

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Carbapenem-resistant Enterobacteriaceae (CRE) have been successfully spread worldwide in a relatively short period of time.1234 Among the CRE, carbapenemase-producing Enterobacteriaceae (CPE) show a high rate of transmission due to the synergy of highly efficient plasmids and strains with good clonal expansion such as sequence type 258 (ST258).2
Since 2011, Korean Centers for Disease Control and Prevention (KCDC, Cheongju, Korea) has begun receiving formal CRE reports from selected hospitals. From that point, data that was properly structured began to be collected.5 Since then, the number of reports has risen sharply and is suspected to have spread nationwide by 2015, and there is a concern that the trend toward endemicity will soon be established. Therefore, before this endemic, CRE should be blocked as much as possible and be seriously dealt with. This review will describe various aspects of how to cope with the CRE problem.
THE BASICS
Carbapenem is born to endure most beta-lactamases because
Carbapenem could be categorized as a kind of beta-lactamase inhibitor by birth because it is a descendant of olivanic acid extracted as the first beta-lactamase inhibitor in 1976 with clavulanic acid.6 Thienamycin from Streptomyces cattleya has an ethoxy (hydroxyethyl) group attached to the 6th carbon, and the first sulfur is replaced with carbon (C1), unlike the beta-lactam basic structure. And a bond between carbon 2 and carbon 3 is unsaturated, i.e., a double bond (Fig. 1). If the bond is saturated, it is a penam structure, but because it is an unsaturated bond, it becomes a penem. The carbon located as the first carbon instead of sulfur (carba-) and a double bond (penem) gave the name ‘carba + penem = carbapenem’ to this structure. The steric hindrance due to the presence of hydroxyethyl groups makes carbapenem stable to most beta-lactamases except carbapenemase.
Fig. 1
The carbapenem stemmed from the primitive beta-lactamase inhibitor, olivanic acid. The hydroxyethyl group (blue circle) in its structure makes the carbapenem stable to the enzymatic inactivation of most beta-lactamases except carbapenemase (every chemical structure in this paper is drawn by using the freeware ACD/ChemSketch 2017.2.1 file version C40E41, Build 99535, 15 Feb 2018, Advanced Chemistry Development, Inc.).

CRE
According to the Centers for Disease Control and Prevention (CDC, Atlanta, GA, USA) definition, CRE are defined as any Enterobacteriaceae which are resistant to any carbapenem or are documented to produce a carbapenemase.7 The major resistance mechanisms are summarized as enzymatic inactivation, efflux pump, and target site alteration (e.g., loss of porin).8 Among the CRE, the bacteria that inhibit carbapenem by encoding inactivating enzymes are CPE. Since the mechanism of spreading CPE is transposon- and plasmid-mediated, the transmission rate is superior to those of non-CPE and the resistance by CPE is substantially the majority of CRE.2
Carbapenemases are categorized into serine-protease and metallo-beta-lactamase (MBL)
Carbapenemases belong to the Ambler class A, B, and D. Class A and D carbapenemases have serine residues in their active sites and hence are called serine-proteases, while class B enzymes are MBLs.91011
The class A carbapenemases include Klebsiella pneumonia carbapenemase (KPC 2-13), imipenem-hydrolyzing beta-lactamase (IMI 1-3), and Guiana extended spectrum (GES 1-20). Of these, KPC-producer is the most prevalent one and shows propensity to be multidrug-resistant. Class D carbapenemase is poorly inhibited by clavulanic acid, while Class A is partially inhibited.12131415 The main class D enzyme is oxacillin hydrolyzing (OXA). As it has a tendency to be frequently mutated, it produces a lots of variants (e.g., OXA-48, 23, 58, etc.).
Class B MBL has zinc ions in its active site of the enzyme, therefore it is inhibited by ethylene diamine tetraacetic acid (EDTA), a chelator of zinc ion.161718 It can destroy all beta-lactams except monobactam. New Delhi Medical (NDM-1), imipenem-resistant Pseudomonas (IMP), Verona integrin-encoded metallo-beta-lactamase (VIM), and Seoul imipenemase (SIM)19 enzymes belong to this class.
