

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The techniques of radiation therapy (RT) have rapidly progressed in the recent decades. Among the most remarkable techniques is intensity-modulated radiation therapy (IMRT), which uses advanced planning software and the dynamic multileaf collimator to produce a highly conformal plan.1 The superior target conformality of IMRT enables dose escalation to tumor, which results in better tumor control without an increase of treatment-related toxicity.23 Better quality of life and lower treatment-related toxicity were reported among patients who received IMRT than those who received other RT treatment.456789
In Korea, cancer incidence has been increasing in the past 20 years owing to the aging population and the popularization of screening.1011 The use of RT has also increased in terms of both the overall number of treatments and utilization rates.1213 Also, the number of RT facilities have steadily increased over time.14 In addition, the previous report stated that 35% of all institutions were capable to implement IMRT in 2006.15
Concentration of the medical resources in capital areas, where nearly half of the whole national population lives, is an important issue in Korea. A total of 22 out of the 43 advanced general hospitals as well as 52,078 (52.7%) of the 98,878 medical doctors in Korea are in capital areas, including Seoul, Incheon, and Gyeonggi province. The difference in healthcare resources between metropolises and non-metropolitan areas is also significant, with 73,933 (74.8%) of the 98,878 doctors in Korea working in the capital area and regional metropolises.16
Thus, in this paper, we aimed to assess the temporal changes of RT according to specific RT modality in Korea. In addition, the IMRT utilization rate as the main index in determining accessibility to advanced RT was examined by geographical region, classified into the capital area vs. non-capital areas and metropolitan areas vs. non-metropolitan areas.
METHODS
Sources of data and data acquisition
The Korean government has operated the National Health Insurance Service (NHIS) for over 30 years, which covers more than 98% of the nation's population.17 The Korean Health and Insurance Review and Assessment Service (HIRA) has provided information on the medical activities based on NHIS claim and reimbursement records.18 We collected information from 2010 to 2016 using treatment codes representing the first planning of RT. Based on the treatment codes, we acquired information regarding the number of RT modalities used. Treatment codes with an average number of use of < 20 per year were excluded from the study. We classified the treatment codes into the following treatment categories: two-dimensional radiotherapy (2DRT), three-dimensional conformal radiotherapy (3DCRT), stereotactic radiotherapy (SRT), proton therapy (PRT), brachytherapy, and IMRT. SRT included both stereotactic body radiotherapy and stereotactic radiosurgery. The details of the classification codes of treatment types are described in Table 1. Because the NHIS had not covered IMRT and PRT before 2011, the number of patients who received IMRT and PRT before 2011 was not calculated in the NHIS database. In addition, information on the regions of each institution that performed the treatments of each code was acquired.
Table 1
Categorization of RT codes
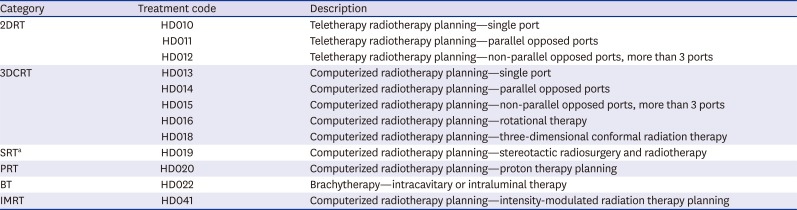
HD017 (computerized radiotherapy planning intraoperative radiation therapy), HD021 (brachytherapy-mold therapy), and HD023 (brachytherapy-interstitial therapy) were excluded because their average number of use was < 20 per year.
RT = radiation therapy, 2DRT = two-dimensional radiation therapy, 3DCRT = three-dimensional conformal radiation therapy, SRT = stereotactic radiotherapy, PRT = proton therapy, BT = brachytherapy, IMRT = intensity-modulated radiation therapy.
aSRT included both stereotactic body radiotherapy and stereotactic radiosurgery.
