and myocardial ischemia.
Those with aggression have a poor temperament and are not willing to trust others. Because the so-called “type A behavior pattern” (TABP) has emerged as a possible risk factor in the development of CAD, research has sought to identify such traits as anger or aggression in CAD patients.910 According to Denollet et al.,11 anger and suppressed anger are related to the development of major cardiac events. Another study by Buckley et al.12 found that intense anger is associated with higher risks for acute coronary occlusion.
Mindfulness-based art therapy (MBAT) is based on Kabat-Zinn's mindfulness meditation13 and reflects on mindfulness-based stress reduction (MBSR), Monti's MBAT14 and the self-regulation theory.15 The critical element in this theory is to equip patients with the ability to cope that can mature the ego harmoniously by subjectively and objectively expressing the physical and psychological pain they face.
This research aimed to understand the treatment effects of MBAT on CAD patients' depression, trait anxiety, anger and anger expression.
METHODS
Subjects
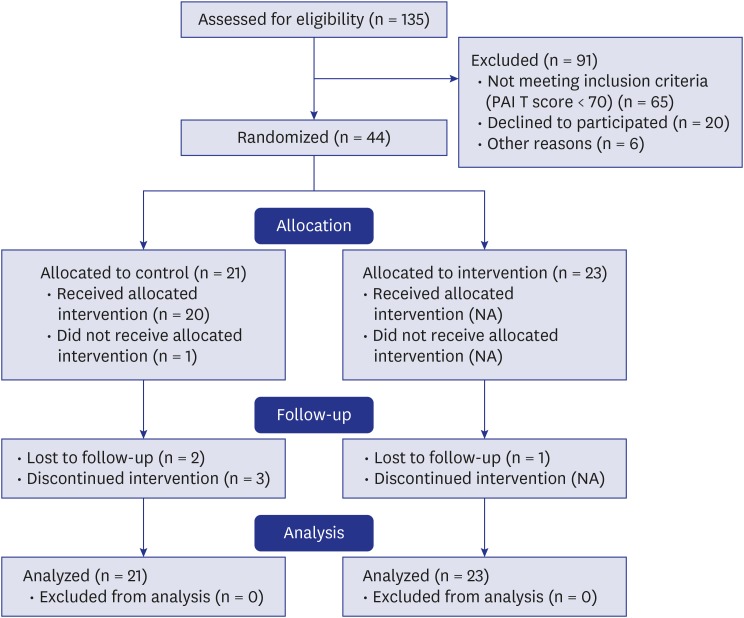
We studied a cohort of 135 CAD patients who were regularly visiting the outpatient clinic and receiving medication at the Wonkwang University Hospital Cardiovascular Center. This research was conducted from March to August 2016. To select subjects who had higher risks of depression, trait anxiety, and anger, we administered the Personality Assessment Inventory (PAI).16 The number of people used in the study was determined by using G*Power program 3.1.4 (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) and the calculated subject when applying α = 0.05, power 80%, and effect size = 0.25 was 135. A total of 70 participants scored over 70 points in the T-scores on the sub-scales measure of depression (DEP), anxiety (ANX), and aggression (AGG). After the 26 subjects were excluded, 44 subjects were split into two groups: 21 belonged to the MBAT group, and 23 to the control group. Before the study, participants were provided detailed explanations regarding study purposes and procedures, based on which they signed research participation agreements indicating consent. Participants were randomly assigned to the MBAT or control group by flipping a coin. As 6 in the MBAT group and 1 in the control group dropped out, only 37 remained as final subjects (Fig. 1).
