

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The life-expectancy around the globe continues to increase, and with the lengthened life, various health problems rise as well.1 Frailty, which has been defined by Fried et al.,2 as having 3 or more of the following symptoms: weight loss, weakness, exhaustion, slowness and low activity, is of much concern, because higher frailty status was shown to be associated with higher disability, mortality, and hospitalization.23 Also, it is important to note that even though the risk of frailty increases with age,4 it has also shown to be preventable and even reversible.5 However, research considering the beneficial factors in regard to frailty has been limited and needs to be investigated further. A possible health behavior that could be protective against frailty is maintaining an active social network,6 which was often measured by an individual's ties with close friends and relatives, marital status, and participation in social activities.7
Increasing number of studies are considering social network in conjunction with various health issues. Previous studies have found association between frequent social contact and lowered risk of depression,89 higher social integration and lowered mortality1011 and better cognition,12 as well as higher social support and lowered level of frailty.6
Studies considering the relationship between social network and frailty are, however, scarce. The findings and methods used are inconsistent and make it difficult to clearly confirm the association between social network and frailty. Woo et al.6 found association between increasing social support and lowered level of frailty, whereas Etman et al.13 and Gale et al.14 focused on negative social network in association with frailty. Furthermore, frailty is becoming easier to operationalize, but the concept of social network is difficult to conceptualize. To elaborate, in terms of research regarding social network, researchers have used terms such as social network,15 social integration,12 or social activity.16 Each definition composes different aspects of social network, which is why it is difficult to measure this construct. However, one common factor that appears across definitions is the frequency of contact (e.g., with friends, family, or neighbors), and frequency of contact is more easily operationalized.
Considering previous research, which presented an increase in frailty status in association with negative social contact,14 we hypothesized that contacting acquaintances less frequently will be associated with higher prevalence of frailty. The aim of this study was to assess the effect of different types of social contact on frailty status. Social contact is thought to be beneficial, because of the support function it provides,7 and by considering the target of contact separately between friends, family, and neighbors, could provide possible indications to the type of people that benefit health the most.
METHODS
Study sample and design
Data were obtained from the Korean Frailty and Aging Cohort Study (KFACS), which gathered its first baseline data in 2016. Detailed information about the study design is provided elsewhere.17 Briefly, KFACS conducted a multi-center based sampling in 10 centers in rural and urban regions across Korea. The sample consisted of people aged 70–84 years old, selected based on age- and gender-specific strata. An in-person interview and health examinations were performed. All participants provided informed consents. The study was approved by institutional review boards of the participating centers. For the first baseline cohort, 1,559 participants were involved, and of those, 1,200 participants with no missing values on the main variables of interest were included.
Independent variables
The independent variable was the frequency of contact with family, friends, or neighbors. Using the KFACS questionnaire, each type of contact frequency was assessed by the question: “How often do you meet or have a chat with … ?” For each question, participants responded by one of the following: daily, 2–3 times a week, at least once weekly, at least once monthly, less than once monthly, or no contact person. These responses were grouped into 4 categories: daily (everyday), weekly (1–3 times a week), monthly (once a month), and rarely (less than once monthly or no contact person).
Dependent variables
The dependent variable of the study was frailty status categorized by Fried's criteria.2 Each component of this criteria was determined as following: weight loss, unintentional weight loss of 4.5 kg or more, or 5% in the last year; weakness, based on grip strength of < 26 kg for men and < 18 kg for women; exhaustion, feeling difficulty with everything or inability to do something more than 3 times in a week; slowness, < 1 m/s in a 4 m walking test; low activity, ≤ 494.65 kcal for men and ≤ 283.50 kcal for women. Presence of 0 component was considered non-frail, 1–2 components pre-frail, and 3 or more components frail.
Control variables
Covariates were collected: gender (men or women), age (70–74, 75–79, or 80–84), education level (< elementary, elementary graduate, or ≥ middle school), monthly household income (< million, 1–2 million, > 2 million in KRW), marriage status (yes or no), number of chronic diseases (0, 1, 2 or ≥ 3), smoking status (yes, past, or never), drinking status (never, < 1 monthly, 1–4 monthly, or ≥ 2 weekly), cognitive functioning (mild cognitive impairment [MCI] or normal), and living status (≤ 8 km or > 8 km). Cognitive functioning was measured using Mini-Mental State Examination in the Korean version of CERAD Assessment Packet (MMSE-KC), and the MCI group and the normal group were determined using a previously proposed guideline.18 Living status was based on the distance of the person (e.g., children, siblings, or relatives) living nearest to the participants. This was then separated into 8 km or less, or more than 8 km.
