

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tumor necrosis factor (TNF) inhibitors have been increasingly used to treat immune-mediated inflammatory diseases (IMIDs), such as rheumatoid arthritis, ankylosing spondylitis, and inflammatory bowel disease (IBD). However, patients treated with TNF inhibitors are at an increased risk of developing tuberculosis including extrapulmonary tuberculosis1 because of the reactivation of latent tuberculosis infection (LTBI).2 These findings have led to the implementation of policies to diagnose LTBI prior to the initiation of TNF inhibitor treatment.34
Current diagnostic tests for LTBI include tuberculin skin tests (TST) and interferon-gamma release assay (IGRA). Additionally, to determine LTBI treatment, other factors, such as chest X-ray screening, physical examination, medical history including previous tuberculosis treatments and their adequacy, and the history of recent contact with patients with active tuberculosis, are considered.2 The widespread screening and treatment of LTBI prior to TNF inhibitor treatment have dramatically reduced the incidence of tuberculosis.5 However, previous studies have reported several cases of patients with IMID who developed tuberculosis associated with TNF inhibitor use, despite negative LTBI screening results.6789 Moreover, some studies have reported the development of active tuberculosis in patients with IMID who received appropriate LTBI treatment prior to the initiation of TNF inhibitors.69 These reports suggest that although appropriate LTBI test and subsequent treatment prior to TNF inhibitor treatment can reduce the incidence of tuberculosis in patients with IMID, tuberculosis can still develop in patients with negative LTBI results as well as those receiving adequate LTBI treatment. To our knowledge, no study has been conducted that focuses upon the incidence of active tuberculosis in patients with IBD with different LTBI statuses who are undergoing TNF inhibitor treatment. Therefore, this study investigated this issue in Korea, where the incidence of tuberculosis is considered to be intermediate (80–100/100,000 per year).10
METHODS
Study subjects
This retrospective cohort study was performed between January 2011 and June 2017, with 740 patients with IBD, including cases of Crohn's disease and ulcerative colitis. All patients underwent TNF inhibitor treatment and were followed-up for ≥ 1 at Asan Medical Center, a 2,700-bed tertiary care center in Korea. The enrolled patients were selected from among 895 patients after applying the following exclusion criteria: 1) patient was followed-up for < 1 year, 2) patient did not undergo LTBI screening test, or 3) patient was diagnosed as having active tuberculosis at the screening visit (Fig. 1). Medical records of the remaining patients were retrospectively analyzed in August 2017.

LTBI screening strategy
During the screening visit, information was registered regarding the presence of any symptoms suggestive of tuberculosis, a medical history of previous tuberculosis treatment, and the use of anti-inflammatory drugs such as azathioprine or steroids. All patients were examined for the presence of bacillus Calmette–Guérin scars. All patients underwent simple chest radiography, and those with radiographic abnormalities suggestive of tuberculosis were further evaluated using sputum acid-fast bacilli smear and culture to rule out active tuberculosis or lung disease due to nontuberculous mycobacteria. TST and/or IGRA were performed on the same day during the baseline examination. TST was performed with 2TU PPD RT23 (Statens Serum Institute, Copenhagen, Denmark), following the Mantoux approach. Induration size was measured after 48–72 hours through the ballpoint method, and an induration ≥ 10 mm was defined as positive, as indicated in the Korean Tuberculosis Guidelines.11 In addition, IGRA was performed using the QuantiFERON-TB Gold In-Tube (QFT-GIT; Cellestis, Carnegie, VIC, Australia), according to the manufacturer's instructions.12 An interferon-γ value of ≥ 0.35 IU/mL was considered as a positive QFT-GIT result. LTBI was considered positive if either the TST or QFT-GIT result was positive.
Criteria for LTBI treatment and its regimen
LTBI treatment was initiated in patients with positive results, normal chest radiography, and the absence of tuberculosis-suggestive symptoms. Moreover, patients with a positive TST and/or QFT-GIT result, a history of previous adequate anti-tuberculosis treatment, and no further tuberculosis exposure were not treated for LTBI. Patients with no previous anti-tuberculosis treatment history and presenting with chest X-ray abnormalities suggestive of spontaneously healed tuberculosis (e.g., non-calcified nodules with distinct margins, discrete linear or reticular fibrotic scars, and fibrotic linear opacity) received LTBI treatment regardless of TST or QFT-GIT results. TNF inhibitor was initiated at 4 weeks after LTBI treatment.