CRE spread very rapidly and are hard to contain
CRE has a very fast propagation speed considering the rapid pace in which it has spread around the world.21120 The reason for this rapid transmission of CRE is due to the synergy of a special clone and a highly efficient mobile element. Taking KPC as an example, the transposon involved in the blaKPC
gene (Tn4401) plays a major role. Tn4401 shows high frequency of transposition ability.21 In addition to advantageous conditions of active and highly efficient transposons, they are placed on self-transferable plasmids, which enter into an efficient sequence type, such as ST258. As a result, the resistant genes spread to various bacterial species.2 OXA is encoded from the blaOXA-48
gene which is closely related with IncL/M type plasmids irrespective of ST type.22 The main risk factors for acquisition of CRE are immune suppressed state, advanced age, admission to intensive care unit, patients under mechanical ventilation, previous exposure to antimicrobials, transplantation, prolonged hospital stay, etc.23
CRE are really harmful
There have been a number of reports that patients with CRE showed a higher mortality and morbidity than those without.24252627282930 In patients with CRE, neutropenia, multiple organ dysfunction, respiratory failure, inappropriate antimicrobials, high severity score, and tigecycline therapy were independently associated with higher mortality.2425 Although resistance does not always mean high virulence, it seems clear that infection or colonization of CRE is overtly a bad prognostic factor.
CRE are already worldwide
CRE has been rampant worldwide since its first emergence in the 1980s. KPC-producing Enterobacteriaceae are now endemic in United States, Colombia, Argentina, Greece, and Italy. OXA-48-producers are endemic in Turkey, Malta, Middle-East (Lebanon, the Sultanate of Oman, Saudi Arabia, Kuwait) and North Africa (Algeria, Egypt, Libya, Morocco, Tunisia), while NDM-1 producing organisms have established endemicity in India, Pakistan, and Sri Lanka.3420 If so, what about in Korea?
Korea could encounter endemicity of CRE before long
It is true that the number of CRE cases is growing rapidly in Korea as of 2018. CRE was first reported in 2008 and was a sporadic case,31 but it was the first signal to warn of impending CRE propagation. So the KCDC started sampling surveillance for about 100 institutions from 2011, and 16 cases were confirmed that year. However, 565 cases were reported in 2015, 1455 cases in 2016, 5716 cases in 2017, and 6770 cases as of August 2018.5 What a steep rise!
The most worrisome and attention-grabbing part for the medical and health government now is whether or not the CRE is now settled (endemic) in Korea. If it is true that the CRE has successfully settled in Korea, it means that complete removal is no longer possible. Two molecular epidemiologic studies on CRE from 60 selected hospitals have shown that the main carbapenemases in Korea are OXA-232 and KPC-2.32 These reports also revealed that a few dominant CRE clones (epidemiologically related) were already spread inter-regionally.3233 According to the standard of epidemiological stages presented by CRE research centers in Europe, the epidemiological stage of CRE in Korea is at least in the stage 4, inter-regional spread.34 Now then, can we say that Korea is in the stage 5 (endemic)?
Endemicity is not officially confirmed because it has to be proven that CRE is isolated in almost all hospitals in Korea to meet the stage 5 criteria. So we cannot conclude that it is endemic yet, at least as of 2018. However, it is also true that endemicity is suspected. When the nationwide survey ongoing by the KCDC will expand to reach a level that can represent nearly all hospitals in Korea, I expect that the time to officially declare endemicity is not too far.
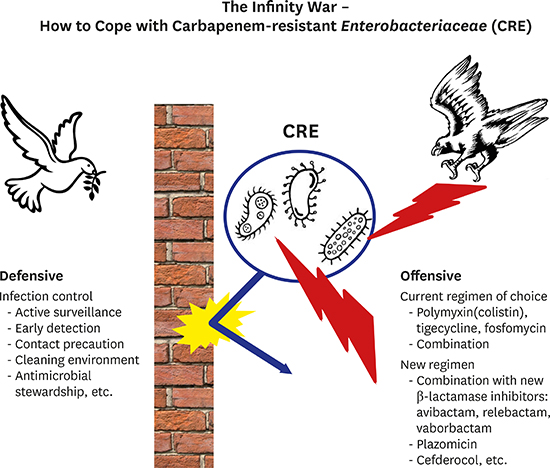
HOW TO COPE WITH CRE
The principle of how to cope with CRE is as follows: When colonization with CRE occurs, the spread must be blocked by strict infection control. If the CRE is cultured from a normally sterile specimen, e.g. blood, or if it is a clinically significant disease caused by CRE, we should attack CRE with appropriate antibiotics. So I subjectively categorize the coping principles for CRE as two broad measures: defensive and offensive (Fig. 2).

