

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Globally, 240 million people representing 5%–6% of the world population are chronically infected with hepatitis B virus (HBV).1 Although the prevalence of HBV infection is decreasing in Korea, it is still a serious public health problem of liver-related morbidity and mortality.2 Chronic HBV infection predominantly manifests as hepatic diseases such as chronic hepatitis, liver cirrhosis, and hepatocellular carcinoma. However, extrahepatic manifestations including renal diseases, polyarteritis nodosa or dermatologic diseases such as popular acrodermatitis occur in 10%–20% of HBV infected patients even in the absence of hepatic disease.34 Recognition of these extrahepatic manifestations is important for the comprehensive care of HBV infected patients, especially in the era of highly effective antiviral therapy.
HBV-related renal diseases could lead to chronic kidney disease (CKD)56 and subsequent end-stage renal disease (ESRD).78 It can be classified as immune complex glomerulonephritis (membranous nephropathy or membranoproliferative glomerulonephritis) and immune complex-related vasculitis (polyarteritis nodosa9 or cryoglobulinemic vasculitis8). Although the pathogenic mechanism behind these renal manifestations is not clear,10 deposition of HBV-related immune complexes,11 HBV replication in the renal tubular epithelium which may promote apoptosis of renal tubular cells,12 HBV-related insulin resistance,13 and oxidative stress14 may contribute to renal dysfunction.
Even though HBV-related CKD and ESRD cases are encountered in the clinic, there are only a few studies on the association between HBV infection and the development of CKD at a population level. Moreover, those studies showed striking disparate results on the role of HBV infection in CKD.15161718 Thus, the aim of this study was to investigate the association between chronic HBV infection and the prevalence of CKD defined as a decreased estimated glomerular filtration rate (GFR) or proteinuria in a population-based, nationwide study in Korea.
METHODS
Study design and data acquisition
This was a multicenter, retrospective, cross-sectional, and matched case-control study. A total of 265,086 subjects who underwent a health-check examination including hepatitis B virus surface antigen (HBsAg) status were enrolled nationwide in 33 hospitals from January 1, 2015 to December 31, 2015. After exclusion of 1,325 people who showed anti-hepatitis C virus (HCV) antibody positivity, 10,048 subjects who showed HBsAg positivity were identified (cases). For the purpose of comparison, 40,192 HBsAg negative subjects (controls) were randomly selected in the same dataset who were 1:4 matched for age by decades and gender using the R program (R Foundation, Vienna, Austria; www.r-project.org/) version 3.3.3.
Demographic data, including age, gender, resident address, height, and weight were obtained from an electronically extracted database for the health-check examinee at each hospital. The laboratory results of the blood chemistry obtained after overnight fasting included the fasting plasma glucose, serum protein, albumin, bilirubin, cholesterol, alanine aminotransferase (ALT), hemoglobin A1c (HbA1c), urea nitrogen, creatinine, thyroid stimulating hormone and complete blood cell count as well as an assay for the HBsAg and anti-HCV antibody. Urine analysis was performed with spontaneously voided clean-caught mid-stream fresh urine. Urine protein was measured using an immediate semi-quantitative urine protein dipstick test and graded as negative, trace, 1+, 2+, 3+, or 4+.
Serum HBsAg was measured mainly using chemiluminescent microparticle immunoassay with Abbott Architect assay and electrochemiluminescence immunoassay. Dipstick urine analysis was performed using the Urisys 2400 cassette strip, which was read by Urisys 2400 automated analyzer (Roche, Mannheim, Germany) in 50% of the hospitals, and various ways in the remaining hospitals. Serum creatinine level was measured using the compensated kinetic alkaline picrate (Jaffe reaction) in 70% of the hospitals, so that the estimated GFR was calculated with the Modification of Diet in Renal Disease equation19:
Although each hospital has different testing methods, the quality control of all the measuring method was certified by clinical laboratory accreditation program, which was operated by the Korean Society of Laboratory Medicine.
