

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Human immunodeficiency virus (HIV) can be transmitted from mother to child. But, with effective preventive measures including universal prenatal HIV counseling and testing, preconception care, antiretroviral prophylaxis, scheduled cesarean section delivery, and avoidance of breastfeeding, the perinatal transmission rate has decreased to < 2% among HIV-exposed infants in developed countries.123 Even though preventive measures could significantly lower the transmission rate, HIV-infected women, particularly those with advanced disease, may have adverse pregnancy outcomes such as preterm birth, low birth weight, and neonatal death.456 Although there have been single-center studies about the prevention of mother-to-child HIV transmission and few mother-to-child transmission cases have been reported by Korea Centers for Disease Control and Prevention (KCDC), a multicenter-based study on pregnancy rate and adverse pregnancy outcomes of HIV-infected women has not been performed, yet.789 This study investigated the pregnancy rates and outcomes in HIV-infected Korean women.
METHODS
Study sites and data collection
We retrospectively reviewed medical records of childbearing-aged (18–50 years) HIV-infected women between January 2005 and June 2017 at four tertiary care hospitals: they were located at Seoul (with 2,400 beds), Suwon (with 1,000 beds), Incheon (with 900 beds) and Wonju (with 850 beds).
HIV-infected mother
Data were collected on maternal status including age, CD4+ cell counts, HIV viral loads, and antiretroviral treatment regimens at the time of the 3rd trimester of pregnancy; preventive measures including antepartum antiretroviral treatment, zidovudine intravenous injection during delivery, cesarean section delivery, avoidance of breastfeeding, and administration of zidovudine syrup to the newborn; and birth outcomes. The number of weeks of pregnancy was determined by examinations at the Department of Obstetrics and Gynecology of each hospital. The follow-up duration was calculated from the first date of visit to the last date of visit.
Definition
A birth earlier than 37 weeks was considered preterm, and birth weight lower than 2,500 g was considered low birth weight. Babies with a body weight below the 10th percentile for their age and sex were considered small for gestational age.10 Neonatal death was defined as death within 28 days of life. If HIV viral loads were negative three consecutive times within six months and HIV antigen/antibody test was also negative at 18 months, the newborn was considered HIV-negative.
RESULTS
There were a total of 95 childbearing-aged HIV-infected women and the total follow-up duration was 587.61 years. The pregnancy rate was 3.57 per 100 patient-years.
Among the 15 HIV-infected women, 21 pregnancies were recorded. Five pregnancies from four HIV-infected women were terminated with induced abortions. Fourteen HIV-infected women gave birth to a total of 16 children: two HIV-infected women gave birth twice during the study period. Two out of 16 children were born earlier than 37 weeks.
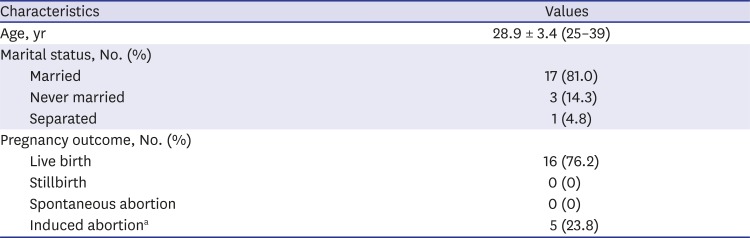
Table 1 shows maternal status and pregnancy outcomes among 21 pregnancies. The mean age of the mothers was 28. 9 ± 3.4 (range, 25–39) years. As for marital status at the time of pregnancy, 17 (81.0%) were married, three (14.3%) were never married, and one (4.8%) was divorced. The partner's HIV status was positive in five (23.8%), negative in 12 (57.1%), and unknown in four (19.0%) pregnancies.