During the study period, the primary selected regimen for LTBI treatment was a combination of isoniazid and rifampin administered for 3 months.13 In the case of adverse events or intolerance to the treatment, a new regimen was used, comprising either isoniazid for 9 months or rifampin for 4 months. Treatment completion required completing > 80% of all prescribed medication within 4 months for isoniazid/rifampin combination, 12 months for isoniazid, and 6 months for rifampin.
Follow-up and development of active tuberculosis
Regardless of the LTBI status, the patients were followed-up by pulmonologists until 6 months after the completion of the TNF inhibitor treatment. Chest X-ray screening was performed at 3 and 9 months after treatment initiation, and at every 12 months thereafter to detect cases of active tuberculosis. The patients were instructed to visit their physicians if they presented any new symptoms or signs suggestive of tuberculosis. For the present study, only the cases where active tuberculosis developed within 1 year of treatment initiation were considered to be treatment-related because the risk of developing tuberculosis due to the reactivation of LTBI is highest within 1 year after the initiation of TNF inhibitor treatment.1415
Statistical analysis
Results are presented as means and standard deviations for continuous variables and numbers and percentages for categorical variables. The risk of developing tuberculosis was assessed on the basis of the standardized incidence ratio (SIR) and its 95% confidence interval (CI) for active tuberculosis. The observed number of tuberculosis cases was divided by the expected number of tuberculosis cases for each 10-year age- and sex-stratified general population in Korea. The expected number of tuberculosis cases was estimated on the basis of the incidence of active tuberculosis in the entire population in 2014, which was the midpoint of the study period, provided by the Korean Centers for Disease Control and Prevention.16 In addition, for patients diagnosed with active tuberculosis within 1 year, the number of person-years at risk (pyr) was calculated from the date of initiation of TNF inhibitor treatment until the date of tuberculosis diagnosis. Continuous variables were analyzed with a Student's t-test, whereas categorical variables were analyzed with either χ2 or Fisher's exact test. All tests were two-sided, and a P value < 0.05 was considered as statistically significant. All analyses were performed using the SPSS software (version 21.0; SPSS, Chicago, IL, USA).
RESULTS
Clinical characteristics of study patients
Following the application of eligibility criteria, a total of 740 patients with IBD who received TNF inhibitor treatment were enrolled (Fig. 1). Mean patients age was 33.1 ± 12.0 years, and 65.8% (487/740) of the patients were male. Patients with Crohn's disease were predominant (80.7%). During the study period, 3 types of TNF inhibitors were administered: infliximab (prescribed to 68.5% of the cases), adalimumab (prescribed to 30.7% of the cases), and golimumab (prescribed to 0.8% of the cases). Azathioprine was the most frequently used anti-inflammatory agent. A detailed description of the cases is presented in Table 1.
Table 1
Clinical characteristics of 740 patients with IBD treated with TNF inhibitor according to the LTBI status
Data are reported as mean ± standard deviations or number (%).
IBD = inflammatory bowel disease, TNF = tumor necrosis factor, LTBI = latent tuberculosis infection, BMI = body mass index, TB = tuberculosis, BCG = bacillus Calmette–Guérin, CXR = chest radiography.
aSwitch of TNF inhibitors: infliximab to adalimumab in 23 patients, adalimumab to infliximab in 4 patients, infliximab to adalimumab in 1 patient, and golimumab to infliximab in 1 patient; bOthers include methotrexate, 6-mercaptopurine, and sulfasalazine.
Diagnosis and treatment of LTBI
As shown in Fig. 1, 84 among 740 patients (11.4%) presented with LTBI (LTBI group). Among those, 49 (58.3%) showed negative TST and positive QFT-GIT results, whereas 18 (21.4%) showed positive results for both TST and QFT-GIT, 16 (19.0%) showed a positive TST and a negative or indeterminate QFT-GIT result, and 1 patient (1.2%) presented chest X-ray findings suggestive of spontaneously healed tuberculosis, with no history of tuberculosis treatment. Among the 84 patients, 72 (85.7%) completed LTBI treatment with isoniazid/rifampin combination for 3 months, whereas the 12 remaining patients underwent regimen changes due to intolerance and adverse events. From those 12 patients, 9 completed LTBI treatment with the new regimen, resulting in an overall completion rate of 96.4% (81/84) of LTBI group. The remaining 3 patients did not complete LTBI treatment due to various adverse events, such as nausea with vomiting.