Definition of the CKD, proteinuria, and anemia
The stages of CKD were classified into 6 categories (G1 to G6) by the clinical practice guideline Kidney Disease: Improving Global Outcomes 201220: G1, the participants had a GFR of at least 90 mL/min/1.73 m2; G2, a GFR of 60–89 mL/min/1.73 m2; G3a, a GFR of 45–59 mL/min/1.73 m2; G3b, a GFR of 30–44 mL/min/1.73 m2; G4a, a GFR of 15–29 mL/min/1.73 m2, and G5a, a GFR less than 15 mL/min/1.73 m2. In this study, a decreased GFR was defined as a GFR < 60 mL/min/1.73 m2 (GFR categories G3a–G5), and the proteinuria was defined as the presence of urine protein of at least grade 2+ in the urine protein dipstick test. Therefore, CKD was defined as a GFR < 60 mL/min/1.73 m2 or proteinuria at least grade 2+. Anemia defined as serum hemoglobin level < 13 g/dL in men, and < 12 g/dL in women according to World Health Organization criteria.
Statistical analyses
All data were expressed as the means ± standard deviation or as a percentage. The continuous variables were analyzed with t-tests, and categorical variables were investigated with Pearson's χ2 tests. Conditional logistic regression model analyses were used to determine the independent factors associated with the decreased GFR and proteinuria. P < 0.05 was considered to indicate a statistical significance. The statistical analyses were performed using SPSS version 24.0 (SPSS, Inc., Chicago, IL, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of each hospital (Seoul National University Bundang Hospital approval No. B-1602/336-101). The data were analyzed anonymously. Informed consents were waived because this was a retrospective data analysis study.
RESULTS
Comparison of the clinical characteristics between the HBsAg positive cases and the age- and gender-matched controls
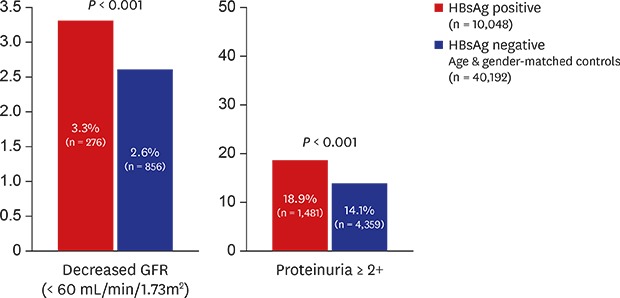
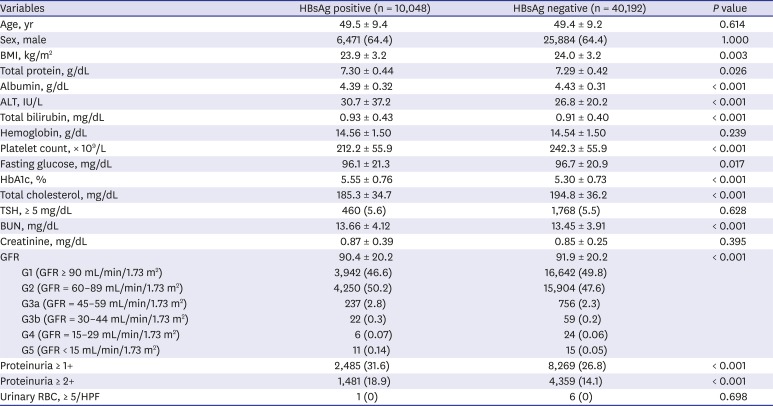
The clinical characteristics of a total 50,240 subjects consisting of 10,048 HBsAg positive cases and 40,192 control subjects are summarized in Table 1. In the case group, the mean age was 49.5 years with male proportion of 64.4%. The mean ALT level was higher in the case group than in the control group (30.7 IU/L vs. 26.8 IU/L; P < 0.001), while the serum albumin level was lower in the case group compared with the control group (4.39 g/dL vs. 4.43 g/dL; P < 0.001). The mean serum cholesterol level (185.3 mg/dL) and platelet count (212.2 × 109/L) were significantly lower in the case group compared with those of the control group (194.8 mg/dL [P < 0.001] and 242.3 × 109/L [P < 0.001], respectively). While the mean serum blood urea nitrogen level in the case group (13.66 mg/dL) was significantly higher than in the case group (13.45 mg/dL, P < 0.001), the mean serum creatinine level was not significantly different between the case and control group. However, the prevalence of GFR < 60 mL/min/1.73 m2 in the case group (3.3%) was significantly higher than in the control group (2.6%, P < 0.001). Moreover, the prevalence of proteinuria (≥ +2) in the case group (18.9%) was significantly higher than in the control group (14.1%, P < 0.001). Therefore, HBsAg positive cases showed a significantly higher frequency of CKD than the HBsAg negative controls.