Statistical analysis
The χ2 test and multinomial logistic regression were used to analyze the association between contact frequency of elderly and their frailty status. For all analyses, the criterion for statistical significance was P < 0.05, two-tailed. All analyses were conducted using the SAS statistical software package, version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Sample characteristics
Baseline characteristics of participants are shown in Table 1. Of the 1,200 participants, 108 (9.0%) were frail, 585 (48.7%) were pre-frail, and 507 (42.3%) were non-frail. Out of those who contacted their family members, 29.6% contacted them daily, 31.0% weekly, 20.5% monthly, and 18.9% rarely. Out of those who contacted their friends, 40.7% contacted them daily, 37.2% weekly, 10.7% monthly and 11.4% rarely. Out of those who contacted their neighbors, 44.0% contacted them daily, 28.3% weekly, 5.5% monthly and 22.2% rarely.
Table 1
General characteristics of participants at baseline

Frequency of social contact by frailty status
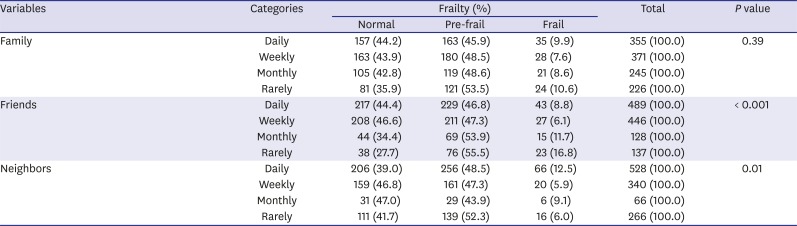
Considering the frequency of contact in terms of frailty status, contact with family showed no significant difference between contact frequency groups, but there were statistically significant differences for contact with friends, monthly (11.7%) and rarely (16.8%) groups showing significantly higher percentage of people compared to the daily (8.8%) group in terms of frailty, and Weekly (47.3%), monthly (53.9%), and rarely (55.5%) groups showing higher percentage of people compared to the daily (46.8%) group in terms of pre-frailty (P < 0.001). There was also a statistically significant difference between groups in terms of contact frequency with neighbors and frailty status (P < 0.01) (Table 2).
Table 2
Frequency of social contact by frailty status
Association between contact frequency and frailty
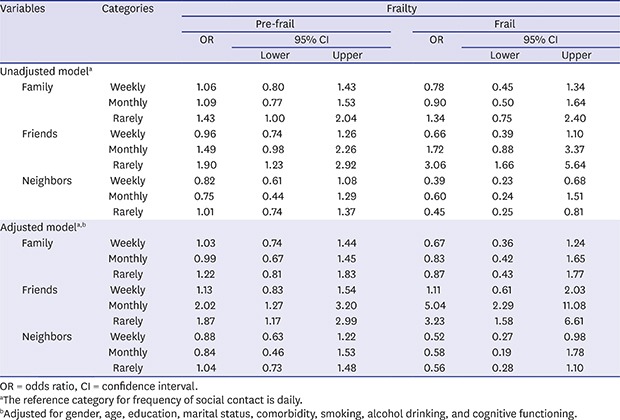
Both the unadjusted and adjusted models of the association between contact frequency and frailty are shown in Table 3. In the unadjusted model, beneficial association between contact frequency was shown mostly in terms of contact with friends, showing higher odds ratio (OR) of both pre-frail (OR, 1.90; 95% confidence interval [CI], 1.23–2.92), and frail (OR, 3.06; 95% CI, 1.66–5.64) in the rarely group, with the daily group as reference. Another beneficial association was presented in terms of contact with family, but it was only shown in terms of pre-frail (OR, 1.43; 95% CI, 1.00–2.04) for the rarely group, with daily group as reference. Opposite association between contact frequency and frailty status was apparent in terms of contact with neighbors. In terms of frail, weekly (OR, 0.39; 95% CI, 0.23–0.68), and rarely (OR, 0.45; 95% CI, 0.25–0.81) groups indicated a lower odds of frailty compared to the daily group.