Meanwhile, the remaining 656 patients classified as non-LTBI group, 645 (98.3%) showed negative results for both TST and QFT-GIT, whereas 11 (1.7%) showed an adequate treatment history of tuberculosis and positive results for TST and/or QFT-GIT. As shown in Table 1, the two groups differed in several baseline characteristics, such as age, sex, body mass index, type of IBD, TNF inhibitor used, and anti-inflammatory drugs administered.
Development of tuberculosis within 1 year according to the LTBI status and treatment
During the follow-up period, 14 cases of active tuberculosis occurred (Fig. 1), from which 6 were excluded due to being diagnosed more than 1 year after treatment initiation. The remaining 8 cases were included in the analysis. As shown in Fig. 1, 1 patient in the LTBI group (1/84; 1.2%) and 7 patients in the non-LTBI group (7/656; 1.1%) developed active tuberculosis within 1 year after the initiation of TNF inhibitor treatment. Detailed characteristics of these 8 patients are presented in Table 2.
Table 2
Characteristics of 8 patients who developed active tuberculosis during TNF inhibitor treatment

Incidence of 1-year tuberculosis according to the LTBI status and in relation to the general population
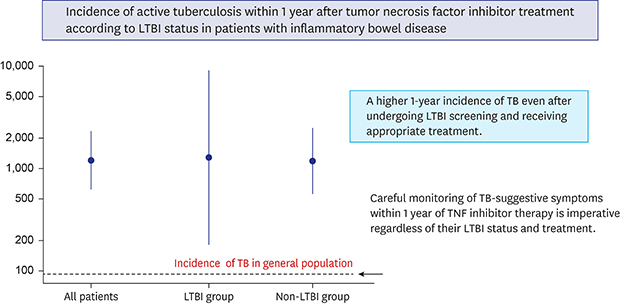
Table 3 shows the observed number of tuberculosis cases and SIRs of all patients (both LTBI and non-LTBI group). The overall incidence of 1-year tuberculosis adjusted for sex and age, was significantly higher among the study patients than in the general population (SIR, 14.0; 95% CI, 7.0–28.0), and there was no significant effect of the LTBI status on SIR (LTBI group: 14.0, 95% CI, 2.0–99.0, non-LTB group: 14.0, 95% CI, 6.7–29.4). Fig. 2 shows incidence rates of active tuberculosis per 100,000 pyr after the initiation of TNF inhibitor treatment in patients with IBD. Average tuberculosis incidences among IBD patients were 1,276.8 per 100,000 pyr (95% CI, 638.5–2,553.2) overall, 1,270.5 per 100,000 pyr (95% CI, 179.0–9,019.7) for the LTBI group, and 1,277.7 per 100,000 pyr (95% CI, 609.1–2,680.2) for the non-LTBI group.


DISCUSSION
The use of TNF inhibitors has been validated as a suitable treatment for IBD.17 However, a small number of patients with IBD have been known to develop treatment-related tuberculosis even after screening and adequate treatment for LTBI.7818 To the best of our knowledge, this was the first study to compare the incidence of active tuberculosis in patients with IBD with different LTBI status within 1 year after the initiation of TNF inhibitor treatment. We showed that the incidence of active treatment-related tuberculosis among patients with IBD was 14 times higher than that in the general population even after LTBI screening was performed and adequate treatment was administered. Notably, this high incidence was not significantly affected by the LTBI status of the patients.
We considered the development of tuberculosis to be related to TNF inhibitor therapy only if it was diagnosed within 1 year of treatment initiation because the risk of LTBI reactivation is the highest during the first 6–12 months of TNF inhibitor treatment.141920 A previous study has reported a biphasic development of active tuberculosis disease during long-term TNF inhibitor treatment in patients with rheumatoid arthritis, with an early development occurring within the first 3 months and a late development after 20–24 months of therapy.21 Active tuberculosis disease could be caused by LTBI reactivation in those with an early development of tuberculosis and by de novo infection in those with the baseline negative LTBI results and a late development of tuberculosis.21 In previous studies analyzing the development of active tuberculosis in patients with IMID, including those with IBD, all cases were included regardless of time period following TNF inhibitor treatment.67891822 That is, these studies included active tuberculosis with late as well as early development in their analyses, leading to difficulties in the interpretation of results. In the present study, we analyzed only the cases that developed tuberculosis within 1 year of treatment initiation since the baseline LTBI screening prior to the use of TNF inhibitors prevents the early development of active tuberculosis and theoretically cannot prevent its late development. To our knowledge, this was the first study to analyze the incidence of active tuberculosis in IBD patients treated with TNF inhibitors, wherein late tuberculosis development was excluded.