Table 1
Baseline characteristics of the subjects at study entry by serostatus of HBsAg
Association between HBsAg positivity and GFR < 60 mL/min/m2
In the univariate analysis, HBsAg positivity, age (≥ 50 years), body mass index (BMI) (≥ 25 kg/m2), serum protein (≥ 6.4 g/dL), serum albumin (≥ 3.5 g/dL), serum bilirubin (≥ 1.2 mg/dL), HbA1c (≥ 6.5%), and anemia were the candidate variables for the multivariate analysis (P < 0.05). In the multivariate analysis, age (odd ratio [OR], 5.49; 95% confidence interval [CI], 3.65–8.26; P < 0.001), HbA1c (OR, 1.89; 95% CI, 1.53–2.33; P < 0.001), BMI (OR, 1.31; 95% CI, 1.13–1.52; P < 0.001), HBsAg positivity (OR, 1.23; 95% CI, 1.0–-1.45; P = 0.015), serum albumin (OR, 0.23; 95% CI, 0.09–0.56; P = 0.001), serum bilirubin (OR, 0.81; 95% CI, 0.67–0.98; P = 0.029) and anemia (OR, 2.28; 95% CI, 1.75–2.98; P < 0.001) were the independent factors for GFR < 60 mL/min/m2 (Table 2 and Fig. 1).
Table 2
Univariate and multivariate logistic analyses of decreased GFR (< 60 mL/min/1.73 m2) with subgroup analysis by sex

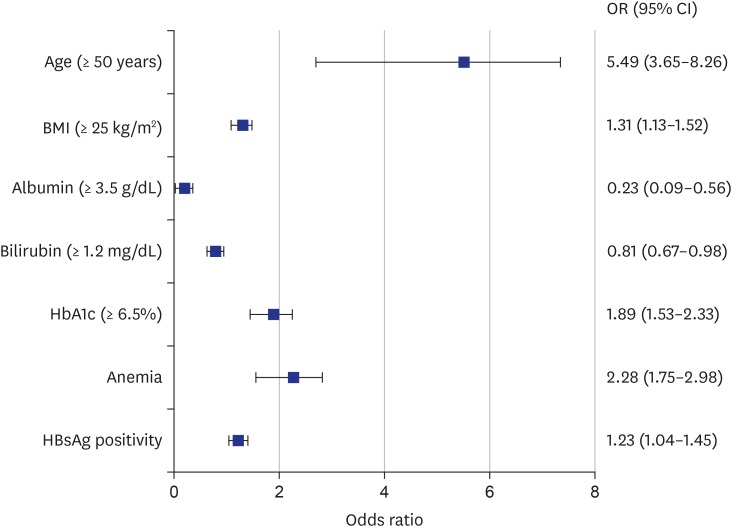
Fig. 1
Forest plot of the impact of the risk factors for a decreased GFR (GFR < 60 mL/min/m2). Age (P < 0.001), HbA1c (P < 0.001), BMI (P < 0.001), HBsAg positivity (P = 0.015), serum albumin (P < 0.001), serum bilirubin (P = 0.029), and anemia (P < 0.001) were the independent factors for a decreased GFR.
GFR = glomerular filtration rate, HbA1c = hemoglobin A1c, BMI = body mass index, HbsAg = hepatitis B virus surface antigen, OR = odds ratio, CI = confidence interval.
To clarify the sex-specific association between HBsAg positivity and CKD, we conducted a subgroup analysis by sex. HBsAg positivity was an independent risk factor for GFR < 60 mL/min/m2 in male (OR, 1.39; 95% CI, 1.14–1.69; P = 0.001) but not in female. In contrast, BMI was an independent factor for GFR < 60 mL/min/m2 in female but not in male (Table 2).
