

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tobacco smoke is one of the leading public health issues worldwide. Global burden of disease (GBD) study 2013 reported that Korea is included among those countries of the world which have high prevalence as well as high consumption (number of cigarettes per smoker/day) of tobacco smoking, which in turn increase the health threats by secondhand smoke (SHS) as well.1 Tobacco smoke (including SHS) was the third principal cause of disease burden in Korea in 2013. According to recent studies, 44.8% of Korean men were exposed to SHS in 2012 and years of life lost (YLL) due to SHS was 9,077 in 2010.2
As SHS is a considerable health problem in Korea, quantifying the related disease burden is a powerful tool for decision making, formulation of evidence-based policies and priority settings. Previous scientific studies in Korea mostly calculated attributable fraction, YLL and relative risk of SHS.2345 Most of these studies are outdated and lack the updated methodology and comprehensive model of burden of disease (BOD) calculation. One previous study calculated BOD attributable to Secondhand Smoking in Korea using updated Korean data and new GBD study methodology. That study reported total BOD due to SHS was 44,143 disability adjusted life years (DALYs) with 57% from men and 43% from women.6 However, all of these previous studies focused on the situation at national level only with no figures for sub-national level.
GBD 2013 calculated BOD by a restructured methodology.7 Years lived with disability (YLD) were calculated by disease prevalence rather than incidence. For PAF calculation of active smoking, smoking prevalence was replaced with smoking impact ratio (SIR) to reflect the accumulative effect of past exposure to smoking. The GBD study calculated BOD of SHS in Korea but it also lacks the use of reliable country specific data. Additionally, it did not calculate the BOD at sub-national level for Korea.
SHS exposure is an involuntary behavior and affected by a number of regional contextual factors, for example, smoking ban policies at sub-national level within a country can have different outcomes in each state.8 Several previous studies proved the effect of legal smoking restrictions on health outcomes and SHS exposure.910 In Korea, regional governments started implementing smoke-free policies since August 2010. Many communities have announced smoking restrictions but time of implementation and extent of coverage is different with in regions. In order to assess the influence of these governmental plans, calculation of disease burden in these regions can be a very effective tool. Sub-national estimates of BOD can help researchers and policy makers to evaluate health disparities within a country and to make tailored plans and policies according to precise regional situation. The GBD study also calculated BOD at sub-national level for few countries like China and Japan but there are no estimates for Korea.11
Therefore, our study aims to calculate BOD due to SHS among nonsmokers in 252 regions of Korea. Most recent and reliable sub-national statistics in Korea will be used and most updated methodology developed by GBD will be applied. This study will provide a quantification of disease burden due to SHS within each region and will be helpful in evaluating the effect of smoke-free regulations and formulation of future policies by local governments.
METHODS
This study followed the GBD methodology for calculating BOD. Firstly, active smoking BOD was calculated and then subtracted from total burden to calculate SHS burden among nonsmokers.
The following steps were followed for calculations.
Selection of SHS and active smoking related health outcomes and relative risk
Systematic review of previous studies was performed to select diseases related to SHS. Final list of health outcomes was selected on the basis of level of evidence for relation with SHS and quality of study design. Detailed procedure of the systematic review has been described in our national level article.12 Finally, three diseases including lung cancer, Ischemic heart disease (IHD) and stroke were found to have strong evidence of association with SHS in adults. Health outcomes for BOD calculation along with ICD-10 codes are given in Table 1.