In the present study, 1 patient within the LTBI group (No 1. in Table 2), who had been treated for LTBI, was diagnosed with active tuberculosis. The most plausible explanation was that anti-tuberculosis chemoprophylaxis is only partially successful in patients with IMID. In a study performed in Greece with 613 enrolled patients of rheumatic diseases who had received TNF inhibitor treatment,23 45 patients received chemoprophylaxis for LTBI treatment, and 6 of those patients developed active tuberculosis within 1 year after the initiation of TNF inhibitor treatment. Similar observations have been reported by other authors,2425 and a recent study conducted in the Netherlands has reported that the estimated reduction in the risk of active tuberculosis following preventive treatment among LTBI patients ranged between 40% and 60%.26 Taken together, these findings suggest that although the screening and treatment of LTBI prior to TNF inhibitor can dramatically reduce the incidence of tuberculosis,5 complete prevention may not be achievable. Another possible explanation is that patients develop tuberculosis due to a new infection with Mycobacterium tuberculosis even within relatively short periods. Immunocompromised condition attributable to TNF inhibitor treatment makes these patients susceptible to active tuberculosis. While our patients' histories were not suggestive of exposure to other infectious patients, living in a tuberculosis-prevalent country such as Korea makes inadvertent exposure plausible.
Among the 656 patients of non-LTBI group, 7 patients developed active tuberculosis despite a negative LTBI result or a history of previous adequate tuberculosis treatment. It was probable that the development of tuberculosis in these patients was due to the incomplete sensitivity of LTBI tests, including TST and/or IGRA. That is, TST and IGRA can provide false-negative results following immunosuppressive therapy comprising oral immunosuppressants, steroids and biological therapy.27 TST requires an intradermal infiltration of T-specific cells through the induction of several cytokines, levels of which is often reduced by immunosuppressive therapy.28 In addition, one meta-analysis has shown a pronounced negative effect of immunosuppressive therapy on IGRA results; IGRA may not be reliable for the diagnosis of LTBI in patients undergoing immunosuppressive therapy, including TNF inhibitor, steroids, and oral immunosuppressants.29 Recently, Edwards et al. have evidently shown that corticosteroids significantly impair QFT-GIT performance.30 Since the 7 patients who developed active tuberculosis were being treated with immunosuppressive agents such as steroids at the time of LTBI test, the test results may have been affected by these agents. It should also be noted that the immune system is responsible for both yielding a positive IGRA result as well as preventing progression to active tuberculosis; as such, individuals with false-negative IGRAs may be the very individuals (e.g., highly immunosuppressed) at the greatest risk of reactivation.31 To avoid a high rate of false-negative results, Taxonera et al.32 have suggested in patients with IBD that LTBI be detected through an early screening test performed in the absence of immunosuppressive treatment and/or significant inflammatory activity in order to maximize the sensitivity of the test.
A correct interpretation of the present results must be made in the light of the study's limitations. First, this was a retrospective non-randomized study conducted in a single-tertiary referral center in Korea, which is known to have an intermediate tuberculosis burden. Therefore, our results cannot be readily extrapolated to the general population of patients with IBD in other regions where the incidence rates of tuberculosis are different from ours. Second, adherence to treatment was not confirmed by direct observations, implying that noncompliance to LTBI treatment, which is difficult to ascertain, may have affected the efficacy of LTBI treatment. Third, the retrospective nature of the study may have limited the collection of accurate data regarding the close contact with active tuberculosis patients. In addition, the risk of tuberculosis can be different depending on the type of a TNF inhibitor33; therefore, the result of our study may not be applied in institutions where different kinds of TNF inhibitors are frequently prescribed.
In conclusion, we showed that patients with IBD who are undergoing TNF inhibitor treatment showed a higher 1-year incidence of tuberculosis than the general population even after undergoing LTBI screening and receiving appropriate treatment. The most relevant finding was that the incidence of tuberculosis was independent of LTBI status, that is, IBD patients with or without LTBI showed a nearly similar high incidence of active tuberculosis after the initiation of TNF inhibitor treatment. These results imply that clinicians should be aware of the risk of the development of active tuberculosis in patients with IBD with negative LTBI result as well as those who receive adequate LTBI treatment following a positive result. Therefore, the careful monitoring of tuberculosis-suggestive symptoms within 1 year of TNF inhibitor therapy is imperative in patients with IBD regardless of their LTBI status and treatment.
 XML Download
XML Download