Infection control as defensive measures
When you start infection control measures against CRE, you would frequently meet another resistance not by the bacteria but by humans. That's because various limitations and regulations are necessarily imposed on health-care personnel as well as the patients. Thus, the medical director who is in charge of the infection control committee should moderate all possible conflicts and problems that can be caused by the procedures.
The key component of the infection control is blocking the transmission of CRE. To achieve this, hand hygiene is the most important norm that every health-care personnel has to comply with. Active surveillance and early detection, enhanced contact precautions, cohorting staff, environmental control, and antimicrobial stewardship are also essential to the adequate infection control program.3435
Prevention of entry to a hospital is a critical step at the beginning
While CRE are often detected among hospitalized patients, it is more important that they are introduced from outside the hospital.363738 Therefore, it is a very crucial step to block them before the admission to hospital. According to the KCDC guideline, if a patient has visited a medical facility in an area of high prevalence of CRE within a year, or if a patient has had previous experiences with CRE or had contact with CRE patients within 12 months, performing a rectal swab as a selective CRE screening is recommended, and pre-emptive isolation is performed until results are obtained.39 The reason for the premise of 'within 1 year' is based on the experts' opinion, but this is also supported by a report that the period of maintaining the colonization state even after discharge is around one year.40
If the screening test is positive for CRE, initiate an enhanced contact precaution while carrying out a detection test for carbapenemase, such as a modified Hodge test, and the result should be reported to the municipal health section as well as to the health center in the district.39414243444546 However, even if the result of the screening test is negative, it is recommended that an additional test is performed at intervals of one day or more from the first day of the test, and the entry is allowed only after confirming the negative two consecutive times.39
The contact precaution should be strictly done
Isolation and contact precautions should be strictly performed. In particular, strengthen the hand hygiene of employees. Overall disinfection should be performed on the environmental surfaces in the room, and surfaces and equipment in frequent contact areas should be cleaned on a daily basis.35394748
The patients should be isolated in a single room and cohorting is considered if the available room is insufficient. Cohorting means not only geographic cohorting to segregate patients, but also staff cohorting to place dedicated staffs assigned only to care for the isolated or cohorted patients during a shift, although there are many limitations. The patient must be in the single or cohort room and can leave the room only for medically necessary reasons with a gown and gloves, and should be accompanied by the dedicated staff. Their visitors are generally limited, and if they will visit the patient, they must wear gowns and gloves in the patient's room. In short, isolation and strict contact precaution is almost like a prison level. When will be the isolation terminated?
The KCDC guideline does not explicitly specify its criteria, but only recommends that three consecutively negative results from cultures of 3- to 7-day intervals could be a basis for determining the discontinuation of isolation.39 According to the SHEA expert guidance, discontinuation of contact precaution is recommended if at least 6 months have elapsed since the last positive culture, or if presence of a clinical infection and ongoing antibiotic use, or if at least 2 consecutive negative rectal swab samples obtained at least 1 week apart.49 Because the duration of carriage is averagely more than 1 month, testing of CRE should not be undertaken less than a month after the positive culture.50 Even if a patient is freed from isolation and is not a CRE carrier any more, there is still a chance of recrudescence or reinfection (around 10%). Therefore, testing of CRE carriage should be repeated on every new re-admission to the hospital.5152
On outbreak
If two or more epidemiologically relevant CRE occur, they are judged to be an outbreak. On outbreak, in addition to strict enforcement of contact precaution, a group infection control team should be constituted to establish epidemiological investigation and countermeasures against the outbreak. And the outbreak should be reported to the health center in the district. Educate and strengthen hand hygiene for all employees in the hospital. At a weekly interval, active surveillance cultures are extensively performed on patients, other patients who have been treated by the same healthcare worker, and patients who are vulnerable to infection. Surveillance cultures are conducted for environmental surfaces where contact is frequent, and for environments where contamination is expected to occur from the patient's secretions or excretions.39
Patients who shared the same room with a patient with CRE are regarded as a tentative carrier of CRE and are also applied contact precaution. If the CRE test results on them are consecutively negative three times in 3- to 7-day intervals, the contact precaution is discontinued. Any healthcare workers who were in contact with the patient with CRE are also included in the outbreak monitoring system. If testing of CRE is positive, they should be restricted from contacting other patients until three consecutively negative CRE results. In the worst case, so that no further containment is possible, the hospital executive should consider closure of the ward. It is advisable to limit the admission of new patients during the period of the outbreak.