Classification of locating regions
The capital area included Seoul, which is the capital city of Korea, Incheon, and Gyeonggi province, which are easily accessible and surrounding to Seoul. Metropolitan areas encompassed seven administered metropolises and a province; Seoul, Daegu, Daejeon, Gwangju, Busan, Incheon, Ulsan, and Gyeonggi province. Gyeonggi province was categorized as metropolitan area because it is highly urbanized as metropolis with population of > 10 million and population density of > 1,100 per km2.19
Statistical analysis
To evaluate the temporal changes according to specific types of RT use, we performed a Poisson regression analysis. The calculated amount of annual rate changes in specific type of RT was defined as annual increase estimate (AIE) and considered statistically significant with a P value of < 0.05. The differences of AIEs between capital and non-capital areas and metropolitan and non-metropolitan areas were also analyzed. All statistical analyses were performed via SPSS version 20.0 (IBM Inc., New York, NY, USA).
RESULTS
Distribution of RT from 2010 to 2016 according to specific modalities
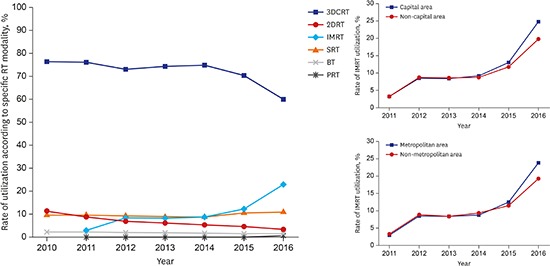
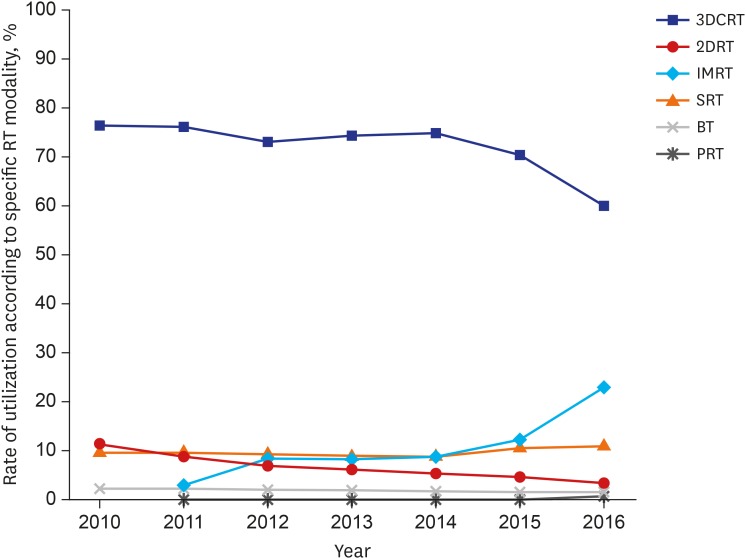
A total of 480,417 patients received RT from 2010 to 2016. The numbers of patients treated with various RT modalities in each year were listed in Table 2. The most dominant RT modality used during the past 7 years was 3DCRT (72%), although the rate of utilization showed a decreasing trend. However, the rate of IMRT utilization showed a steady increase since 2011, making it the second most common RT modality used. The utilization of 2DRT and 3DCRT showed an annual decreasing trend. The AIE of 2DRT and 3DCRT from 2010 to 2016 was −17.0% (95% confidence interval [CI], −16.5 to −17.5; P < 0.001) and −3.1% (95% CI, −2.9 to −3.3; P < 0.001), respectively. Meanwhile, the utilization of IMRT and SRT increased per year, with the AIE of IMRT and SRT being 37.9% (95% CI, 37.1 to 38.7; P < 0.001) and 2.2% (95% CI, 1.7 to 2.7; P < 0.001) from 2010 to 2016, respectively. Fig. 1 shows the change in the rate of RT utilization according to specific RT modalities from 2010 to 2016. In particular, the rate of IMRT utilization had two sharply rising periods, that is, between 2011 and 2012 and between 2015 and 2016. By contrast, the rate of 3DCRT utilization showed a relative abrupt reduction during both periods.