Treatment and therapists
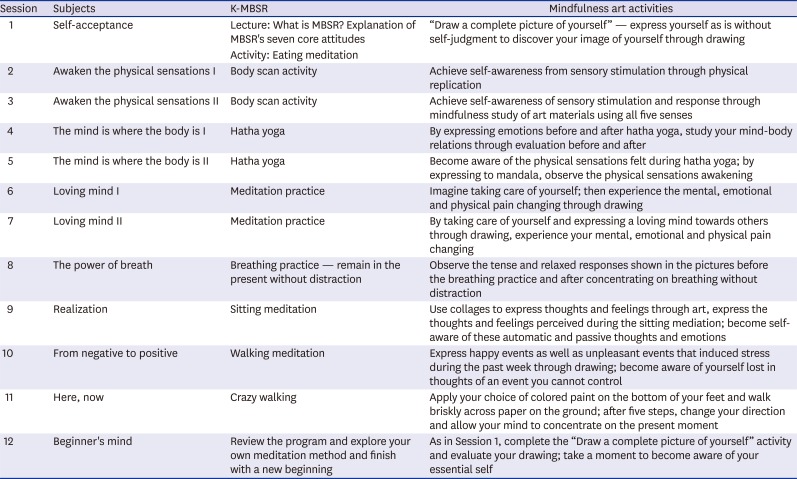
Subjects in the MBAT group received 12 sessions lasting 45 minutes each. Mindfulness-based stress reduction-Korean version (K-MBSR)17 psychological intervention was applied to mindfulness activities. Monti et al.'s13 8-week MBAT program based on MBSR was re-structured with a focus on its progress-by-sessions idea. The MBAT group was divided into A (n = 11) and B (n = 12), and the same type of treatment was given to both of them. The therapist encouraged the patients to express their inner pain or feelings sufficiently. The treatment process is displayed in Table 1. The therapist obtained qualifications from Wonkwang University in 2010 and acquired a doctorate in expressive arts therapy with more than 10 years' experience in the field. The therapist is a specialist in mental health medicine. A senior researcher who is a mindfulness meditation-based group art therapy instructor provided clinical supervision.
Table 1
Stage-wise goals and curriculum of the MBAT intervention
Usual care regimen
During our study, all the subjects in both groups continued to have standard post-treatment clinic care that is directly related with their CAD. However, we asked the subjects in the waitlisted control group not to receive or practice therapies such as meditation, yoga techniques, or interventions similar to MBAT in order to avoid potential contamination as a no treatment group. After the completion of this study, the subjects in the waitlisted control group received the same MBAT intervention as the experimental one.
Measures
Patients used a self-report type evaluation method and evaluated themselves before and after treatment.
State-Trait Anger Expression Inventory (STAXI)
The STAXI provides a self-reported measure of the experience and expression of anger in 44 items.18 Individuals answered on a 4-point Likert scale (“Not at all” to “Almost always”) to assess either the intensity of their angry feelings or the frequency in which anger is experienced, expressed, or controlled.
Beck Depression Inventory (BDI)
The BDI is a 21-item questionnaire designed to assess the degree of depressive symptoms present over a 1-week period.19 Each of the 21 items corresponding to a symptom of depression is summed to give a single score. There is a four-point scale for each item ranging from 0 to 3. Total score of 0–13 is considered minimal range, 14–19 is mild, 20–28 is moderate, and 29–63 is severe. We used the Korean version of the BDI.20
Trait Anxiety Inventory (TAI)
The TAI is a commonly used measure of trait anxiety.21 The TAI defines how one feels in general. It has 20 items for assessing trait anxiety. Trait anxiety items include: “I worry too much over something that really does not matter” and “I am content; I am a steady person.” All items are rated on a 4-point scale (e.g., from “Almost never” to “Almost always”). Higher scores indicate greater anxiety.
Statistical analysis
According to intent-to-treat (ITT) principle, the data for all the subjects were analyzed. Both Student's t-test and χ2 test were used for the analysis of demographic and clinical variables. Repeated measures of analysis of variance (ANOVA) were used to test both interaction and main effects of MBAT between the two groups. All the statistical analyses were conducted by IBM SPSS statistics 21.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Pretest measures
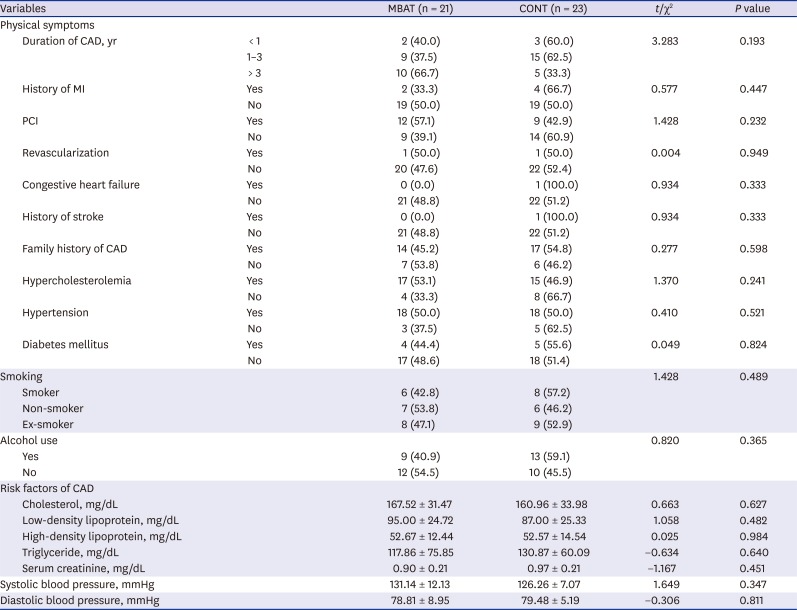
Demographic data and clinical traits are displayed in Tables 2 and 3. There were no significant differences between demographic traits and clinical variables.