Association between HBsAg positivity and proteinuria (≥ 2+)
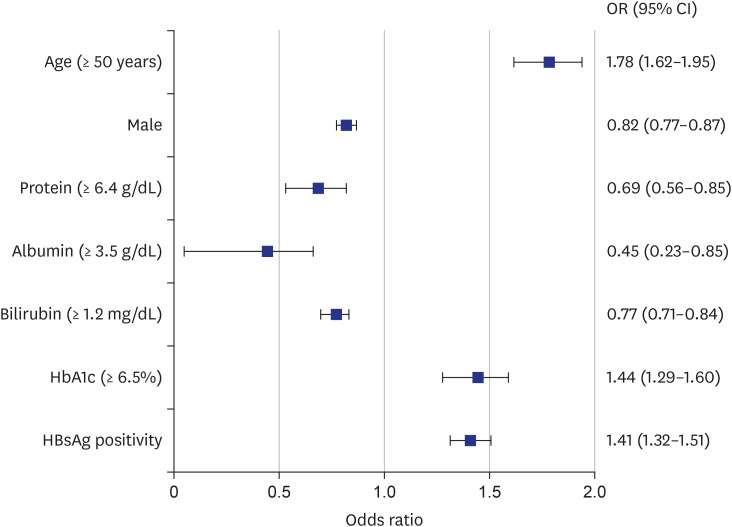
In the univariate analysis, HBsAg positivity, age (≥ 50 years), male, serum protein (≥ 6.4 g/dL), serum albumin (≥ 3.5 g/dL), serum bilirubin (≥ 1.2 mg/dL), HbA1c (≥ 6.5%), and cholesterol (≥ 200 mg/dL) were the candidate variables for the multivariate analysis (P < 0.05). In the multivariate analysis, HBsAg positivity (OR, 1.41; 95% CI, 1.32–1.51; P < 0.001) was the independent risk factor of proteinuria along with age (OR, 1.78; 95% CI, 1.62–1.95; P < 0.001), HbA1c (OR, 1.44; 95% CI, 1.29–1.60; P < 0.001), male (OR, 0.82; 95% CI, 0.77–0.87; P < 0.001), bilirubin (OR, 0.77; 95% CI, 0.71–0.84; P < 0.001), albumin (OR, 0.45; 95% CI, 0.23–0.85; P < 0.001), and total protein (OR, 0.69; 95% CI, 0.56–0.85; P < 0.001) (Table 3). Fig. 2 shows a forest plot of the independent risk factors associated with the proteinuria (≥ 2+). In the subgroup analysis by sex, HBsAg positivity was an independent factor associated with proteinuria in both male and female (Table 3). No significant difference was found in the relationship between HBsAg positivity and the CKD (eGFR < 60 mL/min/m2 or proteinuria 1+) in both male and female subjects (Supplementary Table 1).
Table 3
Univariate and multivariate logistic analyses of proteinuria (≥ 2+) with subgroup analysis by sex
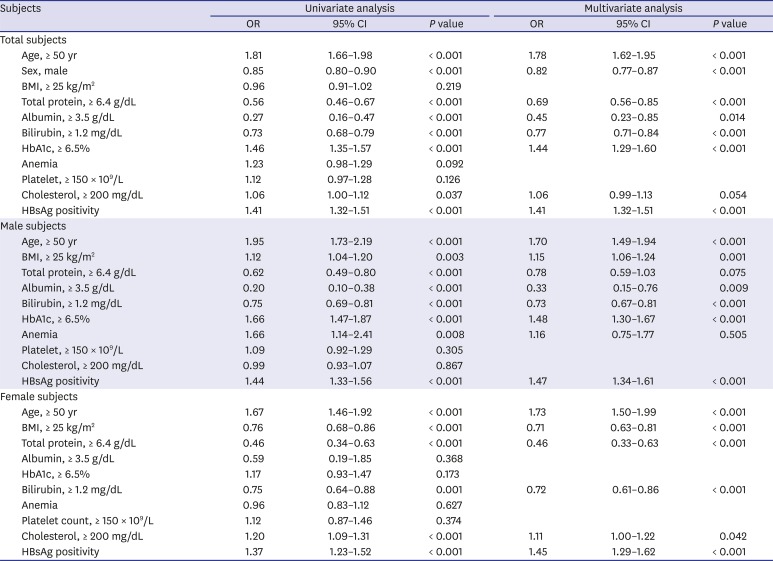
Fig. 2
Forest plot of the impact of the risk factors for proteinuria (≥ 2+). HBsAg positivity (P < 0.001) was the independent risk factor of proteinuria along with age (P < 0.001), HbA1c (P < 0.001), male gender (P < 0.001), bilirubin (P < 0.001), albumin (P = 0.014), and total protein (P < 0.001).
