

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Recently, atypical femoral fracture (AFF) appeared as a matter of issue after a long-term use of bisphosphonate.1234 AFFs are commonly associated with non-union and fixation failure, which require repeated operations.56
AFF differs from typical osteoporotic femoral fractures: femoral neck and intertrochanteric fractures, because the radiologic features of AFF are closely akin to stress fracture.7 A task force of the American Society for Bone and Mineral Research (ASBMR) defined AFF as a fracture that exhibits features of a stress fracture with localized periosteal or endosteal thickening of the lateral cortex (flaring or beak at the lateral cortex).1
Based on several epidemiologic studies, the incidence rate of AFF varies from 76 to 310 per 100,000 person-years.8910 However, in these studies, International Classification of Diseases (ICD) code system was used to identify AFF, instead of radiologic definition of ASBMR. The evaluation based on ICD code system might not be determine the exact occurrence of AFF, because that system could not distinguish between an ordinary femoral fracture and an AFF without radiological review, resulting in a detection bias.24 To determine the exact incidence rate of AFF, a radiologic review is mandatory.
In East Asia, the population is aging, and osteoporosis and osteoporotic fractures are prevalent.1112 Aged populations have been widely treated with bisphosphonates.1314 Accordingly, AFF after the use of bisphosphonate is a growing concern in East Asia.3413 To balance the risk-benefit of the bisphosphonate use, baseline data about the incidence rate of AFF is necessary. However, there have been no reports on the incidence rate of radiologically defined AFF in East Asian patients after the use of bisphosphonate.
The purpose of this study was to estimate the incidence rate of radiologically diagnosed AFF in Korean patients who took bisphosphonates, and to determine the relationship between the AFF occurrence and the duration of bisphosphonate use.
METHODS
Study population
This study was conducted as a hospital-based retrospective study to estimate the incidence rate of AFF among patients who received bisphosphonate in Seoul National University Bundang Hospital (SNUBH), a tertiary referral hospital in Korea. The data for this retrospective analysis were collected from electronic medical records (EMRs) stored in the SNUBH Clinical Data Warehouse (CDW), which integrates clinical data from hospital information systems (HISs).15
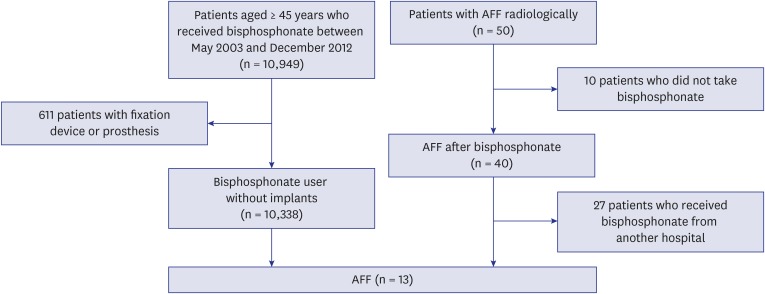
Using the CDW, we identified patients, who had any history of bisphosphonate treatment from May 2003 to December 2012. Among them, we selected 10,949 patients, who were older than 45 years at the time to start bisphosphonate treatment.4 We excluded 611 patients, who had femoral surgeries including internal fixation and hip arthroplasty before the bisphosphonates treatment to avoid potential bias. Finally, 10,338 patients, who met the criteria, were subjects of this study (Fig. 1).
Fig. 1
Flow-chart to identify the patients with AFF after bisphosphonate use.
AFF = atypical femoral fracture.
We collected information on age, sex, body mass index (BMI), and the duration of bisphosphonate use. The duration was determined using the length of each prescription based on pills dispensed and dosing interval, allowing for a gap of up to 60 days between prescription and refill to determine a continuous exposure interval.16
There were 9,238 women and 1,100 men with a mean age of 68.1 years (range, 45–99 years) at the start of bisphosphonate treatment. Their mean BMI was 23.5 kg/m2 (range, 12.2–45.2 kg/m2).