Table 2
Demographic characteristics of subjects
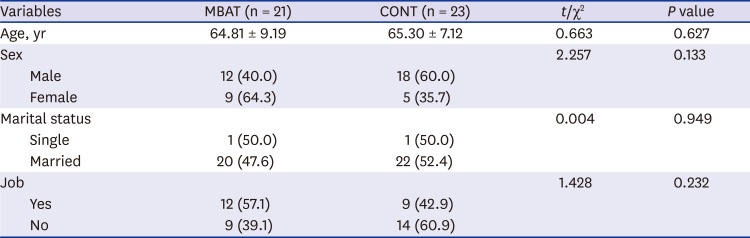
Table 3
Clinical characteristics of subjects
Homogeneity test of psychological variables between MBAT and control group
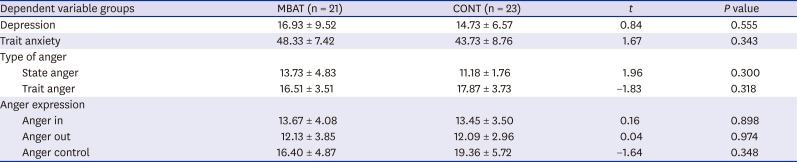
The results showed no significant differences in subjects' psychological characteristics between the MBAT and control groups (Table 4).
Table 4
Homogeneity test of psychological variables between MBAT and control group
Results of comparison for mean difference scores at 12 weeks of MBAT for depression and trait anxiety
The results of outcome measures in MBAT and control groups are shown in Table 5. Both depression and trait anxiety scores showed statistically significant decreases in the MBAT group. Two-way repeated measure ANOVA revealed significant effects for groups (MBAT group vs. control group), time (before and after a single week of the 12 weeks training), and interaction (group × time) in the depression (interaction effect, [F(1,36) = 23.15, P < 0.001]; between group, [F(1,36) = 5.73, P = 0.022]), trait anxiety (interaction effect, [F(1,36) = 13.23, P < 0.001]; between group, [F(1,36) = 4.38, P = 0.043]).
Table 5
Results of comparison for mean difference scores at 12 weeks of MBAT for depression and trait anxiety

Results of comparison for mean difference scores at 12 weeks of MBAT for state anger and trait anger
The results of outcome measures in MBAT and control groups are shown in Table 6. Both state anger and trait anger scores showed statistically significant decreases in the MBAT group. Two-way repeated measure ANOVA revealed significant effects for groups (MBAT group vs. control group), time (before and after a single week of the 12 weeks training), and interaction (group × time) in the state anger (interaction effect, [F(1,36) = 5.60, P = 0.023]), trait anger (interaction effect, [F(1,36) = 6.93, P = 0.012]; within group, [F(1,36) = 4.73, P = 0.036]).
Table 6
Results of comparison for mean difference scores at 12 weeks of MBAT for state anger and trait anger

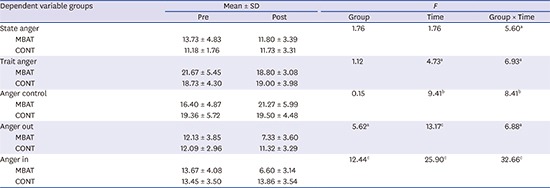
Results of comparison for mean difference scores at 12 weeks of MBAT for anger control, anger out and anger in
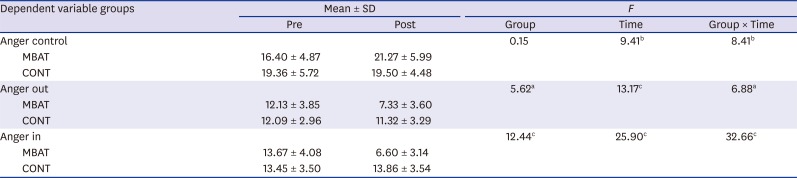
The results of outcome measures in MBAT and control groups are shown in Table 7. Although anger out and anger in decreased, anger control showed a statistically significant increase in the MBAT group. Two-way repeated measure ANOVA revealed significant effects for groups (MBAT group vs. control group), time (before and after a single week of the 12 weeks training), and interaction (group × time) in the anger control (interaction effect, [F(1,36) = 8.41, P = 0.006]; within group, [F(1,36) = 9.41, P = 0.004]), anger out (interaction effect, [F(1,36) = 6.88, P = 0.012]; within group, [F(1,36) = 13.17, P < 0.001]; between groups, [F(1,36) = 5.62, P = 0.023]), and anger in (interaction effect, [F(1,36) = 32.66, P < 0.001]; within group, [F(1,36) = 25.90, P < 0.001]; between groups, [F(1,36) = 12.44, P < 0.001]).
