

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Enterococci are normal and usually harmless in most environmental habitats and the gastrointestinal microflora of healthy individuals and animals.1 However, certain enterococcal species easily acquire virulence in vulnerable patients and may cause life-threatening infections such as urinary tract infections, enterococcal bacteremia, and endocarditis.2 The most common species within human intestines are Enterococcus faecalis and E. faecium.3 These two species are also responsible for the majority of nosocomial human enterococcal infections.4
Numerous studies have recognized intrinsic enterococcal resistance to several antimicrobial medications and their ability to develop resistance soon after the introduction of novel antimicrobials.5 In addition, enterococci can transfer multidrug resistance to other microorganisms.6 Since the discovery of vancomycin-resistant enterococci (VRE) in the late 1980s, VRE infections have risen steadily and represent the spread of major healthcare-associated pathogens worldwide despite increasing efforts at control.7
Early guidelines for VRE control focused on the prevention of cross-transmission between patients and medical personnel.8 Subsequent studies emphasized new acquisitions of VRE in healthcare centers as important factors establishing VRE endemicity and aimed to lower the number of VRE patients relative to the whole patient population of the center.9 The hypothesis that nosocomial VRE infections can be effectively controlled by screening patients at high risk of harboring VRE necessitates studies examining risk assessment methods. Primary studies have developed clinical rules to predict whether patients may be VRE reservoirs at the time of admission.10 In this study, we evaluate factors associated with VRE colonization in patients transferred to the emergency department.
METHODS
Study sample
The present study was conducted in the emergency department of an 820-bed medical college-affiliated hospital located in Incheon, Republic of Korea. Incheon is a city in the Seoul metropolitan area, and is the third largest city in Korea, with a population of 2.91 million. The study was conducted at a tertiary referral hospital. In 2016, 57,521 people visited the emergency room of this hospital, and 8,782 (15.3%) were admitted, of whom 2,007 (3.5%) were admitted to the intensive care unit (ICU).
Study design
VRE screening tests were routinely performed during 2016 in the emergency room where this study was conducted to identify the VRE inflow pathway and to establish a VRE control program. Every patient transferred to the emergency department and admitted to our hospital was screened by rectal swab according to methods described in previous study.11 This study was a retrospective study of data derived from medical records that included the results of VRE screening tests.
The study was conducted over a period of 12 months, from January 1 to December 31, 2016. The inclusion criteria were the same as the inclusion criteria for the VRE screening test. Patients who met the following criteria were excluded: patients who were not admitted to another hospital before transfer; patients transferred from a nursing home or a geriatric long-term care facility. Owing to the cross-sectional study design, we included only data from the first visit for patients who were admitted multiple times within the study period regardless of the number of visits. We also excluded patients who were discharged from the emergency department or transferred again, to another hospital. Since VRE transmission within the emergency department was effectively controlled by appropriate protocols, we assumed that no cases of VRE transition occurred while awaiting admission.
We set VRE colonization as the dependent variable in our analyses. VRE colonization was defined based on the results of rectal swab cultures. The independent variables were demographic and clinical factors, and factors related to the transferring hospital. Demographic and clinical factors included age, gender, health insurance, vital signs, mental status, bedsores, initial severity, laboratory studies related to infections such as white blood cell (WBC) count, C-reactive protein (CRP) and neutrophil to lymphocyte ratio, final diagnosis, and ICU admission during the hospital stay. Mental status was categorized as alert or not. We evaluated initial severity using the Korean Triage and Acuity Scale (KTAS) score.12
Factors related to the transferring hospital included number of beds, type of hospital, duration of antimicrobial exposure at the transferring hospital, and hospital days at the transferring. We assessed factors related to the transferring hospital according to referring request documents or statements by patients or caregivers. The number of beds at the transferring hospital was categorized as less than 100, 100–500, or over 500 beds. The type of transferring hospital was categorized as general or geriatric long-term care hospital. The cut-offs for duration of antimicrobial exposure at the transferring hospital were three days and seven days. The cut-offs for hospital days at the transferring hospital were three days and seven days.
Statistical analysis
Statistical analyses were performed with IBM SPSS Statistics ver. 18.0 for Windows (IBM Co., Armonk, NY, USA). Patients were divided into two groups, the VRE group and non-VRE group, based on one or more VRE colonization events. Previously collected patient data were analyzed for differences in basic characteristics by the χ2 test, independent samples t-test, and Mann-Whitney U-test. We performed logistic regression analyses of characteristics that significantly differed between groups to identify risk factors associated with VRE colonization in patients transferred to the emergency department. Statistical significance was defined when P values were less than 0.05.
RESULTS
A total of 5,892 patients were transferred to our hospital and 742 patients were admitted within the study period from January 2016 to December 2016. Rectal swabs for VRE culture was carried out for 701 patients. Of these, a total of 650 patients were enrolled, except for 23 patients who were referred to other hospitals from the emergency department and 28 patients who were admitted more than once during the study period. No patient was excluded because of missing data. Of the 650 enrolled patients, 106 (16.3%) who had positive VRE culture results were categorized in the VRE group and the remaining 544 patients made up the non-VRE group.