Radiological detection of AFF
We captured 300 subtrochanteric or diaphyseal fractures of the femur from CDW, which were diagnosed from May 2003 to December 2012, using ICD-10 code of S722 (subtrochanteric fracture) and S723 (femoral shaft fracture). After then, radiographs of these 300 fractures were reviewed by two orthopedic surgeons, who had 9 and 27 years of experience as orthopaedic surgeon. The reviewers were blinded to the information about the bisphosphonate use. A diagnosis of AFF was made according to the radiographic criteria by the ASBMR taskforce1; 1) location anywhere along the femur from just distal to the lesser trochanter to just proximal to the supracondylar flare, 2) a transverse fracture line at the point of origination in the lateral cortex (the orientation of fracture line may become oblique), 3) non-comminuted or minimally comminuted, and 4) localized periosteal or endosteal thickening of the lateral cortex at the fracture site (beaking or flaring). When both of the two agreed, a diagnosis of AFF was made.
In AFF patients, we counted the duration of bisphosphonate treatment until the fracture.4 If a patient had multiple or bilateral AFFs during the study period, we counted the duration of bisphosphonate use until the diagnosis of the first AFF.
Statistical analysis
Descriptive statistics was presented as mean and standard deviation or as counts and proportions.
Incidence rates were defined as the number of new AFF per 100,000 person-years. The denominator is the sum of the person-time of the at risk population. It was determined as actual time a patient contributed to the study, from the first date the patient received bisphosphonate to the last day of prescription of bisphosphonate or to the date diagnosed as fracture.
To compare the incidence rate of the AFF between Korea and other geographic areas, age-adjusted incidence rate was calculated using U.S. 2010 Census data. The 95% confidence intervals (CIs) for the incidence rates were estimated using the Fay-Feuer method for gamma-based central CIs for directly standardized rates.17
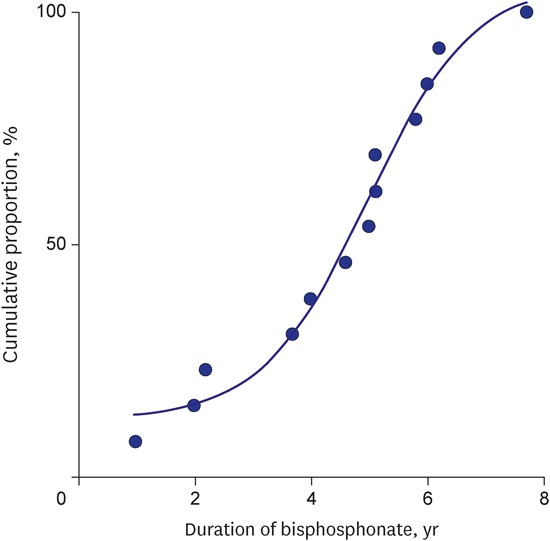
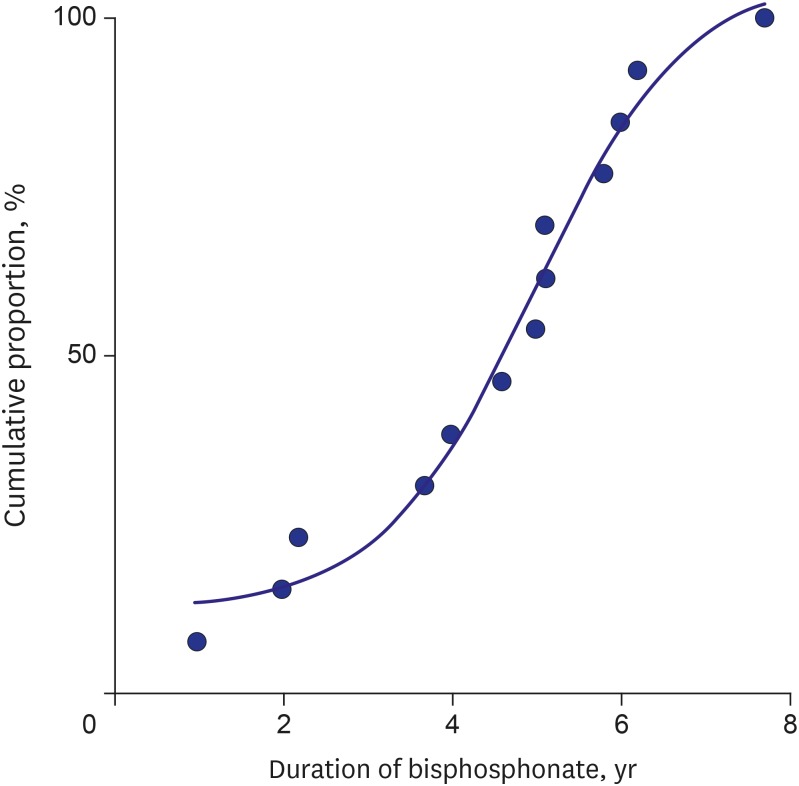