If there are no more patients with CRE in the hospital and the organism is no longer identified in the active surveillance culture, the outbreak could be declared to be terminated. Within two weeks after the end of the outbreak, the hospital must submit a report on the result of the epidemiological investigation about the outbreak to the division of healthcare-associated infection control in the KCDC.39
A series of actions to be taken for managing CRE on admission, on outbreak, and occurrence from a hospitalized patient on the basis of the 2018 KCDC guideline are summarized in Fig. 3.

Antimicrobial stewardship works
In addition to effectively blocking horizontal transfer of CRE by conducting contact precautions, it is also an important infection control policy to do the proper regulation of antibiotics. This is because the reduction of antibiotic usage reduces the colonization pressure for selection of resistant organisms and consequently reduces the probability of colonization or transmission of CRE. There have been a number of reports about the successful reduction of CRE by antimicrobial stewardship.5758 It is also worth considering that carbapenem-sparing strategies are usually preferred on the treatment of patients with clinically significant CRE infection to avoid the selection.59
When it comes to a lawsuit – a medicolegal aspect
Nowadays, patients are well aware of health care-associated infections (HAI). If a patient thinks that he or she has suffered from CRE colonization or infection, the patient could file a lawsuit. The key term in medical litigation is ‘malpractice’ or ‘negligence’. Malpractice is legally defined as professional negligence by act or omission by a healthcare provider in which the treatment provided falls below the accepted standard of practice in the medical community and causes harm to the patient.60 Medical malpractice belongs to tort law that deals with professional negligence. Tort law is basically distinct from criminal law.60 Believe it or not, however, negligence with HAI are prosecuted under criminal law in Korea now.6162 And hospitals are vicariously liable for negligent or failures by staff to comply with the infection control programs.6364
The winning or losing of a lawsuit depends on proving the causal relationship between the negligence of the doctor and the damage of the patient. Currently, the courts are demanding the patient to bear the burden of proving such a strict causal relationship. However, due to the fact that it is practically difficult for the patient to prove causality, some lawyers today claim to apply the mitigation of law principles to the patient, and instead pass the burden of proof to the hospital on the basis of the German law (conversion of proving responsibility).65 Of course, it is also argued that if the burden of proof goes to the hospital, there may be cases in which the healthcare provider may be held responsible even though there is no actual causation.66
Hence, hospital executives and medical staff need to deal with this CRE infection problem as much as possible in terms of the potential medico-legal aspect as well as from the view of infection control.
The best prevention for reducing the threat of lawsuit of HAI is that hospitals should establish their infection control system (infection control committees with the assistance of the medical and hospital staff) and manage it thoroughly.67
A checklist based on the KCDC guideline39 that should be prepared by the hospital just in case of possible lawsuits of HAI or colonization by CRE is suggested in Table 1.
Table 1
A checklist of the management of infection or colonization by CRE suggested for the preparedness to the possible medico-legal suits
Offensive measures
Current therapeutic regimen
Currently, polymyxin E (colistin), tigecycline, and fosfomycin are used for the treatment of CRE, and a combination of these antimicrobials is preferred.859
1) Colistin is the therapeutic option of choice for now
Colistin was extracted from Paenibacillus polymyxa and appeared on the market in 1959, but severe and frequent nephro- and neurotoxicity precluded its use in clinical practice. However, in the 21st century, it was reappraised and eventually has become a therapeutic agent of choice for CRE.6869 Colistin has a threatening appearance that looks like an awl. Ten amino acids form an annular handle, fatty acid is plugged in it, and five methane sulfonate sodium are wrapped around by means of amine groups (Fig. 4A), hence the name colistimethate sodium (CMS) was given. While the lipophilic fatty acid plays a role as an anchor on the bacteria, the handle of ten positively-charged amino acids binds to the lipopolysaccharide (LPS) on the CRE. During the process, colistin kicks out the calcium and magnesium ions which maintain the integrity of the LPS and outer cell membrane. As a result, the outer surface of the bacteria is disintegrated and the CRE ultimately die. Colistimethate effectively kills nearly all CPE including MBL.7071

