

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic kidney disease (CKD) is a well-known risk factor for cardiovascular disease and mortality.1 CKD caused by nephrectomy may increase mortality by inducing cardiovascular disease; thus, to preserve kidney function, partial nephrectomy (PN) has become the standard surgical care for small renal masses.2345 However, the benefits of partial versus radical nephrectomy (RN) are still under debate, particularly as they relate to the survival advantage of PN.6789101112131415
PN is the preferred treatment modality for renal cell carcinoma (RCC) in patients with pre-existing CKD, when technically feasible. However, little is known about differences in overall survival (OS) and postoperative renal function between patients undergoing RN and PN for the treatment of RCC in patients with pre-existing CKD. To address this gap in the literature, we evaluated the impact of PN over RN on survival rate and kidney function in patients with stage III CKD.
METHODS
Study population
We retrospectively collected data from 5,916 patients who underwent RN or PN for localized RCC from January 1988 through December 2014 at eight institutions in Korea.16 After excluding 1,584 patients with solitary kidney, bilateral RCC, stage pT3 or greater, lymph node or distant metastases, preoperative hemodialysis, or pre-existing stage IV CKD (estimated glomerular filtration rate [eGFR] < 30 mL/min/1.73 m2) and those with missing preoperative kidney function records, we finally analyzed 4,332 patients who underwent PN or RN for pathological T1a-T2N0M0 RCC in this study. To evaluate the effects of PN on survival rate according to CKD stage, we divided patients into two subgroups: CKD I–II (eGFR ≥ 60 mL/min/1.73 m2) and CKD III (30 ≤ eGFR < 60 mL/min/1.73 m2). Data included age, sex, body mass index (BMI), preoperative nutritional status (albumin and hemoglobin levels), comorbidities (diabetes and hypertension), American Society of Anesthesiologists (ASA) score, tumor size, pathologic stage, Fuhrman grade, tumor histology, and preoperative kidney function (eGFR).
Primary outcomes
The primary outcome was difference in postoperative kidney function and OS between the PN and RN arm according to baseline kidney function. OS was calculated by death from any cause after surgery. Cancer-specific survival (CSS) was assessed by the cancer-related death rate. Data regarding death and the cause were obtained from the database of every participating center and updated by the office for Korean National Statistics. The follow-up period was calculated from the date of surgery to the date of the last known contact with the patient or the date of death. To assess the longitudinal change in kidney function after nephrectomy, serial serum creatinine data were collected annually for each patient. The eGFR was calculated using the Modification of Diet in Renal Disease equation.17
Statistical analysis
Differences between groups of patients receiving PN and RN in baseline clinical and pathological characteristics were compared using the Mann-Whitney test for continuous variables and the χ2 test for categorical variables. To reduce the impact of treatment selection bias, we performed rigorous adjustment for significant differences in characteristics of patients by use of the propensity score. Patients were pair-matched by age, sex, BMI, preoperative nutritional status (albumin and hemoglobin levels), comorbidities (diabetes and hypertension), ASA score, tumor size, pathologic stage, Fuhrman grade, tumor histology, and preoperative kidney function (eGFR). OS and CSS were estimated by the Kaplan-Meier method and compared by the log-rank test. OS represents the time from surgery to death from any cause. CSS represents the time from surgery to death by cancer. Cox proportional hazards regression models were used to assess the relation of surgery type with survival rate or new onset of stage IV CKD. In the descriptive analyses of kidney function, the mean eGFR in each group was evaluated separately and plotted against each follow-up point. Probabilities of freedom from new onset of stage IV CKD after nephrectomy were also compared using Kaplan-Meier plots. To study the relationship between nephrectomy type and repeated longitudinal measurements of eGFR, and to obtain the slope of the kidney function decline over time and reliable confidence intervals (CIs) of nephrectomy type effects on the renal function trajectory, linear mixed models (with random intercepts and slopes specific to each participant) were used. We calculated a separate regression line with time slopes to compare the differences in the slopes of eGFR decline according to the nephrectomy type. Two-sided tests were performed, and P values < 0.05 were considered statistically significant. All statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS version 24.0; IBM, Chicago, IL, USA).
RESULTS
Patient demographic and clinical characteristics
Table 1 shows the baseline characteristics of patients. Before propensity matching analysis, there were significant differences in tumor size, diabetes distribution ratio, Fuhrman grade, pathologic stage, and tumor histology type between RN and PN arms. These differences were eliminated by matching. In the CKD I–II group, 878 RN patients were matched with 878 PN patients. The median pre-eGFRs were 77.1 and 78.7 mL/min/1.73 m2 in each arm (RN vs. PN), respectively. The median follow-up durations in the RN and PN arms were 52 (interquartile range [IQR], 18–81) and 43 (IQR, 12–62) months, respectively. In the CKD III group, 138 RN patients were matched with 138 PN patients. The median pre-eGFRs were 54.1 and 53.8 mL/min/1.73 m2 in each arm (RN vs. PN), respectively. The median follow-up durations in the RN and PN arms were 56 (IQR, 18–78) and 52 (IQR, 20–72) months, respectively.