Table 1
Health outcomes with ICD-10 codes and RR

| Diseases | ICD-10 codes | Relative risk | |
|---|---|---|---|
| SHS (From GBD 2013)7 | Active smoking | ||
| Trachea, bronchus and lung cancer | C33–C34 | 1.506 for both genders and all age groups | NAa |
| IHD | I20–I25.9, Z82.4–Z82.49 | 25–29 yr = 1.468 | 2.2 for men; 1.7 for women1314 |
| 30–34 yr = 1.433 | |||
| 35–39 yr = 1.4 | |||
| 40–44 yr = 1.368 | |||
| 45–49 yr = 1.336 | |||
| 50–54 yr = 1.305 | |||
| 55–59 yr = 1.276 | |||
| 60–64 yr = 1.247 | |||
| 65–69 yr = 1.219 | |||
| 70–74 yr = 1.191 | |||
| 75–79 yr = 1.165 | |||
| 80+ yr = 1.139 | |||
| Stroke | I60, I61, I62.0, I63, I64, I65, I66, I67.0, I67.1, I67.2, I67.3, I67.5, I67.6, I67.7, I69.0, I69.1, I69.2, I69.3, G45, G46 | 25–29 yr = 1.59 | 1.6 for both genders and all age groups1314 |
| 30–34 yr = 1.541 | |||
| 35–39 yr = 1.493 | |||
| 40–44 yr = 1.448 | |||
| 45–49 yr = 1.405 | |||
| 50–54 yr = 1.362 | |||
| 55–59 yr = 1.322 | |||
| 60–64 yr = 1.283 | |||
| 65–69 yr = 1.246 | |||
| 70–74 yr = 1.211 | |||
| 75–79 yr = 1.177 | |||
| 80+ yr = 1.145 | |||
As good quality Korean studies related to SHS are not available, relative risk (RR) was taken from the GBD 2013 study, which generated age specific RR using integrated exposure curves, based on previously published articles for RR.7 RR for active smoking was derived from Korean studies. Systematic review of Korean literature was done using the same procedure and search engines as SHS. RRs for each disease along with reference article and ICD-10 codes are mentioned in Table 1.
Calculation of population attributable fraction (PAF)
PAF calculation of SHS
Age and gender specific PAF for SHS was calculated using the following standard formula:
Where PSHS is the proportion of adult nonsmokers (25 years and above) who are exposed to SHS at work or home and in each region RRSHS is the relative risk of disease among people who are exposed to SHS, to the risk among people who are unexposed.
Following the GBD study, no lag time was used for prevalence of SHS.7
PAF calculation of active smoking
Prevalence based formula of PAF calculation was used for diseases with short lag (IHD and stroke).
Where PCS is age and gender specific proportion of adults who are current active smokers in each region and RRCS is the relative risk of disease due to active smoking. Five year lagged smoking prevalence was used following the GBD study.7
For diseases with long lag period (e.g., cancer), a new methodology for PAF has been introduced in the GBD study in which current smoking prevalence has been replaced with SIR. Detail of this method is mentioned in national BOD calculation.12
Data source
For PAF calculation at sub-national level, regional prevalence of SHS was taken from Community Health Survey (CHS) 2013 while prevalence of current active smoking was derived from CHS 2008 (5-year lag). CHS is conducted annually since 2008, in 254 regions of Korea. This survey uses a multistage sampling design to obtain a sample of adults aged 19 years or older.18 Yeongi-gun region was omitted in 2013 CHS and Sejong was not included in 2008 CHS so, our result included 252 regions only.