2) Tigecycline is also useful, but not appropriate for bacteremia/sepsis
Tigecycline is a semisynthetic antibiotic that has been supplemented to the minocycline structure.7273 A 9-tert-butyl-glycyl amido moiety is attached to the 9th carbon of the minocycline to make the glycylcycline (Fig. 4B). Tigecycline is not affected by the efflux pump due to its big glycyl moiety (too big for the pump to efflux) and has a five times higher affinity than that of tetracycline to the bacterial 30S ribosome.7273 This third-generation tetracycline is officially approved for the treatment of a soft tissue infection and intraperitoneal infection, and is also used in the treatment of CRE. However, as its high volume of distribution (Vd) of 7–10 L/kg suggests, tigecycline is not an adequate therapeutic option for the bloodstream infection by CRE.73
3) Fosfomycin could be a potential option, but…
High dose fosfomycin in combination with carbapenem can be a useful option for the treatment of CRE. However, there is no proven clinical efficacy yet. In fact, there are reports of clinical failures and emerging resistance to these antimicrobials and clinical studies are limited.74
4) Combination therapy is currently a mainstay of regimen
The combination of a carbapenem-containing regimen with colistimethate or tigecycline or aminoglycoside could be preferred over monotherapy for CRE.597576 At present in Korea, however, the combination regimen of tigecycline with colistin or carbapenem is always cut down because the Korean Health Insurance Review and Assessment Service (HIRA, Wonju, Korea) does not approve the regimen yet. Therefore, tigecycline should be used as a monotherapy for now.
New drugs: beta-lactamase inhibitor
The first beta-lactamase was discovered even before the first penicillin product was formally marketed.7778 Since then, the war between beta-lactam and beta-lactamase has been repeated over and over again. The core of this infinite war is the interaction between hydroxyl group of serine and carbonyl moiety. Serine in the bacterial transpeptidase (penicillin binding protein, PBP) plays an active role in the process of bacterial cell wall synthesis. The hydroxyl group of serine has a high affinity for a carbonyl group of D-alanine, the main bricks of the bacterial cell wall. By the way, as beta-lactams also have lots of carbonyl moieties, they appear structurally very similar to D-alanine from a standpoint of the serine. Hence, the serine improperly and preferentially binds beta-lactam. Once a beta-lactam and serine combine to form an acyl-enzyme complex, the complex is hardly dissociated due to slow deacylation and the cell wall synthesis is greatly hurt to culminate in the death of bacterial cells. That's the way beta-lactam works.
And bacteria take revenge on beta-lactams in the same way. The beta-lactamase attacks carbonyl groups on beta-lactam with the serine as the front attacker, just like PBP. The enzyme performs rapid acylation and rapid deacylation, which means that one beta-lactamase can inactivate many beta-lactam molecules. That's the way of resistance the beta-lactamase wields.
Now it's the beta-lactamase inhibitor's turn. Yes, the inhibitor works in the same way: its carbonyl moiety blocks the serine residue in the active site of the beta-lactamase. These infinite interactions are summarized in Fig. 5.
Fig. 5
The interaction between serine and carbonyl group makes the infinite war among β-lactam, β-lactams, β-lactamase inhibitors.
PBP = penicillin binding protein.

However, this mechanism is limited to serine protease-based carbapenemase (class A, D). In case of class B MBL, it's a different story. The MBL inhibits carbapenems through the mediation of zinc ions. Therefore, most beta-lactamase inhibitors are ineffective for the class B carbapenemases. Although colistin can deal with the MBL-producing CRE now, frequent nephron- and neurotoxicity limits the use of this agent. The development of inhibitors that effectively inactivate MBL is a dire assignment now.7980
1) The combination of avibactam with beta-lactams could be a powerful weapon
Avibactam is the first inhibitor to shift the paradigm of previous beta-lactamase inhibitors. It does not have a beta-lactam ring.81 Instead, it has a diaza-bicyclo-octane (DBO) structure as a main framework as illustrated in Fig. 6A. This heterocyclic core is the main nucleophilic acylator to attack serine-based carbapenemase. It shows reversible inhibitor unlike the previous inhibitors. Hence one molecule of avibactam can be recycled and can inactivate a number of carbapenemase molecules almost indefinitely, which makes avibactam a much better and more efficient inhibitor than previous beta-lactamase inhibitors. A 4: 1 combination of ceftazidime with avibactam has expanded the original spectrum of ceftazidime and showed effective inhibition of KPC, AmpC, and OXA-48 (partially). But it is not effective for MBL.818283848586 Another combination with ceftaroline fosamil has a similar spectrum of activity.
