

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vesicoureteral reflux (VUR) is one of the most common urologic abnormalities in children,1 and it is diagnosed in about one-third of children with a urinary tract infection (UTI).2 VUR in children with UTI can result in renal scarring, hypertension, and renal failure.345 Antibiotic prophylaxis and surgical correction of VUR were the mainstay treatments of VUR, until the advent of endoscopic surgery (ES). ES has been gradually evolving since the endoscopic subureteric bulking agent injection technique was introduced in 1981.6 After approval by the Food and Drug Administration in the United States, dextranomer/hyaluronic acid copolymer (Dx/HA) injection became more popular and proved to be a reliable option in all cases of low-grade VUR.37 The advantages of ES over open surgical options include its minimally invasive nature with decreased morbidity and hospital stay, as well as its perceived technical simplicity.89 Some authors even recognized Dx/HA injection as a first-line option for all grades of VUR.101112
However, the major disadvantage of the ES is generally considered to be its lower success rate than the open technique, especially in high grades of reflux.7 In a meta-analysis of endoscopic therapy in 8,101 ureters, primary success rates were 78.5% for grades I and II, 72.0% for grade III, 63.0% for grade IV, and 51.0% for grade V reflux.7 Another downside of ES is its decreased long-term durability. Lee et al.13 demonstrated a 1-year total success rate of 46.1%. No difference in the success rate between subureteral injection technique (STING) and hydrodistention implantation technique (HIT) was observed on postoperative 1-year voiding cystourethrography (VCUG). Furthermore, recurrent dilating reflux (grade ≥ 3) was seen after 2 years in 20% of patients who had been previously considered to be cured after 1 or 2 injections in the Swedish Reflux Trial.14 Since most other series on ES have reported success rates at 3 months, data on long-term success rates are lacking.8 Similarly, further investigation of the rates of UTI and other complications of reflux nephropathy such as renal scarring after ES is necessary. Therefore, this study aimed to report data on long-term success rate, postoperative UTI, and renal scarring and to evaluate the predictive factors for successful outcomes after ES in pediatric patients with VUR.
METHODS
Patients
We retrospectively reviewed 73 patients (110 ureters) under the age of 20 years who underwent ES for VUR at our institution between 2007 and 2014. We obtained approval from our institutional review board for this study. The indication of ES was persistent VUR or breakthrough febrile UTI after antibiotic prophylaxis, renal scarring, poor compliance to medication, and parental preference. The exclusion criteria for this study included a duplicated system, history of previous injection therapy for VUR, secondary VUR after previous surgery, and neurogenic bladder dysfunction. Detailed medical history of the patients including antibiotic use, preoperative UTI, presence of bladder bowel dysfunction, age at operation, date of operation, grade of reflux, laterality, differential renal function (DRF), and incidence of cortical defect was collected and analyzed.
Bulking agents and surgical technique
Two bulking agents were used for ES: Dx/HA and polydimethylsiloxane. The employed injection technique was either STING as described by O'Donnell and Puri15 and Puri et al.,16 or HIT, which is an intraureteric injection at the 6 o'clock position of the ureteral floor, often followed by a subureteric injection.12 Intraoperative findings including the shape of the ureteral orifice, lateralization of the orifice, hydrodistention grade (0 to 3), injection methods, injected volume of the bulking agent, and mound shape after injection were reviewed.
Outcome measures
Renal and bladder ultrasonography (US) was performed 1, 3, and 12 months postoperatively. A single pediatric urologist retrospectively reviewed the US images and identified the Dx/HA mounds. The volume of the mound was measured using the equation 4/3 π × length/2 × width/2 × height/2. Antibiotic prophylaxis continued after injection until the resolution of VUR was confirmed by VCUG performed 3 months postoperatively. If VUR persisted, the VCUG was repeated after 1 year. Additional ES or ureteroneocystostomy (UNC) was performed in selected patients according to the surgeon's decision after discussion with the patient or the parents. Primary success was defined as the absence of VUR in the treated moiety at the first VCUG. The association between primary success and pre- and intra-operative variables was analyzed. Parameters representing long-term renal function, such as newly developed renal scarring or DRF, were measured by dimercaptosuccinic acid (DMSA) renal scan, which was performed at least 12 months after ES. Renal functional deterioration was defined as the appearance of new renal scarring or a decrease in DRF of more than 5% after ES. Factors predictive of renal function deterioration or febrile UTI after ES were analyzed.