VRE culture results showed that E. faecium colonization was detected in all 106 patients. No patients were colonized by E. faecalis. Among patients with VRE colonization, 52 (49.1%) were diagnosed with infectious diseases. The most frequent diagnosis in the VRE group was pneumonia, which was diagnosed in 19 patients (17.9%). Other frequent diagnoses were urinary tract infection in 17 patients (16%) and 7 (6.6%) with hepato-biliary infection.
Demographic and clinical characteristics of patients in the VRE and non-VRE groups are as shown in Table 1. Median age was significantly higher in the VRE group than in the non-VRE group. VRE group patients were more likely to have bedsores than non-VRE group patients. Other factors such as vital signs, mental status, laboratory test results known to be related to infectious disease, and initial severity did not significantly differ between groups.
Table 1
Comparison of demographic and clinical factors between VRE and non-VRE groups
The characteristics related to the transferring hospital are as shown in Table 2. VRE group patients were more likely to be transferred from geriatric long-term care hospitals. The duration of antimicrobial exposure at the transferring hospital and admission days at the transferring hospital differed significantly between the VRE and non-VRE groups, but the number of beds of the transferring hospital did not.
Table 2
Factors related to transferring hospitals in VRE and non-VRE groups
The results of the logistic regression analysis of factors shown to be risk factors for VRE infections are presented in Table 3. Age, the presence of bedsores, and transfer from geriatric facilities were independent risk factors for VRE infections in patients transferred to the emergency department.
Table 3
Results of logistic regression analysis

DISCUSSION
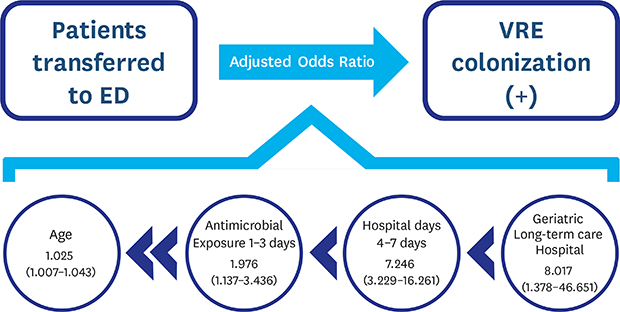
We observed that transfer from a geriatric long-term care hospital, hospital days, duration of antimicrobial exposure, and age were associated with VRE colonization in patients transferred to emergency departments in Korea. VRE colonization in transferred patients was mainly associated with factors related to the transferring hospitals rather than factors related to patient demographic and clinical characteristics.
According to the Korean National Healthcare-associated Infections Surveillance System (KONIS) Manual 2016, the rate of vancomycin resistance among E. faecium isolated from patients with nosocomial infections during ICU admission in Korea is 48.3%. This represents an increase compared to the vancomycin resistance rate of 40.3% observed five years prior. A Korean study determined that 184 patients (17.6%) out of 1,048 admitted to a single medical ICU over a period of 21 months had VRE colonization.13 A follow up study conducted in 2018 in the same ICU found that 37 patients (22.8%) had VRE colonization among 142 patients who had undergone liver transplantation.14
In this study, among patients who were transferred to the emergency department of a tertiary referral hospital, the proportion of patients with VRE colonization was 16.3%. This result is not significantly different from the 17.6% reported in a previous study conducted in a single ICU in a tertiary referral hospital.13 This indicates that the reason why VRE infections have not decreased despite continuing infection control in referral hospitals in Korea may be associated with patients transferred from other hospitals.
Among demographic and clinical factors, age and presence of bedsores were associated with significant differences in the dependent variable. These results were consistent with those of previous studies showing that age and wound type were associated with VRE infection.1516 However, there was no association with bedridden state, which was associated with infections in a previous study.17 This may be explained by the relatively low numbers of bedridden patients transferred to emergency departments.
Among factors related to transferring hospitals, those associated with significant differences in the dependent variable were type of transferring hospital, duration of antimicrobial exposure, and hospital days. These results were consistent with those of previous studies showing that duration of antimicrobial exposure and hospital days are associated with VRE infection.1718 Previous studies that examined the type of transferring hospital, another independent variable that showed a significant difference, were scarce. The exact same type of hospital as geriatric long-term care hospital exists only in Korea and Japan. However, these results are not expected to be significantly different from those of previous studies, in which patients hospitalized in long-term wards or residents in geriatric long-term care facilities had higher rates of VRE infection.19
The variables that were significant in the logistic analysis were transfer from geriatric long-term care hospital, hospital days, duration of antimicrobial exposure, and age. The only variable related to demographic and clinical factors was age, and all other variables were related to the transferred hospital. The odds ratio of variables related to the transferred hospital were relatively large.
This study had several limitations. First, because the data were collected from referring request documents or the statements of patients or caregivers, it was often difficult to identify the types of antibiotic that patients had received. Therefore, we were forced to examine duration of exposure to any antibiotics instead of duration of exposure to vancomycin specifically. Second, the analysis of clinical factors such as objective severity and prognosis was not sufficient. However, we believe that the associations between clinical factors and VRE colonization would not have been strong. Third, this was a retrospective study based on medical records. In retrospective studies, experimental design and statistical analysis cannot always completely control for confounders.
 XML Download
XML Download