Table 1
Baseline characteristics of patients who underwent PN or RN after propensity score matching

Values are presented as number of patients (%) or median (IQR).
RN = redical nephrectomy, PN = partial nephrectomy, CKD = chronic kidney disease, IQR = interquartile range, BMI = body mass index, ASA = American Society of Anesthesiologists, POD = postoperative day, eGFR = estimated glomerular filtration rate.
Kidney function after radical or PN
Among patients with CKD stage I–II, kidney function was significantly better preserved in the PN group than in the RN group regardless of the postoperative period (Fig. 1A). Also, PN showed better kidney function compared with RN in the early postoperative period among patients with CKD stage III. However, the beneficial effect of PN on kidney function was not sustained (Fig. 1B). There was a significant difference in the decreasing eGFR between the PN and RN groups among patients with CKD stage I–II (−0.039 vs. −0.302 mL/min/1.73 m2/mon, respectively, P < 0.001; Fig. 2A). However, RN was not associated with a higher eGFR decrease compared to PN among patients with stage III CKD (−0.077 vs. −0.073 mL/min/1.73 m2/mon, respectively, P = 0.589; Fig. 2B). Kaplan-Meier analysis showed that the 5-year CKD IV-free survival rates after surgery were not significantly different among patients with CKD stage I–II and stage III. (Fig. 2C and D). The incidences of new onset CKD stage IV after RN and PN were 3.6% (five patients) and 1.4% (two patients). However, in Cox hazards models for CKD stage IV, patients who underwent PN were not significantly different compared with their RN-treated counterparts (hazard ratio [HR], 0.573; 95% CI, 0.137–2.400; P = 0.446). Only one patient in the RN arm required dialysis.
Fig. 1
Changes in eGFR over time after RN and PN. (A) Patients with CKD I–II and (B) patients with CKD III.
eGFR = estimated glomerular filtration rate, RN = radical nephrectomy, PN = partial nephrectomy, CKD = chronic kidney disease.
Fig. 2
Changes in the eGFR over time after PN (red line) and RN (blue line) stratified by CKD stage (A, B). Slopes are based on regression coefficients from the linear mixed models. Solid line: regression line, dotted line: 95% CI. (A) Patients with CKD I–II. (B) Patients with CKD III. Kaplan-Meier survival curves for CKD IV free survival stratified by nephrectomy type (C, D). (C) Patients with CKD I–II. (D) Patients with CKD III. Red line: PN; Blue line: RN.
eGFR = estimated glomerular filtration rate, CKD = chronic kidney disease, PN = partial nephrectomy, RN = radical nephrectomy, CI = confidence interval.
Survival rate after radical or PN
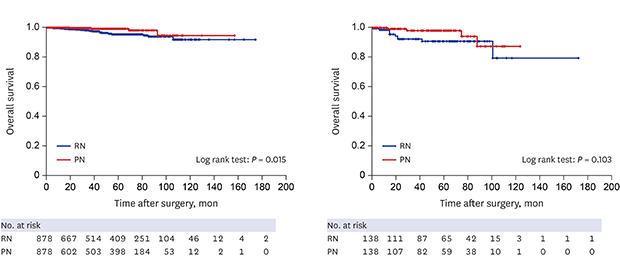
In the CKD I–II group, the 5-year OS rates after surgery were 99.4% for PN versus 96.5% for RN (P = 0.015; Fig. 3A). The 5-year CSS rates were 99.7% for PN versus 99.5% for RN (P = 0.492; Fig. 3C). Table 2 summarizes the adjusted HRs for clinical end points in the PN arm versus the RN arm. Patients undergoing PN were at a significantly lower risk of kidney function decrease and death from any cause. In Cox hazards models for OS and CSS, although patients who underwent PN did not have a significantly different CSS rate compared with their RN-treated counterparts, the OS rate was different (OS: HR, 0.320; 95% CI, 0.122–0.840; P = 0.021; CSS: HR, 0.466; 95% CI, 0.050–4.311; P = 0.501). In the CKD III group, the 5-year OS rates after surgery were 97.8% for PN versus 93.5% for RN (P = 0.103; Fig. 3B). The 5-year CSS rates were 99.3% for PN versus 98.5% for RN (P = 0.287; Fig. 3D). OS and CSS were not significantly different between the two arms (OS: HR, 0.395; 95% CI, 0.124–1.260; P = 0.117; CSS: HR, 0.313; 95% CI, 0.033–3.008, respectively, P = 0.314).
Fig. 3
Survival rate stratified by CKD stage and nephrectomy type. Kaplan-Meier estimating curves for overall survival (A, B), and cancer specific survival (C, D) according to nephrectomy type (PN [red line] versus RN [blue line]). CKD I–II patients: (A) and (C); CKD III patients: (B) and (D).
PN = partial nephrectomy, RN = radical nephrectomy, CKD = chronic kidney disease.
