

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Distal radius fractures (DRFs) are one of the most common fractures not only among adults but also among children and adolescents.12 More than 640,000 cases of DRFs are reported annually in the United States,3 and almost 71,000 cases are reported in the British adult population.4 The high incidence of DRF causes a substantial economic burden and other social problems including decreased school attendance, lost work hours, loss of independence, and lasting disability.5 Therefore, DRF prevention is important, and it is essential to understand the epidemiology of DRFs to achieve this.
Since most DRFs are caused by low-energy trauma, such as a fall from a standing height,6 slippery weather conditions may cause fracture epidemics.7 Thus, the incidence of DRF, which shows a clear seasonal variation, is known to increase in winter.89 However, most previous epidemiological studies of the incidence and seasonal variation of DRFs have been confined to European countries and North America.710 Few studies have examined seasonal variation in DRFs in Asia.11 Lee et al.12 reported seasonal variations in DRF incidence in Korea; however, their study had some limitations; it had a short-term study period and was conducted in a single center.
Thus, our aim in the present study was to examine the incidence and seasonal variation of DRFs in Korea based on an analysis of nationwide data acquired from the Korean Health Insurance Review and Assessment Service (HIRA).
METHODS
Data source
The authors analyzed nationwide data obtained from the HIRA from 2011 to 2015. In Korea, 97% of the entire population is legally obligated to enroll in the National Health Insurance (NHI) program. Patients only pay about 30% of the total medical cost to healthcare institutions, and all healthcare providers submit claims data for inpatient and outpatient management, including diagnostic codes, which are classified according to the International Classification of Diseases, 10th revision (ICD-10), procedure codes, prescription records, demographic information, and direct medical costs to the HIRA to request reimbursement for the remaining 70% of the medical cost from the NHI service. Of the remaining 3% of the population not registered in the NHI program, excluding illegal residents, most receive healthcare coverage through the Medical Aid Program. The claims data for patients covered by the Medical Aid Program are also reviewed by the HIRA. Hence, the medical records of almost all newly admitted or hospitalized patients in healthcare institutions in Korea are prospectively recorded by the HIRA.
Data collection
The authors used ICD-10 codes and procedure codes to identify patients of all ages with newly diagnosed DRFs in Korea between 2011 and 2015 (Table 1). Although HIRA data provide patient identifiers, if a patient with a DRF makes multiple visits to a healthcare institution, claims data for the number of visits are generated. To avoid the risk of multiple counting, the authors used a previously reported method,13 as follows. First, patients with surgically treated DRFs were identified with ICD-10 codes (S52.5 and S52.6) and operation codes (N0603, N0613, N0607, N0617, N0993, N0994, and N0983) (Table 1). Each operation code was counted as a single case. However, percutaneous pinning and external fixation are often performed simultaneously. Therefore, if a patient received the two operations on the same day, they were considered to be performed on a single DRF. The same criterion was applied when a patient received open reduction with internal fixation and external fixation on the same day. Subsequently, in order to identify patients with DRFs who received conservative treatment, those who underwent surgical treatment were excluded from the HIRA data using patient identifiers, and those with splint or cast codes (T6020, T6030, T6151, and T6152) for DRF ICD-10 codes (S52.5 and S52.6) were included (Table 1). For conservative treatment, multiple splint or cast codes are commonly entered for a single case of DRF because an initially applied splint can be substituted by a cast at a later stage, or a long-arm cast can be changed to a short-arm cast, etc. For this reason, additional codes entered after a period of 6 months following the initial entry of splint or cast codes were recounted.14
Table 1
ICD-10 diagnosis codes and procedure codes of distal radius fractures

We examined patient data to identify the year and month in which the fracture occurred, and the patient's age and sex. We first counted the number of DRFs for each year and then calculated age-adjusted and sex-specific incidence rates per 100,000 persons with DRFs using the 2010 United States population as the standard population. Estimated year-specific, age-specific, and sex-specific populations in Korea were obtained from the “Statistics Korea” website (http://www.kosis.kr). Patients were divided into groups according to age (5-year intervals), and then the incidence of DRFs per age group per study year was calculated according to the population of each age group in Korea for a given study year (per 100,000 persons).
We divided the year into 4 seasons to examine the seasonal variation in the incidence of DRFs; March through May was defined as spring, June through August as summer, September through November as autumn, and December through February as winter. Seasonal variations in the incidence of DRFs were examined according to year and age group (15-year intervals). Lastly, the relationship between the monthly incidence of DRFs and the monthly national average temperature in Korea during winter was investigated.
Statistical analysis
The annual percentage changes in the age-adjusted incidence rate of DRFs were calculated from 2011 to 2015 using joinpoint regression analysis (Joinpoint Regression Program, version 4.3.1.0; National Cancer Institute, Bethesda, MD, USA). All other data sets were analyzed using SAS statistical software version 9.13 (SAS Institute, Cary, NC, USA). Univariate analysis was conducted using the t-test. The correlation between the monthly number of DRFs and the national monthly mean temperatures in winter (https://data.kma.go.kr) was analyzed using the Spearman rank test. Values of P < 0.05 were considered significant.
RESULTS
A total of 647,655 DRFs (621,451 patients) occurred from 2011 to 2015; thus, an average of about 130,000 DRFs occurred annually in Korea. Of these, 259,453 cases (249,457 patients) involved male patients, and 388,202 cases (371,994 patients) involved female patients, with a male to female ratio of 1.50. The mean age of patients with DRFs was 47.2 years (standard deviation [SD] ± 25.5). The mean age of men was 30.2 years (SD ± 23.2), while that of women was significantly higher at 58.6 years (SD ± 20.2, P < 0.001). The total number of DRFs increased from 2011 to 2013 (128,000 and 137,054, respectively), and then decreased after 2013 (129,687 in 2014 and 116,750 in 2015) (Table 2). The age-adjusted incidence rate per 100,000 persons increased between 2011 and 2012 (278.0 and 291.7, respectively), and then decreased after 2012 (288.33 in 2013 and 246.00 in 2015) (Fig. 1, Table 2). The annual percentage change in the age-adjusted rate for 5 years was calculated as −2.9% (95% confidence interval [CI], −8.2%–2.6%), which was not statistically significant (P = 0.190).
Table 2
Number of cases and age-adjusted rates of distal radius fractures from 2011 to 2015