Statistical analysis
For comparisons between groups, the χ2 or Fisher's exact test was used for qualitative variables, while the Mann-Whitney test was used for quantitative variables. Binary logistic regression analysis was performed in the multivariate analysis. All reported P values are two-sided, and P < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 18.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Asan Medical Center (approval No. 2017-0373). The requirement to obtain a written informed consent was waived by the Institutional Review Board of the Asan Medical Center because our study was retrospective research based on medical records, and this research presented no more than minimal risk of harm to subjects.
RESULTS
Patient demographics
The demographic data of the 73 patients (110 ureters) are listed in Table 1. Sixty-one percent of the ureteral units had grade III to V VUR. Only 1 ureteral unit had no prior VUR diagnosed by VCUG; however, during the ES for contralateral grade IV VUR, the surgeon decided to perform an injection to the ureter because the ureteral orifice was opened in the shape of a stadium with grade I hydrodistention. Among the 27 male patients (44 ureters), 5 underwent concomitant circumcision.
Table 1
Characteristics and demographic data according to renal units
Values are presented as number of patients (%) or mean (range) not otherwise specified.
UTI = urinary tract infection, BBD = bladder bowel dysfunction, CAP = continuous antibiotic prophylaxis, VUR = vesicoureteral reflux, DRF = differential renal function, Dx/HA = dextranomer/hyaluronic acid copolymer, IQR = interquartile range.
aPreoperative DRF value is presented as mean (IQR).
Factors associated with primary success
The mean follow-up duration was 36.3 (median 24, range 12–118) months. A 65.6% success rate by ureter (72/110 ureteral units) and a 67.1% rate by patient (49/73 patients) were achieved. The success rate in relation to the degree of reflux was 78.9% in grade I, 87.0% in grade II, 62.5% in grade III, 37.5% in grade IV, and 66.7% in grade V. A second endoscopic injection was performed in 8 ureteral units, and complete resolution of VUR was achieved in 4 of them, which resulted in a success rate of 69.0%. After a third injection in one ureteral unit with grade II VUR, the complete resolution rate was 70.0%. Eleven patients (15 ureteral units) underwent open UNC after failed ES. Primary success or failures for pre- and intra-operative factors are listed in Table 2. The VUR grade, hydrodistention grade, shape of mound at the time of injection, and mound detected at the first postoperative US were statistically significant factors for the prediction of primary success in the univariate analysis (χ2 test and independent t-test). The correlation between the intraoperatively injected volume of the bulking agent and the measured volume on the postoperative US was low and not significant (correlation coefficient, 0.283; P = 0.057). In a multiple binary logistic regression analysis, the significant predictive factors for primary success were VUR grade (odds ratio [OR], 0.28; 95% confidence interval [CI], 0.137–0.51; P < 0.001) and detection of a mound at the first postoperative US (OR, 13.53; 95% CI, 3.13–58.52; P < 0.001).
Table 2
Primary success or failure after initial ES for each clinical parameter

Values are presented as number of patients (%) or mean ± SD.
ES = endoscopic surgery, UTI = urinary tract infection, BBD = bladder bowel dysfunction, VUR = vesicoureteral reflux, DRF = differential renal function, Dx/HA = dextranomer/hyaluronic acid copolymer, STING = subureteric injection technique, HIT = hydrodistention implantation technique, US = ultrasonography, SD = standard deviation.