Table 2
Distribution of RT in Korea from 2010 to 2016 according to specific modalities
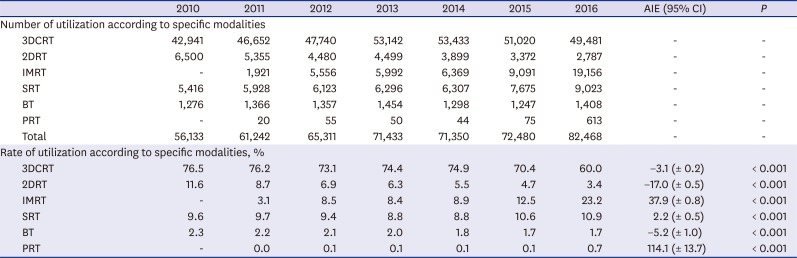
Fig. 1
Rate of RT utilization from 2010 to 2016 according to specific RT modalities.
RT = radiation therapy, 3DCRT = three-dimensional conformal radiation therapy, 2DRT = two-dimensional radiation therapy, IMRT = intensity-modulated radiation therapy, SRT = stereotactic radiotherapy, BT = brachytherapy, PRT = proton therapy.
IMRT utilization between the capital and non-capital areas from 2010 to 2016
RT utilization in both the capital and non-capital areas is shown in Table 3. A total of 67% (321,734/480,417) of RTs was performed in the capital area. The proportion of RT utilization in the capital area during the past 7 years ranged from 66% to 68%. In terms of IMRT utilization, a steady increasing trend (P < 0.001, Fig. 2A) was noted from 2010 to 2016, in both capital and non-capital areas. Considering AIE from 2010 to 2016 between the capital and non-capital areas, the rate of AIE in the capital area was higher than that in non-capital areas (40.7% vs. 31.9%; P < 0.001).
Table 3
Comparison of RT utilization between capital and non-capital areas

Proton therapy was performed in the capital area only.
RT = radiation therapy, AIE = annual increase estimate, CI = confidence interval, 3DCRT = three-dimensional conformal radiation therapy, 2DRT = two-dimensional radiation therapy, IMRT = intensity-modulated radiation therapy, SRT = stereotactic radiotherapy, BT = brachytherapy.

IMRT utilization between metropolitan and non-metropolitan areas from 2010 to 2016
Table 4 shows the comparison of RT modality utilization between the metropolitan and non-metropolitan areas. A total of 86% (410,771/480,417) of RTs was performed in the metropolitan areas. The proportion of RT utilization in the metropolitan areas was consistent per year, ranging from 85% to 86%. With respect to IMRT utilization, increasing patterns were observed in both metropolitan and non-metropolitan areas (P < 0.001, Fig. 2B), which is similar to the results for comparison of RT utilization between capital and non-capital areas. The metropolitan areas showed a higher AIE of IMRT use than non-metropolitan areas (39.7% vs. 29.4%; P < 0.001).
Table 4
Comparison of RT utilization between metropolitan and non-metropolitan areas
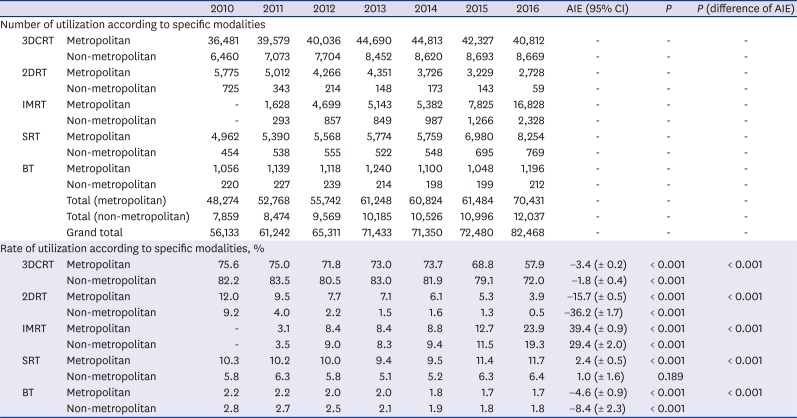
Proton therapy was performed in the metropolitan area only.
RT = radiation therapy, AIE = annual increase estimate, CI = confidence interval, 3DCRT = three-dimensional conformal radiation therapy, 2DRT = two-dimensional radiation therapy, IMRT = intensity-modulated radiation therapy, SRT = stereotactic radiotherapy, BT = brachytherapy.