Fig. 1
Age-adjusted and sex-specific rate of distal radius fractures per 100,000 persons in Korea from 2011 to 2015.
The 5-year age group-specific number of DRFs from 2011 to 2015 was highest in the 10 to 14-year-old age group (124,591 cases, 19%), followed by the 55 to 59-year-old age group (70,978 cases, 11%), and the 60 to 64 year-old age group (61,608 cases, 10%) (Fig. 2). Among those under 45-year-old, the incidence was higher in male than in female individuals; in particular, boys accounted for 82% (101,796 cases) of DRF cases in the 10 to 14-year-old age group. The age group of 45-year-old women had a higher incidence of DRFs than their male counterparts, and 82% (317,687 DRFs) of 387,607 DRFs in persons over 50 years occurred in the female population (Fig. 2, Table 3). The incidence rate per 100,000 persons by age group peaked in the 10 to 14-year-old age group, then decreased, and increased again as they aged (Fig. 3A). In the female population, the annual incidence rate per 100,000 persons was highest in the 70 to 79-year-old age group, while the 10 to 14-year-old age group showed the highest incidence rate in the male population (Fig. 3B and C).
Table 3
Number of distal radius fractures divided by the age of 50 from 2011 to 2015

Fig. 3
Incidence rate of distal radius fractures per 100,000 persons, by age group — (A) Total population, (B) Men, and (C) Women.

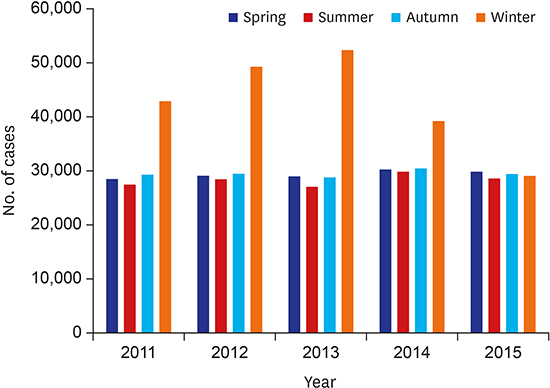
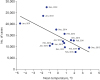
During the study period, the number of DRFs was highest in winter (33%), followed by autumn (23%), spring (23%), and summer (22%) (Table 4). The annual change in the number of DRFs in winter was more prominent than in other seasons (Fig. 4, Table 4). While the incidence proportion of DRFs in children, adolescents and young men under 30-year-old peaked during spring, females over 15-year-old and men over 30-year-old had the highest incidence proportion during winter (Fig. 5). During the study period, the highest mean monthly number of DRFs occurred in January (15,722 cases, 12%), followed by December (15,508 cases, 12%), and February (11,321 cases, 9%) (Fig. 6). As the national monthly mean winter temperature increased, the monthly number of DRFs tended to decrease, and the correlation was significant (P = 0.003, r = −0.704) (Fig. 7).
Table 4
Seasonal variation of number of distal radius fractures from 2011 to 2015

Fig. 4
Seasonal variation in the incidence of distal radius fractures by year in the total population.