Long-term outcomes
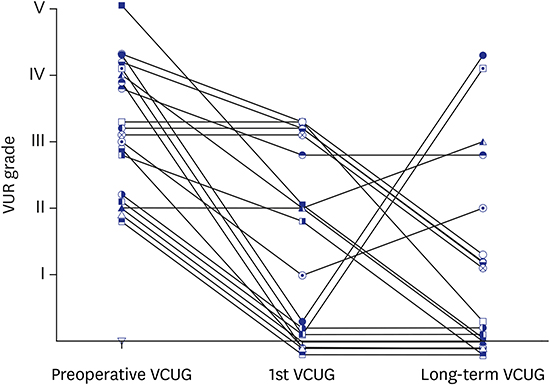
Long-term follow-up VCUG at mean 35.4 (median 27, range 12–88) months after the first ES was performed in 22 ureteral units, excluding units that underwent UNC. The long-term success rate was 59.0% (13/22). Among 9 failed units, 2 (22.2%) showed recurrence of VUR from grade 0 to IV, 1 (11.1%) showed persistent grade II VUR, and 2 showed aggravation of VUR (grade I to II and grade II to III) (Fig. 1).
Fig. 1
Spaghetti plot of VUR grade changes between preoperative VCUG, first VCUG, and long-term VCUG.
VUR = vesicoureteral reflux, VCUG = voiding cystourethrography.

Postoperative febrile UTI developed only in 1 female patient with preoperative grade IV VUR that was resolved at the first VCUG and was then found to have progressed to grade IV at the time of the UTI (67 months after the operation). After excluding 15 ureteral units that underwent open UNC after failed ES, long-term follow up with DMSA renal scans was performed in 52 ureteral units (54.7%). The mean duration to the long-term DMSA scan was 39.7 (median 30, range 12–119) months. Renal function deterioration was found in 8 (15.3%) ureteral units, and it was less common in those with primary success than in those who experienced failure (9.5% vs. 40.0%; P = 0.035). Renal function deterioration (8 units) and febrile UTI (1 unit) were less frequent in those with a detectable mound at the first postoperative US than in those without it (4.2% vs. 25.9%; P = 0.053) (Table 3). Among the ureteral units that experienced renal function deterioration or febrile UTI, 5 (55.6%) experienced primary success at the first VCUG. And 4 (50.0%) showed hydronephrosis after initial ES. However, in a multiple binary logistic regression analysis, no significant predictive factor for either renal function deterioration or febrile UTI was found.
Table 3
Factors related to renal function deterioration or febrile UTI in 52 ureteral units followed up with long-term DMSA scan

Values are presented as number of patients (%) or mean ± SD.
UTI = urinary tract infection, BBD = bladder bowel dysfunction, VUR = vesicoureteral reflux, DRF = differential renal function, Dx/HA = dextranomer/hyaluronic acid copolymer, STING = subureteric injection technique, HIT = hydrodistention implantation technique, US = ultrasonography, SD = standard deviation.
DISCUSSION
A critical weakness of ES is its relatively low success rate of 77% at 3 months after a single injection as reported in a systematic review.8 Although no randomized controlled trials have compared ES and open UNC, a resolution rate of up to 99% is expected after open surgery.17 Meanwhile, ES was reported to have a rather low success rate of 85%, even after additional second and third injections, in a meta-analysis.7 Therefore, it is most important to establish how to select the best candidates for ES. We retrospectively reviewed our consecutive data of ES cases and evaluated the predictive factors for short-term (postoperative 3 months) and long-term (postoperative median 27 months) success rates, as well as long-term renal function change.
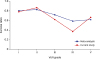
The primary success rate (67.1% per patient) in our study was comparable to that from a previous meta-analysis, which reported a 67.1% (62/114) rate per patient following a single injection in children without ureteral duplication or neuropathic bladder.7 In the present study, the trend in the resolution rate of VUR per grade also resembled the sigmoidal pattern noted in the meta-analysis (Fig. 2). Our long-term VUR resolution rate (59.0%) was disappointing, considering a success rate of 77% as reported in a previous systematic review. However, our result concurs with that of the study of Lee et al.13 in which a success rate of 46.1% was reported 1 year postoperatively, with only 74% of the initially successful cases having remained successful at 1 year. Holmdahl et al.14 also showed that 2 years after ES, the recurrence of dilating VUR was 20%. Similarly, among the 22 ureteral units that were followed up with long-term VCUG in our study, 81.8% of the initially successful cases remained successful. Moreover, in two of the failed cases, there was a substantial regression from grade 0 to IV, back to the preoperative VUR grade. Based on this result, we believe that ES is most suitable for VUR grades I to III.