HbsAg = hepatitis B virus surface antigen, HbA1c = hemoglobin A1c, OR = odds ratio, CI = confidence interval.
DISCUSSION
In this nationwide multicenter study, we demonstrated that HBsAg positive cases showed a significantly higher frequency (3.3%) of a GFR < 60mL/min/m2 than that of the HBsAg negative, age-sex matched controls (2.6%), and they also showed a higher frequency of proteinuria ≥ 2+ (18.9%) than that of the controls (14.1%). Moreover, HBsAg positivity was an independent factor not only for a GFR < 60 mL/min/m2 but also for proteinuria in the multivariable logistic regression analysis. Interestingly, the subgroup analysis showed that the association between HBsAg positivity and a GFR < 60 mL/min/m2 was only confirmed in male but not in female.
A 2-year multicenter cross-sectional, single arm French study (Hepatitis and Renal Parameters Evaluation) showed that renal abnormality was highly prevalent in treatment-naïve chronic hepatitis B patients (n = 280): a GFR < 60 mL/min/1.73 m2 in 3.5% (4/73) and proteinuria ≥ 1+ in 38.1% (59/155). It was similar with the results of our study: a decreased GFR in 3.3% and proteinuria ≥ 1+ in 30.9% among the HBsAg positive cases.21 The HBsAg, HBV core antigen or HBV e antigen was detected within immune complex deposits in kidney tissues from patients with HBV associated glomerulonephritis (HBGN). Moreover, the sera of HBV-infected patients induced the apoptosis of human kidney proximal tubular epithelial cells by up-regulation of Fas.12 The circulating Cu/Zn superoxide dismutase levels, suggesting an enhanced oxidative stress were higher in hepatitis B patients undergoing renal replacement therapy than in patients without hepatitis B.14 Serum HBV-DNA levels were associated with proteinuria in HBGN,22 and antiviral therapy against HBV, such as lamivudine with or without immunosuppressive therapy, resulted in a complete resolution of membranous nephropathy in 75%–80% of patients.232425 Therefore, these findings support the role of HBV infection in the development of renal injury.
However, several clinical studies on the association between the HBV infection and CKD showed highly controversial results. Lee et al.17 reported that HBV infection was not associated with CKD in a Taiwanese community based cross-sectional study that included health check examinees (n = 54,996) from April to November 2004, while HCV infection was associated with CKD. However, the same authors reported that HBV infection, but not HCV infection, was associated with CKD in elderly patients > 60 years of age, which was not consistent with their previous study.18 A Japanese single center health check examinee study (n = 12,535) during 2004 and 2006 showed that HBV infection (n = 130, 1.0%) was not associated with a lower GFR and albuminuria, while HCV infection (n = 72, 0.6%) was associated after adjusting for age, sex, systolic blood pressure and fasting glucose. However, further adjustment for either homeostasis model assessment insulin resistance or serum ALT abolished the association between HCV infection and albuminuria.15 A Chinese single center health check examinee study (n = 15,600) from 2009–2012 showed that there was no association between either HBV or HCV infection and CKD; however, the presence of hypertension, diabetes, albumin level, triglyceride level and total cholesterol level were independent factors, while age and sex were not significant factors.26
In contrast to the above cross-sectional studies, a longitudinal 13-year nationwide Taiwan cohort study using the National Health Insurance Research Database (n = 88,980) from 1996–2010 showed that untreated chronic HBV infection was associated with an increased risk of CKD (adjusted hazard ratio [HR], 2.58; 95% CI, 1.95–3.42), and the association was significant in male of any age and female under the age of 50 but not in female aged 50 years or older.6 The same authors also reported that untreated chronic HBV infection is associated with an increased risk of ESRD (12-year cumulative incidence, 1.9%) compared with a non-HBV cohort (0.49%) (adjusted HR, 3.85; 95% CI, 2.83–4.50; P < 0.001).7 Another single-center cohort study from Hong Kong that included 2,838 patients with type 2 diabetes enrolled during 1995–1999 showed that chronic HBV infection was associated with an increased risk of ESRD (adjusted HR, 1.53; 95% CI, 1.11–18.58; P = 0.036) during a median follow-up of 3.5 years.27 All of the above 3 published longitudinal study results were similar with our cross-sectional study results showing that chronic HBV infection was significantly associated with a decreased GFR (adjusted OR, 1.22; 95% CI, 1.03–1.43) and with proteinuria (adjusted OR, 1.35; 95% CI, 1.27–1.43).