Table 1
Maternal status and pregnancy outcomes among 21 pregnancies
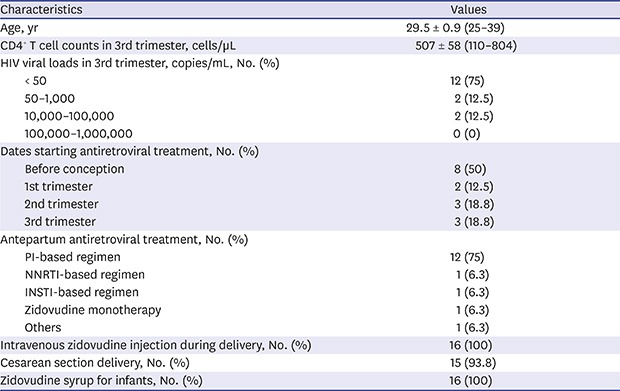
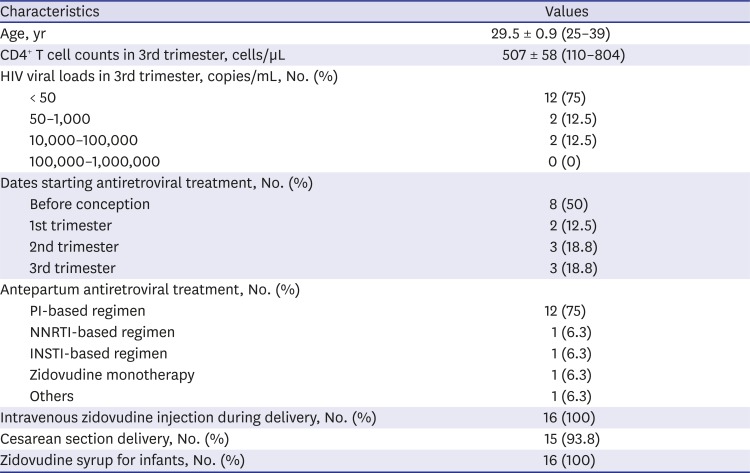
The median CD4+ T cell counts of HIV-infected women who delivered children were 507 ± 58 (110–804) cells/μL in their 3rd trimester (Table 2). The antepartum viral loads in 3rd trimester were suppressed (< 50 copies/mL) in 12 (75%) deliveries, two of the mothers who were unsuppressed (50–1,000 copies/mL) received antiretroviral therapy (ART) before conception and the other two mothers (10,000–100,000 copies/mL) received ART from 3rd trimester. Antepartum ART was given to all of 16 pregnancies and half of them was started before conception. As for antepartum ART regimens, 12 (75%) received protease inhibitor (PI) based ART. One zidovudine monotherapy was given in 2005. Intravenous zidovudine was administered to all mothers during delivery. Fifteen (95%) infants were delivered by cesarean sections. Zidovudine syrup was administered for six weeks and breastfeeding was discouraged for all the infants. We followed-up 13 babies with HIV RNA PCR and antigen/antibody test until 18 months and no infant was confirmed as positive for HIV infection.
Table 2
Maternal status and preventive measures among 16 pregnancies with live birth
Among the 16 live births, there were three infants with adverse outcomes (Table 3). The three infants came from different mothers. One preterm infant was delivered by unplanned cesarean section due to vaginal bleeding at 24 weeks of gestation, with a birth weight of 870 g. His mother did not have any comorbidities except HIV infection with suppressed viral loads and CD4+ T cell counts of 770 cells/μL. The baby died 10 days after delivery due to respiratory distress. Another preterm infant was also delivered by cesarean section due to vaginal bleeding at 35 weeks of gestation. Her birth weight was 2,280 g and her mother also did not have any comorbidities except HIV infection with suppressed viral loads. Thus, these two preterm infants had low birth weights. Another infant with small for gestational age and was delivered by scheduled cesarean section at 38 weeks of gestation. Her birth weight was 2,620 g. Her mother also had no comorbidities other than HIV infection with suppressed viral loads.

DISCUSSION
HIV-infected women tend to avoid pregnancy through contraception and abstinence because of anticipated adverse outcomes such as preterm birth, low birth weight, small for gestational age, stillbirth, neonatal death, and mother-to-child transmission.71112 However, the pregnancy rate has increased, which may be attributed to the widespread application of highly active antiretroviral therapy (HAART), which has resulted in a decrease in mother-to-child transmission.11314 In our study population, the pregnancy rate of HIV-infected women of childbearing age was 3.57 per 100 patient-years, which was lower than the rates reported by other countries (7.4 in the United States and 7.8 in sub-Saharan Africa).1114 The birth rate of child-bearing aged women (20–49 years) in the Korean general population is generally higher than HIV-infected women: 3.71 per 100 woman-years in 2005 and 4.03 per 100 woman-years in 2015, respectively.15 The pregnancy rate of the general population would be higher than the birth rate. We could not evaluate the effect of scaling up of HAART because the pregnancy rate of HIV-infected women in Korea was not previously reported. There were 16 live births and five induced abortions among 21 pregnancies. One induced abortion was therapeutic termination due to ectopic pregnancy. The induced abortion of HIV-infected women is known to be more prevalent than non-infected women,16 and our study showed a high rate (23.8%) of induced abortion among HIV-infected pregnant women in Korea. Exceeding concerns of mother-to-child transmission could give rise to the low rate of pregnancy and high rate of induced abortion.