We performed Poisson regression analysis to estimate the association between duration of bisphosphonate use and AFF. And, we plotted the cumulative proportion of AFF for each duration of bisphosphonate use. Statistical analyses were carried out with SPSS version 16.0 (SPSS Inc., Chicago, IL, USA) and STATA version 14 (StataCorp, College Station, TX, USA).
RESULTS
During the study period, 50 patients were diagnosed as having an AFF. Among them, 10 patients did not have history of bisphosphonate use before the diagnosis, and 27 patients received bisphosphonate treatment at other hospitals. Among 10,338 individual patients, who had a history of at least one filled prescription for an oral or intravenous bisphosphonate in our hospital, the remaining 13 patients developed AFF (Fig. 1). The incidence rate for an atypical fracture was 85.9/100,000 person-years (95% CI, 50.2–146.9), and age-adjusted incidence rate was 72.7/100,000 person-years (95% CI, 29.1–175.8).
Thirteen AFF patients included 12 women and one man. Their mean age was 65.8 years (range, 52–77 years) and the mean BMI was 25.1 (range, 20.6–29.3 kg/m2). The mean duration of bisphosphonate use in AFF patients was longer (4.5 ± 1.9 years) than that (1.5 ± 2.0 years) in non-AFF patients (Table 1). In 7 patients (53.8%, 7/13), bilateral AFF occurred during the study. Among the 20 AFFs in the 13 patients, 55% (11/20) occurred at the subtrochanteric area, and 45% (9/20) at diaphyseal fractures.
Table 1
Comparison between patients with AFF and without AFF
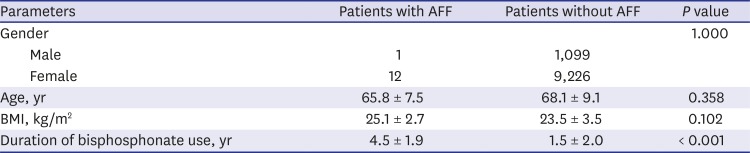
In Poisson regression analysis, higher BMI was associated with an increased risk of AFF (relative risk, 1.2; 95% CI, 1.004–1.359). The risk of AFF increased 2.1 folds per 1 year incremental of bisphosphonates use, although it was not statistically significant (95% CI, 0.704–6.355) (Table 2). The cumulative proportion of AFF increased abruptly when the duration of bisphosphonate use was 4 years or more (Fig. 2).

DISCUSSION
This is the first study on the incidence rate of AFF after the use of bisphosphonate from East Asia. We found that the incidence rate was 85.9/100,000 person-years in Korean patients who was older than 45 years. Higher BMI was associated with occurrence of AFF. Regarding use of bisphosphonate, longer duration of bisphosphonate use was associated with occurrence of AFF with marginal significance.