DISCUSSION
An average of 130,000 cases of DRFs occurred annually from 2011 to 2015 in Korea. The annual age-adjusted incidence rate per 100,000 persons was between 240 and 300, but no statistically significant annual change was observed. The incidence of DRFs in males was highest in children and adolescents, while in females it was highest in those in their 70s. Further, females showed a markedly increased DRF incidence after the age of 50 years. DRFs reached peak incidence during winter. However, the annual incidence of DRFs occurring in winter greatly varied compared with that occurring in other seasons and correlated with the average temperature during the winter season. Children, adolescents and young men under 30-year-old had a peak incidence proportion of DRFs during spring, and females over 15-year-old and males over 30-year-old had the highest incidence proportion of DRFs during winter.
In studies using national claims data, the number of DRFs may vary slightly from study to study depending on their assessment methods.1415 Kwon et al.14 examined the DRF incidence and related mortality in patients aged ≥ 50 years with between 2008 and 2012, and reported 65,654 and 74,720 DRFs in 2011 and 2012, respectively. In our study, however, the numbers of DRFs in patients aged ≥ 50 years were 72,890 and 81,694 in 2011 and 2012 respectively, and higher than those of the previous study (Table 3). We considered conservatively-treated patients with multiple procedure codes for splints or casts within 6 months as a single DRF, similar to the method used by Kwon et al.14 However, patients who received two operations were counted as two DRFs, assuming that they had bilateral DRFs. If the primary surgery was not successful, the patients needed reoperation. In our study, if reoperation was performed, we counted these cases as 2 DRFs. Our method has the potential for overestimating the number of DRFs, but we consider these are very rare cases. Thus, the method we used to assess the number of DRFs produced slightly different results than those reported by the previous study, but this difference was less than 10%.14
In our study, the incidence rates of DRFs in children and adolescents between 10 and 14 years of age were high, especially in the males, similar to those of previous studies.16 The cause of a peak incidence rate is known to have a correlation with pubertal growth spurt;17 the process of bone mineralization cannot keep up with the abrupt increase in new bone development, resulting in bones that are particularly susceptible to fracture. It is known that physical activities among these age groups are vigorous18 and most pediatric forearm fractures are reported to correlate with playing or sports activities.1920 In particular, the incidence proportion of the DRFs in children and adolescents was previously reported to be high in spring.1921 This observation is consistent with our study that children, adolescents and males younger than 30-year-old engaging in vigorous physical activities showed a high incidence proportion of DRFs in spring. Such results are considered due in part to the nature of spring season being appropriate for playing and sports activities with better weather conditions.
We also found that the incidence rate of DRFs notably increased in individuals over 50 years of age, particularly in women, which was similar to the findings of previous studies.422 The incidence of DRFs increased in older women due to various risk factors, including decreased bone mineral density (BMD), low vitamin D levels, and postural balance decline.232425 Postural balance decline in older women is associated with a decrease in lower limb strength, sensory system function (vision, vestibular, and proprioception), and flexibility.26 Fu et al.27 reported that sedentary women aged 40 to 60 years improved postural stability through a balance training program. However, the importance of such balance training is often overlooked compared to BMD evaluation.23 The prevention of osteoporosis and balance decline is needed to reduce the incidence of DRFs in women 50-year-old and older.
Several previous studies in Europe and North America have confirmed that the incidence of DRFs increases in the winter, and this pattern is reported to be associated with snowy and icy conditions.7810 However, in East Asia, including China, Japan, and Korea, there have been few studies investigating the seasonal variation in the incidence of DRFs. The marked decrease in temperature during winter in East Asia is accompanied by widespread inflows of cold continental air, called cold surges or cold waves.28 A cold surge is one of the most important characteristic weather phenomena of the East Asian winter monsoon on synoptic time scales.29 Therefore, seasonal variations in the incidence of DRFs may occur due to such seasonal characteristics in East Asia. All age groups, excluding those usually associated with high-level physical activities, showed a high incidence proportion of DRF during winter.
Bischoff-Ferrari et al.9 reported that higher winter temperatures were inversely related to the risk for DRFs. In this study, the incidence of DRFs tended to decrease as the national mean temperature in winter increased. Such effects from weather conditions resulted in annual variations of the DRF incidence rate in winter. During winter, when under an intense cold surge, proper maintenance of roads is necessary in order to reduce the incidence of DRFs.
Although this study employed a large sample size, based on a nationwide database, it also has some limitations. First, the correlation between the incidence of DRFs and snowfall could not be analyzed. Although the Korean Meteorological Administration (https://data.kma.go.kr) provides precipitation data, which covers both rainfall and snowfall, it does not distinguish between these 2 parameters. Thus, we could not analyze the correlation between the incidence of DRFs and snowfall. Second, since the HIRA data did not provide the cause of injury, an analysis on the injury mechanism was not available. Third, primary surgery and reoperations could not be distinguished in the coding system. As such, when 2 operation codes were entered for a single patient, it was assumed that the second operation code was entered for the opposite side, rather than for reoperation. With this method, the patients with reoperation were counted as two DRFs, and thus the number of DRFs may have been overestimated. Finally, there is the possibility of some code errors in such a large database.
In conclusion, the annual incidence of DRF was 130,000 in Korea. Children, adolescents, and men under 30-year-old had a high incidence of DRFs in spring. However, the incidence in females over 15-year-old and men over 30-year-old was highest in winter. The incidence of DRFs in winter varied notably from year to year. In winter, the DRF incidence increased under an intense cold surge. Active preventive measures are essential, especially in women 50 years or older given the high DRF incidence in this group.
 XML Download
XML Download