To prevent mother-to-child transmission, antepartum, intrapartum, and postpartum preventive measures are recommended. All pregnant women are to receive HIV screening tests, ART, avoid breastfeeding, and health care providers must try to minimize exposure of the fetus to mother's blood and body fluids.12 According to our result, all mentioned preventive measures seem to be provided properly. All mothers received antepartum ART, zidovudine intravenous infusion during delivery. Furthermore, all infants received zidovudine therapy after delivery. As a result, mother-to-child transmission was not observed in this study. Two mothers with HIV RNA > 10,000 copies/mL at the 3rd trimester underwent scheduled cesarean section and their children were not infected with HIV. According to a KCDC report, there were 560 HIV-infected women in childbearing age and four mother-to-child HIV transmission cases occurred between 2005 and 2015.9 Considering the KCDC report and pregnancy rate among HIV-infected women from our study (3.57 per 100 patient-years), the presumptive rate of mother-to-children transmission is estimated to be 1.82% ( ), and it is considered to be eliminated by World Health Organization (WHO) criteria.17
), and it is considered to be eliminated by World Health Organization (WHO) criteria.17
), and it is considered to be eliminated by World Health Organization (WHO) criteria.17
A total of three (18.8%) HIV-exposed infants showed adverse outcomes: two (12.5%) preterm births, two (12.5%) low birth weight, one (6.3%) small for gestational age, and one (6.3%) neonatal death. According to a Korean study, the rate of preterm birth and low birth weight were 5.9% and 5.0%, respectively, in 2010.18 Although the rate of adverse birth outcomes was higher than that of the general population, the rates were similar to the incidence in other countries of HIV-infected women, with a preterm birth rate of 13.0% in the United Kingdom and a 23.7% preterm birth rate, an 18.4% small for gestational age rate and a 2.3% neonatal mortality rate in Botswana.4121920 A meta-analysis reported increased risk for preterm birth, low birth weight, small for gestational age, and stillbirth in women who have not received ART compared those who received ART.12 Although all mothers of our study received ART, 50% of mothers started ART after conception, and 25% of mothers had unsuppressed viral loads in 3rd trimester. Fortunately, there was no adverse outcome in infants from mothers with unsuppressed viral loads in 3rd trimester in the present study. In fact, high viral load is a known risk factor for preterm birth and low birth weight.5 Therefore, more efforts are necessary to screen and treat HIV infection for pregnant women in order to prevent adverse birth outcomes. Several studies reported that HAART or a PI-based regimen is associated with preterm birth, and it was also reported that administration of a PI-based regimen in the first trimester increases the risk of preterm birth.62021 Nine pregnant women who were treated with a PI-based regimen before pregnancy or during the first trimester were included in this study. Two of them (22%) had a preterm birth. Since the number of subjects was too small, we could not identify any significant association. On the other hand, there are few studies that show that ART is associated with small for gestational age.2022 The association of adverse pregnancy outcomes with nevirapine has been clearly demonstrated and is now not recommended due to its toxicity.23 In this study, no mother took nevirapine.
There are several limitations to our study. First, the small number of subjects limits the generalizability of our study, and its retrospective nature limits our ability to make any causal determinations. There could be women who were using contraceptive methods, but the relationship between contraceptive methods and outcomes could not be evaluated due to the retrospective nature of this study. In addition, induced abortion or other pregnancy outcomes might have been done in other clinics and not reported to the study hospital. So, the pregnancy rate might be underestimated and maternal mortality and complications may have been overlooked. The pregnancy rate of HIV-infected women in Korea appears to be lower than that of the general population. Although we observed several adverse outcomes including preterm delivery, low birth weight, small for gestational age, and neonatal death, mother-to-child transmission of HIV infection was successfully prevented with effective preventive measures. Further interventions to improve pregnancy outcomes for HIV-infected women are needed.
 XML Download
XML Download