For SIR based PAF calculation of lung cancer due to active smoking, total lung cancer mortality rate by regions was derived from national mortality statistics database. Average lung cancer mortality of 5 years (2008–2013) was used to stabilize the data by region.19 Lung cancer mortality was zero in thirteen regions which lead to zero PAF value in these regions. This limitation of data resulted in under estimation of BOD related to active smoking in these regions. Lung cancer mortality rate for never smokers in Korea was taken from previously published Korean Cancer Prevention Study (KCPS) and the same rate was used for all regions due to lack of data at sub-national level. KCPS is a cohort study of Korean smokers and never smokers with 12 years of follow up.20
Calculation of DALY
Method and data source
As regional statistics for disease prevalence and mortality are not available in Korea, DALY at sub-national level was estimated by redistribution of national DALY to sub-national level using age and gender specific demographic structure of each region. For YLD estimation at national level, age and gender specific prevalence was taken from the Health Insurance Review and Assessment Service (HIRA) data 2013 and Korean Central Cancer Registry Database (KCCR) 2012. In contrast to the GBD study, we used disability weights from a recent Korean study which calculated DW for 228 causes.21 For YLL calculation age and gender specific deaths were derived from National Statistical Office database 2013. Method and data source for national level DALY calculation has been described in detail in the national level article.12
Calculation of BOD due to SHS among non-smokers
Firstly, burden among nonsmokers for each disease was calculated by subtracting current smoking burden from total BOD by the following equation:
Where BNS is BOD among nonsmokers, B is the total BOD for both non-smokers and smokers, PAFcs is the population attributable fraction of active smoking, and PCS is the active smoking prevalence by gender, age and region.
Secondly, BOD attributable to SHS among non-smokers for each disease was calculated as:
Finally, total BOD attributable to SHS among non-smokers at each sub-national level was calculated by sum of all the person's SHS DALY at that region. Gender and age standardized DALY/1,000 by region were calculated using national population 2013 as the standard.
RESULTS
Prevalence of SHS exposure among nonsmokers at sub-national level
Median of SHS prevalence was highest in Jeju-do and lowest in Jeollanam-do. Generally, prevalence of SHS was higher in big cities as compared to smaller towns and rural areas. Range and median of SHS prevalence by gender and region is shown in Fig. 1. Among men, median was highest in Incheon and in women, it was highest in Jeju-do. Median of SHS prevalence was higher in men than women in most of the regions except Jeollanam-do and Jeju-do.

A map showing prevalence of SHS exposure at sub-national level is provided in Fig. 2. Prevalence of SHS exposure among nonsmokers ranged from 35% in Gwangju (Gyeonggi-do) to 6% in Wonju; Jangseong-gun; Goheung-gun; Gurye-gun and Dong-gu, Ulsan. The top three regions with highest SHS prevalence were located in Gyeonggi province. Among men, SHS prevalence ranged from 47% in Buk-gu, Ulsan region to 4% in Gurye-gun region in Jeollanam-do province. SHS Prevalence in women ranged from 34% in Gwangju to 4% in Dong-gu, Ulsan.

SHS burden at sub-national level
BOD as total DALY
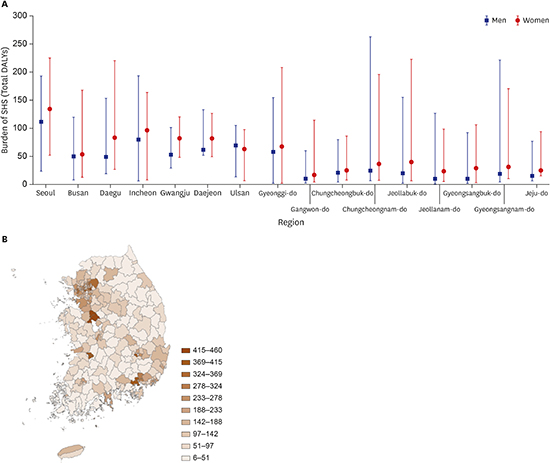
Median of DALY was highest in districts of metropolitan cities and lowest in small towns and rural areas. Median of SHS burden was highest in Seoul and lowest in Jeollanam-do. Range and median of SHS burden as DALYs by region and gender is shown in Fig. 3A. Median of BOD was highest in Seoul for both men and women. Median was higher in women than men in all the regions except Ulsan. There was very little gap between range and median of SHS burden of men and women in all the regions.
Fig. 3
Second-hand smoke burden range by gender and administrative region (unit: total disability adjusted life years).