Previous studies reported different incidences of AFF, because the occurrence of AFF varies according to the study design (retrospective vs. prospective), inclusion criteria for cut-off of age, population at risk (among bisphosphonate users vs. patients with fractures), method identifying AFF (ICD-10 codes vs. radiograph by ASBMR criteria), and statistical method (cumulative incidence vs. incidence rate).34181920212223242526
Many studies have used ICD code system to identify AFF, which it might lead to overestimate the occurrence of AFF, because ICD code system did not distinguish between atypical and ordinary features of fracture.8910 Even in studies using radiographic criteria for diagnosis of AFF, it should be considered which criteria were used to identify AFF, because differences in radiographic criteria might result in different occurrence of AFF.126
In terms of statistical method, many studies on AFF evaluated cumulative incidence to estimate the occurrence of AFF.181922232425 However, the duration of bisphosphonate use should be considered in order to determine the exact amount of occurrence of AFF in population at risk, because the duration is a well-known risk factor.24 The occurrence of AFF should be analyzed by using the incidence rate (per person-time), instead of cumulative incidence (per person). Incidence rate is the number of new cases per population at risk in a given time period (per person-years), and cumulative incidence is the number of new cases within a specified time period divided by the size of the population initially at risk (per person). We evaluated the age-adjusted incidence rate of AFF, which allowed comparing the occurrence of AFF in Korea with those of other countries.
The incidence rate of AFF in East Asian populations has been considered to be higher than those in western populations.41627 Anatomical variation such as more anterolateral bowing of the femur in East Asian population has been reported to be a possible explanation for the higher risk of AFF in that population.27282930 However, our results showed that the incidence rate of AFF in East Asian was comparable with those of western population (Table 3).4202131
Table 3
Incidence rate (/100,000 person-years) of AFF identified radiologically after bisphosphonate use

| Authors | Country | Study period | Age, yr | No. of subjects | AFF | Incidence rate, % |
|---|---|---|---|---|---|---|
| Schilcher and Aspenberg21 | Sweden | 2005–2008 | ≥ 55 | 3,087 | 5 | 100.0a |
| Tamminen et al.20 | Finland | 2007–2009 | ≥ 50 | 4,379 | 8 | 61.0 |
| Meling et al.31 | Norway | 2004–2011 | ≥ 65 | 2,214 | 16 | 79.0 |
| Current study | Korea | 2003–2012 | ≥ 45 | 10,338 | 13 | 85.9 (103.8a) |
Higher BMI was associated with occurrence of AFF in our study. This may indicate that pathophysiology of AFF includes a feature of stress fracture due to higher weight.
Our study demonstrated that the longer duration of bisphosphonate use was a possible risk factor of AFF, although it did not show statistical significance in time-to-event model, Poisson regression analysis. Many studies have presented that the occurrence of AFF was strongly associated with the duration of bisphosphonate use.242132 To prevent AFF, a drug holiday was suggested at 3 or 5 years after bisphosphonate use.333435363738 In our study, the cumulative probability of AFF abruptly increased at 4 years of bisphosphonate use, which support that expert opinions from western countries.3334353637383940
In our study, 20% (10/50) of our AFF patients did not have history of bisphosphonate use before the diagnosis of AFF. The recent ASBMR criteria also did not require a history of bisphosphonate use to define AFF,1 and several studies showed that AFF occurred in patients who did not take bisphosphonate.1632
There are some limitations in this study. First, we could not evaluate previous medication of bisphosphonate elsewhere, because this is a retrospective single center study. If some patients had previously taken bisphosphonate, we would have underestimated the duration of bisphosphonate use. Likewise, we could have missed some AFFs, which had been treated elsewhere. However, our hospital is a tertiary referral hospital and most patients were followed at our hospital due to a difficulty and limitation of repeated referrals in Korea. Second, we could not balance the risk-benefit of continuing bisphosphonate for longer than 5 years. To determine whether to prescribe the medications for longer than 5 years, the long-term efficacy must also be evaluated. Third, we did not distinguish osteoporosis from other medical conditions treated with bisphosphonate in this study.
Despite of these limitations, our findings showed that the incidence rate of AFF in Korea was on a par with those of western countries, and higher BMI was associated with occurrence of AFF. The incidence rate of AFF in Korea can provide basic information to conduct further studies, evaluating risk and benefit of continuing bisphosphonate.
 XML Download
XML Download