Table 3
OR and 95% CI of frailty by frequency of social contact
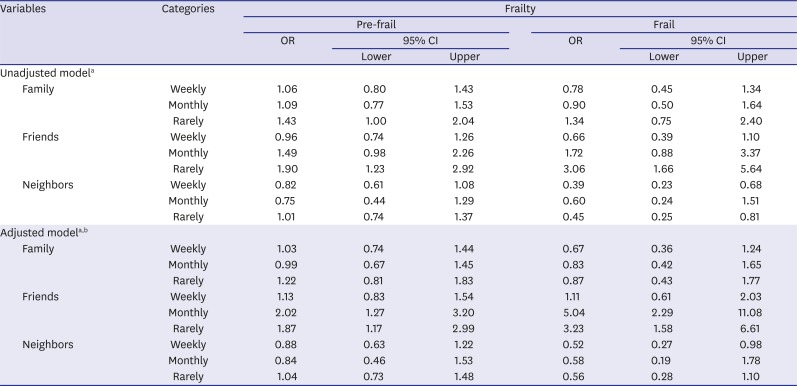
For the adjusted model, there remained no significant association between frailty status and contact with family members. In terms of contact with friends, the odds of pre-frail were significant for those in the monthly (OR, 2.02; 95% CI, 1.27–3.20), and rarely (OR, 1.87; 95% CI, 1.17–2.99) groups compared to the daily group. The odds of frail were also significantly higher among those contacting friends monthly (OR, 5.04; 95% CI, 2.29–11.08) or rarely (OR, 3.23; 95% CI, 1.58–6.61) with daily group as reference. Any significant association between contact with neighbors and frailty disappeared except for the weekly group (OR, 0.52; 95% CI, 0.27–0.98) in terms of frail.
DISCUSSION
In this study, we investigated the association between the frequency of contact with acquaintances and the prevalence of frailty. In accordance with previous studies,61419 our findings indicate that people who maintain less frequent contact with others are at greater odds of prevalent frailty compared to people who maintain better contact frequency. The contact frequency was considered separately for friends, family, or neighbors, and according to our results, different type of contact was associated with frailty differently. Of the three types of contact, contact frequency with friends was most significantly associated with frailty.
A few things could be considered from the beneficial outcomes in terms of contact with friends. First, this is an indication of how different types of the target of contact behave differently in terms of people's health, and that contact with friends are perceived more positively compared to others. However, the possibility of a reverse causality, in which less healthy people contact their friends less frequently, cannot be disregarded. Yet, seeing how beneficial effects of social contact found in this study are in line with previous research showing beneficial effects of social contact on people's health, in terms of level of depression,20 and cognitive decline,21 strengthens the possible relation between social contact and frailty, especially when the target of contact is a friend.
Contact with neighbors was analyzed in our study considering previous research illustrating beneficial effect of neighborhood cohesion in terms of frailty.19 However, our results indicate the possibility of negative association between contact with neighbors and frailty, and this is an important implication. Although frequent social contact has shown beneficial effect in terms of health,81622 previous studies have also shown that poor social relationship can negatively impact health.14 In the same regard, it could be assumed that contacting one's neighbors is perceived negatively, and therefore lead to negative health outcome. However, it is unwise to conclude that contacting one's neighbors frequently is damaging, but further analysis of the association found in our study could provide insight in terms of the mechanisms involved in the association between social contact and health.
The support aspect is often considered the most important in regard to social network.72324 Although this was not analyzed in the current study, a few things could be considered in terms of the linkage between social contact, social support, and frailty. According to our results, it is possible that people perceive their contact with friends as being more supportive compared to family or neighbors, resulting in more beneficial outcomes from contacting one's friends. Although it is difficult to confirm the causal direction between the factors considering the cross-sectional nature of the current study design, the association found proposes the necessity to study the mechanisms involved within this association. For instance, how contacting one's friend is perceived as well as its interaction with the socio-cultural environment around the individual.7
Our study, along with others,131419 has shown positive association between social contact and frailty. Furthermore, we analyzed the target of contact separately to see who is most beneficially associated with people's health. The data were gathered from various sites around Korea, which is useful in terms of generalization. However, because this is a cross-sectional data, causal direction is difficult to determine, and the possibility that healthier people maintain better social contact cannot be disregarded. Also, despite the fact that social contact is a more objective measure of social network, there has not been a clear guideline to group contact frequencies. To account for this limitation, categorization from previous studies,152526 as well as the frequency distribution in our study were considered to generate social contact groups.
This study is important, because it is the first nationwide cohort study focusing on frailty, and the findings provide indication for future research. In the future, a study designed to include more various aspects of social network mechanisms would help to understand the function of social network in an individual's health. Also, the analysis of follow-up data would help better confirm the causal direction between social contact and frailty.
In conclusion, social contact is an important factor in relation to frailty in Korean older adults. Our study also provides implication to the importance of studying the target of contact separately, as well as the underlying mechanisms that affect the relationship between social contact and frailty. Further research in this area will be beneficial for the aging population around the globe.
 XML Download
XML Download