A map showing BOD at sub-national level is provided in Fig. 3B. SHS burden ranged from 460 DALYs in Cheonan to five DALYs in Songtan, Pyeongtaek region. Seven out of the top fifteen regions with highest BOD in terms of DALYs were located in Seoul. In men, total DALYs ranged from 263 DALYs (Cheonan) to one DALYs (Gurye-gun, Jeollanam-do. In women, total DALYs ranged from 225 DALYs (Songpa-gu, Seoul) to two DALYs (Songtan, Pyeongtaek).
BOD per 1,000
In contrast to total DALY/1,000 was higher in small towns and rural areas as compared to big cities. Median was highest in Jeju-do and lowest in Gwangju. Range and median of SHS burden/1,000 by gender and region is shown in Fig. 4A. Median was highest in Jeju-do for both men and women. Women had higher median in all the regions except Incheon and Ulsan in which men were higher.
Fig. 4
Second-hand smoke burden range by gender and administrative region (Unit: disability adjusted life years per 1,000).

Burden of SHS at sub-national level per 1,000 is shown in Fig. 4B. DALY per 1,000 was highest in Seogwipo (west) in Jeju-do (2.21/1,000) and lowest in Dong-gu, Ulsan (0.18/1,000). Twelve out of fifteen regions with highest DALY per 1,000 were small towns and rural areas. BOD/1,000 ranged from 2.10 (Buyeo-gun) to 0.11 (Gurye-gun, Jeollanam-do) in men and 2.60 (Seogwipo, west in Jeju-do) to 0.13 (Dong-gu, Ulsan) in women.
Gender and age standardized BOD per 1,000
Median of gender and age standardized DALY was higher in big cities but the gap between medians of different regions was very small. Gender and age standardized DALY per 1,000 median was highest in Jeju-do and lowest in Jeollanam-do. Range and median of SHS burden as gender and age standardized DALY/1,000 by gender and region is shown in Fig. 5A. Median was higher in women than men in all regions. Median of burden was highest in Jeju-do for both men and women.
Fig. 5
Second-hand smoke burden range by gender and administrative region (Unit: gender and age standardized disability adjusted life years per 1,000).

Burden of SHS at sub-national level in terms of gender and age standardized DALY per 1,000 is shown in Fig. 5B. Gender and age standardized DALY per 1,000 was also highest in Seogwipo (west) in Jeju-do (1.66/1,000) and lowest in Dong-gu, Ulsan (0.17/1,000). Gender and age standardized DALY in men was highest in Cheonan (1.84/1,000) and lowest in Jeollanam-do Gurye-gun (0.12 per 1,000). Gender and age standardized DALY in women was highest in Seogwipo west in Jeju-do (1.84/1,000) and lowest in Dong-gu, Ulsan (0.11 per 1,000). BOD by gender at sub-national level in terms of DALYs is shown in Supplementary Table 1.
DISCUSSION
According to our study, there was wide variation of SHS related burden among regions at the sub-national level. Many previous studies indicate that active smoking and SHS prevalence is affected by a number of regional contextual factors including local culture, socioeconomic status, and smoking ban policies.222324 A recent study in Korea also explored the effects of various regional factors on SHS exposure and found that prevalence varied according to different local factors.8
Generally, prevalence of SHS exposure among nonsmokers was higher in big cities as compared to small towns and rural areas. A recent Korean study also showed that living in an urban area was positively associated with SHS exposure.8 Most of this prevalence is due to workplace exposure to SHS. People living in big cities are office workers and exposed more to SHS as compared to rural areas. Prevalence of SHS exposure is more in younger age groups as compared to older people.25 Big cities usually have a larger proportion of younger population as compared to rural areas resulting in an increased SHS exposure. Additionally, overcrowded places and more social interaction among people also result in increased SHS exposure in urban areas.