Previous studies have shown that age, diabetes mellitus, hypertension, male, anemia, and obesity are independent risk factors for CKD,2829 which was partially concordant with our results; old age, high BMI, high HbA1c level, anemia, and hypoalbuminemia, as well as HBsAg positivity, were independent factors associated with GFR < 60 mL/min/m2. In the subgroup analysis by sex, HBsAg positivity remained an independent factor for GFR < 60 mL/min/m2 in male but not in female. This finding is consistent with a previous cross-sectional study.30 It may be related to the higher susceptibility of chronic HBV infection and the higher risk of HBV-related liver injury in male than in female.31 Moreover, the renal protective role of estrogen was also demonstrated previously32: the course of kidney disease is more modest in female than in male,3334 and estrogen replacement therapy can help to improve renal functions in menopausal women.35
Screening proteinuria by dipstick is often the first approach to evaluate the kidneys and provides a sensitive test for renal disease from early to advanced stages.36 In this study, HBsAg positivity was an independent factor for proteinuria not only among all the subjects but also in both male and female in the subgroup analysis.
Although the present study could not provide information on the HBV-DNA level and HBV genotype, almost all (95%–99%) of the Korean hepatitis B patients exhibited the HBV genotype C37 which is more virulent and has a lower antiviral response to interferon than that of genotype B.3839 Lei et al.40 reported that individuals with HBV genotype C may be more susceptible to HBGN and severe clinical manifestation. Additionally, individuals with HBV genotype C may be susceptible to renal damage due to a high viral load.
There are several limitations in this study. Because of the nature of the data, information on the serum HBV-DNA level and antiviral therapy against HBV was not available. Even though some portions of the cases may have had received antiviral drugs with complete control of HBV replication, HBsAg positivity remained as an independent factor for CKD or proteinuria in this study. Second, this study had a cross-sectional design with a single measurement for the GFR and proteinuria which do not provide the causal relationship between HBV infection and CKD. Third, because our case group was defined as HBsAg positive individuals, very rare case of acute hepatitis B may be not excluded in this group. However, majority of acute hepatitis B cases in adults showed a symptomatic presentation, so that they may go doctor's clinic rather than health-check examination center. Fourth, the selection bias would be existed in our study because it is likely that subjects with relatively good health and economic conditions underwent health-check examination. Furthermore, the GFR was not determined by a direct measurement, and the estimated GFR may not accurately reflect renal function in some patients with a severe liver disease because these patients had decreased muscle and creatinine production. Lastly, information on hypertension, diabetes, medication, and liver images such as abdomen ultrasonography and/or abdomen computed tomography was not available, and we could not assess potential confounders associated with the decreased GFR or proteinuria. Despite these limitations, to our knowledge, this is the first study to report a population level association between chronic HBV infection and CKD in Korea with a large sample size and comprehensive laboratory results.
In conclusion, this large, nationwide, multicenter study indicates that HBV infection is significantly associated with CKD. Especially, male sex may affect the association between HBV infection and CKD. Therefore, physicians should pay attention to the renal function as well as the liver function of chronic hepatitis B patients in the era of effective antiviral therapy.
 XML Download
XML Download