Fig. 6
New beta-lactamase inhibitors with non-beta-lactam structure and monobactam. (A) Avibactam; (B) The sulfonate group of aztreonam (monobactam) interacts with the zinc binding site of the MBL. As a result, MBL is too far away to reach the monobactam moiety; (C) The boronic moiety of vaborbactam (bigger square) preferentially attacks the hydroxyl group (smaller square) of serine protease; (D) Addition of piperidine ring to the avibactam makes relebactam.
MBL = metallo-beta-lactamase.

Aztreonam intrinsically endures the MBL because the sulfonate bound to the monobactam ring interacts with the zinc binding site of the MBL and the active site of the enzyme is too far away to reach the monobactam ring as illustrated in Fig. 6B.86 Together with the spectrum of activity of avibactam, aztreonam/avibactam could be a promising agent.
2) Vaborbatam-meropenem uses boronic acid to inactivate carbapenemase
Vaborbactam is also an inhibitor that does not have a beta-lactam ring. The key component is the boronic acid in the structure, which reacts with the serine in the active site of carbapenemase to inactivate it (Fig. 6C). Its combination with meropenem is effective on class A (KPC), class C (AmpC), and class D OXA, but no effect is expected on class B MBL such as NDM-1.87
3) Relebactam-imipenem/cilastatin shows steric hindrance of efflux pump as well as inhibition of carbapenemase
In the avibactam structure, the addition of the piperidine ring to the carbonyl group of the second carbon makes relebactam (Fig. 6D). As a result, relebactam can show steric hindrance of the bacterial efflux pump as well as the ability to inhibit carbapenemase based on serine-protease. Combination of relebactam with imipenem/cilastatim is under clinical evaluation.88
New drugs: other than beta-lactamase inhibitor
1) Plazomicin could fight with CPE which produce serine-carbapenemase.
Plazomicin is derived from sisomicin. In the structure of the sisomicin, hydroxy aminobutyric acid (HABA) was added at the first carbon and hydroxyethyl group was added to the amino sugar (Fig. 7A). It has been reported that combination of plazomicin with ceftobiprole or daptomycin can treat methicillin resistant Staphylococcus aureus, even vancomycin-resistant S. aureus, and could be effective against CRE.8990
Fig. 7
The structure of new antimicrobials other than beta-lactamase inhibitors: (A) The schematic structure of plazomicin (HABA). (B) The chemical structure of cefiderocol (left) with catechol moiety (square).
HABA = hydroxy aminobutyric acid.

Since CRE is fundamentally resistant to carbapenem, it should theoretically be independent of aminoglycoside. However, aminoglycosides are often not effective in CRE, too. The reason for this is that CRE also has a gene that makes aminoglycoside modifyng enzyme (AME) as well as a carbapenemase gene. Unlike other aminoglycosides, plazomicin is not affected by AME. Thus, plazomicin can demonstrate an excellent therapeutic effect on CRE.90 But it is not effective on the MBL-producing CRE. The CRE with the NDM-1 gene also possesses the Arm/Rmt (aminoglycoside resistance methylase/ribosomal RNA methyltransferase) gene which showed resistance to plazomicin. When the bacterial rRNA is methylated by this gene, plazomicin cannot work effectively on this CRE.91929394
2) Cefiderocol, a Trojan horse
Cefiderocol is a siderophore cephalosporin, which is worth noting. The structural formula has a catechol moiety, which acts as a siderophore for iron (ferric) capture (Fig. 7B).95 From the viewpoint of bacteria, cefiderocol is regarded as a siderophore rather than an antibiotic. Thus, cefiderocol easily passes through the bacterial iron transport system while cheating the bacteria, and kills them all. So it is also called a Trojan horse cephalosporin. Cefiderocol has a potent activity against CRE and non-fermenting bacteria.9697
SUMMARY
The current trend of CRE occurrence in Korea suggests that endemicity is about to come. Therefore, it is necessary to prepare a thorough measure against impending CRE disaster. It is important that every hospital should implement a proper and thorough infection control system to cope with this phantom menace of CRE. When you meet a patient with clinically significant CRE infection, you should be prudent to administer the proper regimen of antibiotics. While colistin, tigecycline, and various combinations with carbapenem-containing regimen are the mainstay of the current therapeutic option, new antimicrobials such as avibactam, plazomicin, or siderophore cephalosporins are promising.
 XML Download
XML Download