Our results show that SHS burden in different regions was not related to SHS prevalence only. Many regions had higher SHS prevalence but lower burden and vice versa. These findings were due to the fact that SHS burden was dependent not only on SHS prevalence and PAF but also on total DALY and nonsmoker DALY in a specific region. Prevalence of SHS exposure may be high in a specific region but nonsmoker population and DALY may be low due to high active smoking prevalence resulting in lesser disease burden. Total population of a region was also an important factor effecting total BOD. In order to adjust for these differences of population size, gender and age structure at sub-national level, three indices of BOD were calculated including total DALY and gender and age standardized DALY.
Our results indicated that SHS exposure among nonsmokers and BOD in terms of total DALY was predominantly higher in large cities while BOD per 1,000 was higher in small towns and rural areas. This finding can be explained by population size of regions. Large cities have higher SHS prevalence and high total DALY due to big population size resulting in high burden in terms of total DALY. Small number of total population in towns can be the reason for fewer DALYs in these areas.
BOD became higher in small towns and rural areas after adjusting the results for population size in terms of DALY per 1,000. This finding can be explained by the specific age and gender structure of urban and rural areas. Korea is a country with high number of elderly population accounting for 11.9% of total residents in 2013.19 According to GBD report 2013, DALY was highest in elderly population (65 years and over) in Korea.26 Elderly population rate is high in these rural areas, which cause more disabilities contributing to increase in disease burden in these areas. Many previous studies proved that uptake and utilization of screening services is very low in rural areas2728 which can also lead to increase in both fatal and nonfatal disease burden in these areas. Therefore, it can be inferred that BOD as total DALYs is high in large cities but probability of suffering is higher in rural areas. Therefore, policy makers should focus not only on the areas with high SHS prevalence but also on the rural areas and small towns in which low prevalence is causing greater disease burden. Along with control of SHS exposure, early diagnosis and proper screening of related diseases especially in elderly population can also help to control the burden by reducing disability and early fatality. Health education programs about significance of disease screening and early diagnosis should be implemented especially focusing small towns and rural areas.
Gender and age standardized DALY per 1,000 was calculated after adjusting the results for population size and demographic structure. Gender and age standardized DALY showed a mix picture of BOD for urban and rural areas and the difference between medians of BOD was very small. These findings show that disease burden depends on other local factors and regional situation as well. Planning and priority settings for smoking ban policies and their extent of implementation in each region are important elements affecting the health outcomes.
Our study has a few limitations. First, for PAF calculation of lung cancer due to active smoking at sub-national level, total lung cancer mortality rate at sub-national level was derived from national statistics data, which showed no mortalities for few regions, which may have resulted in inaccurate estimation of smoking burden in those areas. Second, the same never smoker lung cancer mortality rate at national and sub-national level was used for PAF calculation of lung cancer due to active smoking which may not depict the accurate status in each region. Third, sub-national DALY was calculated by redistribution of national DALY due to lack of disease prevalence and mortality data by each region. This indirect method may have created ambiguity in the results. Finally, we could not include children and adolescents, the most vulnerable victims of SHS exposure. Further studies based on sub-national data are needed to evaluate the exact BOD in each area.
In conclusion, there were substantial variations between regions according to disease burden. In addition to SHS prevalence, BOD among non-smokers was associated with many other factors like prevalence of active smoking, population size and age structure in each region. Total DALY was higher in large cities while DALY per 1,000 was higher in small towns and rural areas. These results are due to big population size in cities and high number of elderly population in small regions. So, more resources should be allocated in big cities for control of active smoking and SHS prevalence by formulating policies according to each location and gender. Resources in small towns and rural areas need to be allocated more towards implementation of screening programs, early diagnosis and treatment of diseases especially in elderly population. People should be educated about SHS related health threats and importance of health screening programs with more focus on rural areas. Gender and age standardized DALY per 1,000 was higher in both small towns and large cities which show that local regional policies have effect on BOD control. Regional governments should implement smoking policies according to specific situation in each region and regular evaluation of preventive policies by calculating BOD should be done to assess their effectiveness.
 XML Download
XML Download