Fig. 2
Line graph of primary success rates after initial ES by preoperative VUR grade. Red line indicates the pattern of the current study. Blue line is modified from the meta-analysis study by Routh et al.8
ES = endoscopic surgery, VUR = vesicoureteral reflux.
An interesting finding of this study was that mound detection at the first postoperative US was one of the two significant predictive factors for successful ES, along with the VUR grade. According to previous studies, proper mound formation such as a volcano appearance of the mound with the ureteral meatus on top was found to be a significant predictor of a successful endoscopic injection outcome.1819 We also found that the intraoperatively determined mound shape and a detectable mound at the first US 1 month postoperatively were significant factors in a univariate analysis. However, mound detection at the first postoperative US, and not the intraoperative mound shape, was the most critical factor for primary success. Since failure after successful ES is assumed to be due to the migration of deposited bulking agents,14 we suggest that a postoperatively detectable mound is a more reliable determinant in the prediction of outcomes than intraoperatively determined mound shape. Notably, our finding of no significant association between the injected volume and the measured mound volume at postoperative 1 month validates that the injected bulking agent might have lost its consistency or migrated out of the injection site during the very early postoperative period. Therefore, it is reasonable to conclude that consistent mound detection on postoperative US acts as a significant predictor of VUR resolution on postoperative VCUG.
Conversely, Zamilpa et al.20 indicated a poor association between Dx/HA mound appearance on US and VUR resolution. They found intramural mounds on US at postoperative 3 months in 65.1% of cases and reported an accuracy of 55%, a positive predictive value of 46%, and a negative predictive value of 60% for US as a test for VUR. They aimed to evaluate whether VCUG could be replaced with US and concluded that either VCUG or a nuclear medicine cystogram is necessary to evaluate VUR resolution. We agree that US is not a substitute for VCUG in the assessment of VUR resolution. Since we have utilized US at postoperative 1 month as a precautionary measure to investigate obstruction at the ureterovesical junction, the most unfavorable complication after endoscopic injection, it can act as additional valuable information for use in counseling parents and maintaining compliance with other invasive radiologic evaluations.
Notably, long-term follow-up data after ES are limited in literature.5 Lee et al.,13 Läckgren et al.,21 and Oswald et al.22 all showed a significant decline in success rates at extended follow up. Recently, the Swedish Infant High-Grade Reflux trial demonstrated that 10.3% had renal function deterioration at 1-year follow up without any difference between the ES group and the antibiotic prophylaxis group.23 In the present study, 47.2% of the cases underwent long-term DMSA follow up. We also found that renal functional deterioration was not uncommon (15.3% among 52 units with DMSA follow-up data and 8.4% in 95 units overall, excluding patients who underwent open UNC after failure of ES) and that it developed more frequently in ureters where endoscopic correction had failed (40.0%). ES contributes significantly to renal function deterioration, usually after unsuccessful surgeries, but even after the short-term resolution of VUR, which is likely due to its insufficient durability over time. Since open,24 laparoscopic,25 or robotics26 procedures have higher success rates than ES, one should contemplate carefully before deciding whether to select ES over other modalities.
There are several limitations in our study. As this study was retrospective, postoperative US was done without an intention to focus on the mound by the radiologist. This could be the reason that our mound detection rate (41.8%) was lower than that of another study in which a 79% detection rate at 2 months was reported.27 Another limitation of this study is that two different bulking agents were used in our data. However, most cases underwent Dx/Ha injection (84.5%), and the multivariate analysis for the prediction of primary success did not show differences in a subset analysis within the Dx/HA injection group; therefore, the VUR grade (OR, 0.30; 95% CI, 0.16–0.54; P < 0.001) and mound detection at the first postoperative US (OR, 3.72; 95% CI, 1.97–22.91; P = 0.002) remain significant predictors.
Our findings suggest that a successful short-term outcome of ES is expected in VUR grades I to III, especially if the mound is detected at the first postoperative US. However, the potential for unpredictable renal function deterioration and recurrence of dilating VUR in the long-term, even after a successful primary outcome, warrants continued follow up in patients who undergo ES.
 XML Download
XML Download