Table 7
Results of comparison for mean difference scores at 12 weeks of MBAT for anger control, anger out and anger in
DISCUSSION
The incidence of CAD rises every year, leading to higher mortality rates. Psychological factors have a significant effect on the progress and prognosis of CAD, and in that sense, proper psychological intervention is required. Our study aimed to investigate the effects of MBAT on reducing depression, anxiety, anger, and anger expression among CAD patients.
The MBAT group showed a significant decrease in depression and trait anxiety. A few other studies found the effectiveness of this therapy in CAD patients as well. Abbott et al.22 found that CAD patients showed reduced depression and perceived stress with the help of MBAT. In a recent study by Nyklíček et al.,23 those who recently experienced percutaneous coronary intervention had their anxiety, depression, and stress levels decreased after receiving MBAT for a short period of time. Parswani et al.24 also found that MBSR training significantly reduced blood pressure and body mass index, both physiological parameters, as well as anxiety, depression, and perceived stress levels in CAD patients. Based on these findings, the MBAT might help improve awareness of the moment, cognitive processes, and information processing by focusing attention on the breath and being in the present moment.25 In addition, this method might allow patients to simply approach their emotions and aim to understand and apply them, rather than driving away unwanted emotions through mindfulness meditation.13 Thus, rather than changing something that exists, mindfulness is a technique that allows people to approach it and understand, experience, and describe it. MBAT also combines traditional, psychological, and relaxation techniques that induce relaxation, which in turn decreases autonomic nervous system (ANS) reactivity.26
This therapy not only helps patients to practice relaxation, but also offers additional measures to help them reach a relaxed state. It induces changes in essential physiological factors that are easily affected by emotions, such as breathing synchrony and heart rate, and also boosts satisfaction among patients through physical integration. Some other studies found that the development of acceptance and self-compassion could produce beneficial outcomes from the positive effects of the therapy on depression and anxiety.27 When patients show minor symptoms of depression, MBAT should be applied as a mental health intervention to prevent it from progressing into major depressive disorder.28
Our study also found that after MBAT, CAD patients saw their state and trait aggression reduce significantly. The therapy was effective in reducing anger expression, particularly anger-control, anger-out, and anger-in. In previous studies, such as Chilvers et al.,29 MBAT improved hostility. Rodriquez et al.30 showed that the therapy might help improve control over trait anger. In a study by Younge et al.,31 mindfulness training had a positive effect on physiological parameters, including exercise capacity and heart rate, and could serve as an effective clinical therapy for heart disease patients. Further, MBAT helps patients with concentration, non-judgment, and acceptance, and also helps them live in the present. It provides a technique that can alter cognition, helping patients see their anger as merely a temporary shift of emotion, not as consequences of certain behaviors. By doing that, the therapy seems to improve patients' self-control. With it, patients can execute a more adaptive response to deal with their anger, rather than approaching it with aggression.
The limitations of this research are that the number of subjects studied is small, and the study was conducted during a limited 12-week period. Second, self-reported surveys were used to make evaluations and it was possible that researcher supervision intervened during the study. Third, probable errors caused by demographic variables, status of CAD, or treatment methods also cannot be excluded. Fourth, the fact that there have been more frequent visits to the MBAT group than the control group may have worked as a bias in judging the treatment effect. Fifth, the study showed higher dropout rates in the control group, and the primary cause for this was found to be the lack of motivation for treatment. This fact could also have triggered a bias in analyzing the treatment effect. Furthermore, as the number of subjects is small, large standard deviations were obtained.
However, this research is significant in that it is the first study to evaluate the effects of MBAT on CAD patients. In addition, previous studies observed patients who had received treatment for a significant period before the study. This research looked at patients who had recently received treatment to verify the effect of MBAT. Lastly, patients were able to learn techniques to adapt to their illness and improve psychological well-being. Future studies will need to observe a larger number of patients to evaluate the effects of MBAT and observe ways to clinically apply MBAT.
 XML Download
XML Download