Table 2
Cox regression analyses for OS, CSS, and new onset of CKD IV survival

DISCUSSION
The effects of PN and RN on survival rate and renal function in patients with stage III CKD have not been evaluated in detail. Compared to RN, PN is thought to have a more favorable effect on OS in patients with deteriorated preoperative kidney function. In our previous study, we observed that the renal function of patients with CKD stage I or II recovered after RN and that the same phenomenon occurred in patients with CKD III.18 However, the level of renal function recovery was lower in patients with CKD stage III than in those with CKD stage I or II. We hypothesized that among patients with CKD III, RN would be more detrimental to kidney function than PN, and expected to see a greater survival benefit following PN among patients with CKD III than among those with CKD I or II. However, the results of this study contradicts our hypothesis.
The major findings of this study were: 1) there was no difference between PN and RN arms in the rate of eGFR decrease among CKD stage III patients, although the superior benefit of PN over RN was consistently maintained between the two nephrectomy types in CKD stage I–II patients; 2) the 5-year OS and CSS survival rates in the RN arm were comparable to those of the PN arm in patients with pre-existing CKD III; and 3) the OS was higher after PN than after RN in patients with preoperative normal kidney function. The results obtained for CKD stage III patients are seemingly counterintuitive because it is conceivable that in pre-existing CKD, the functional recovery capacity is not maintained by physiological compensation.
Several underlying mechanisms may explain this phenomenon. First, a similar kidney function after nephrectomy may affect the OS rate. After surgery, kidney function was significantly better preserved in the PN arm than in the RN arm in the early period after surgery. The eGFR drops sharply by 20 mL/min/1.73 m2 on average when RN is performed in CKD I–II patients, whereas it decreases by approximately 10 mL/min/1.73 m2 on average in CKD III patients. In the CKD III group, patients who underwent PN maintained their postoperative kidney function up to a certain level while the postoperative kidney function of patients that underwent RN recovered gradually over time; therefore, statistically significant differences in the postoperative eGFR of PN and RN groups disappeared with time. Kidney ischemia in PN may have irreparable damage to operated kidney in CKD III patients. These changes may be associated with the survival rate of patients. Furthermore, it is possible that RN may not affect survival unless the eGFR reaches the cutoff value for dialysis (30 mL/min/1.73 m2), a variable which did not differ between groups.
Second, PN may not increase OS compared to RN in certain patients. Recent studies reported that the benefits of PN with regard to OS or kidney function can vary depending on the patient's preoperative kidney function, age, comorbidity, and tumor size and anatomy.192021222324 Woldu et al.19 found that the benefits of PN on kidney function were observed only in patients with CKD stage II, and not in those with CKD stage III, despite the fact that most urologists would prioritize PN in the latter group in daily clinical practice. Sun et al.20 reported that compared to RN, PN was not protective of other-cause mortality in elderly patients (aged ≥ 75) with localized RCC or those with multiple comorbidities at diagnosis. Meanwhile, Larcher et al.21 argued that PN was beneficial only to patients with significant comorbidities. However, the authors also contended that PN decreased other cause mortality over RN only in specific subgroup of patients with RCC. An et al.22 and Chung et al.23 also reported that PN was not more favorable than RN in terms of OS in elderly patients. Kopp et al.24 compared survival differences to investigate the prognostic impact of tumor anatomical variation or stage, and found that the benefits of PN might fade away for complex tumors. Another study also confirmed no survival difference between PN and RN in a propensity adjusted cohort of patients with T1b RCC.25 The current study demonstrated that the differences between OS rates after PN and RN disappeared in patients with pre-existing CKD.
We found that the relative benefit of PN over RN in reducing mortality and preserving kidney function was consistently observed in patients with preoperatively normal kidney function. Furthermore, given that the kidney function and survival outcomes were comparable for the two nephrectomy types, RN may be selected as a relatively safe treatment for RCC in specific patients with pre-existing CKD stage III. The remarkable finding in this study is that the benefits following PN were not sustained in patients with pre-existing CKD stage III. However, given the significant risks associated with RN, PN should still be the method of choice in this patient group. Also, it should not be overinterpreted that RN would not completely cause severe cardiovascular disease or fatal mortality in patients with preexisting CKD.
Our study has several limitations. First, this was a retrospective study, and this design may have affected the results owing to unmeasured confounders. No statistical method of adjustment can completely abolish this limitation. Second, only a small number of patients were followed up. It is possible that the lack of difference in OS between the two arms in stage III CKD may have been affected by the limited number of patients throughout follow-up. Third, only healthy patients with available contact information and relatively better baseline kidney function (CKD IIIA) who were still alive were included as CKD stage III patients.
The choice of PN versus RN should be made based on a variety of clinical factors. When considering PN in a patient with pre-existing CKD, the issue of potential morbidity in relation to the patient's health condition needs to be discussed, because the decision to perform RN versus PN is influenced by preoperative renal function. Our study adds to the current knowledge about the beneficial effect of PN on survival rate and kidney function in patients with pre-existing CKD. Our use of a large consecutive patients recruited at multiple centers may be a good reference indicator of real world outcomes.
In conclusion, PN is associated with a higher OS rate in patients with preoperative CKD stages I and II. However, compared with RN, PN did not show a better 5-year risk of death and kidney function in patients with pre-existing CKD stage III. Additional studies should be conducted to investigate the patient characteristics for which the benefit of PN may be maximized.
 XML Download
XML Download