DISCUSSION
This survey assessed the utilization of RT, specifically IMRT, and its comparison between regional areas with socioeconomic differences. In our analysis of IMRT utilization in Korea from 2010 to 2016, an increasing trend of IMRT use was predominant. Presently, advances in RT techniques have significantly altered the RT implementation landscape.202122 The benefits of IMRT, such as reducing toxicity, maximizing quality of life, and maintaining disease control,168920 contributed to the change in RT practice.
We observed that the utilization of IMRT showed a steady increase from 2012 to 2015, with an abrupt increase from 2011 to 2012 and from 2015 to 2016. In particular, IMRT utilization in Korea increased by an average rate of 1.3% between 2012 and 2015, by 5.4% from 2011 to 2012, and by 10.7% from 2015 to 2016. In 2011, the Korean NHIS announced that the national insurance will cover IMRT for patients with head and neck cancer, prostate cancer, brain tumor, spinal tumor, and recurrent or persistent tumors previously treated with RT. Thereafter, in 2016, NHIS announced subsequently that the national insurance on IMRT will cover all tumors if IMRT was implemented to spare an organ at risk or to reduce irradiated dose to normal organ. As such, the remarkable growth of IMRT use at both periods was associated with the extension of the national insurance for IMRT utilization by the NHIS.
Notably, the increasing pattern of IMRT use has been found in all institutions across Korea, regardless of the geographical region that encompasses and socioeconomic differences. As previously mentioned, the Korean NHIS covers more than 98% of the population.18 It facilitates patient access to advanced medical care by reducing the economic burden and leads to the implementation of advanced medical treatment in each institution.2123 Korea's universal healthcare system has lowered the socioeconomic barriers to advanced medical services, such as IMRT. However, in the current survey, a difference was noted in the increasing degree of IMRT utilization. The capital and the metropolitan areas had higher AIE of IMRT utilization than non-capital areas and non-metropolitan areas (40.7% vs. 31.9% and 39.7% vs. 29.4%, respectively). These differences were associated with both the concentration of medical institutions and the movement of patients who have advanced disease and are candidates for recent treatment from non-capital areas or non-metropolitan areas to urban areas depending on their willingness, rather than inadequate access to advanced medical care.1524
The increase in use of IMRT is a global trend. Mell et al.25 reported that only 32% of radiation oncologists in the United States used IMRT in 2002, whereas 73.2% used IMRT in 2004.26 In the United Kingdom, 45.8% of radiation oncology centers performed IMRT in 200727 and 76% in 2010.28 In Canada, only 37% of radiation oncology centers implemented IMRT in 2006, whereas 72% of these centers performed IMRT for all patients who could benefit from the treatment in 2010.29 In our study, the rate of IMRT use in Korea has steadily increased, but it was only 23.2% in 2016, which is still lower than the rates in the abovementioned countries. This suggests that the treatment efficiency of RT can be improved with continuous increase of IMRT treatment in Korea.
Our study has several limitations. Because the claims and reimbursement records from the HIRA include only the insured treatment, uninsured cases, including uninsured benign disease or RT for foreign patients, cannot be analyzed. Thus, the total number of RT utilization in this survey might be smaller than the actual number of implemented treatment. Moreover, we assumed that the use of IMRT can be an indicator of the accessibility of advanced medical care because possession of the equipment capable of IMRT is directly connected to the socioeconomic burden of each institution. Therefore, we hypothesized that IMRT implementation implied a strong commitment to perform recent treatments. However, we also agree that this hypothesis has its limitations because it was strongly related to the viewpoint of radiation oncologists.
In conclusion, the number of patients who received IMRT in Korea has shown a steady increase in the past 6 years. Furthermore, the increasing trend of IMRT utilization had the same patterns regardless of geographical region with political and socioeconomic difference, although the rate of increase varied. Regarding the increase of IMRT utilization being a global trend, this survey detailed the status of IMRT implementation and showed that IMRT has become one of the most common RT modalities for cancer treatment in Korea.
 XML Download
XML Download